叶酸受体阳性循环肿瘤细胞联合肿瘤标记物检测对NSCLC诊断价值
2021-05-08秦坤金翔凤衣腾飞李烁孙昭赟刘玉洪
秦坤 金翔凤 衣腾飞 李烁 孙昭赟 刘玉洪
[摘要]目的探討叶酸受体阳性循环肿瘤细胞(FR+-CTCs)联合肿瘤标志物外周血癌胚抗原(CEA)、细胞角蛋白19片段(CYFRA21-1)检测在非小细胞肺癌(NSCLC)诊断中的价值。方法对146例NSCLC病人(肺癌组)、25例肺良性疾病病人(肺良性疾病组)和20例健康体检者(健康对照组)的CEA、CYFRA21-1和FR+-CTCs检测结果进行回顾性分析,利用受试者工作特征(ROC)曲线分析各指标诊断价值。结果肺癌组FR+-CTCs阳性率(75.3%)较健康对照组(5.0%)和肺良性病变组(8.0%)明显升高(χ2=11.412,P<0.01)。肿瘤直径和肿瘤分期是影响NSCLC病人FR+-CTCs表达的主要因素(Z=2.354,P<0.01;H=9.924,P<0.01),与病人的年龄、性别、有无吸烟史无关(P>0.05)。NSCLC组CEA、CYFRA21-1及FR+-CTCs联合检测的曲线下面积(AUC)为0.778(95%CI=0.720~0.816),诊断灵敏度为77.50%,特异度为78.08%,与CYFRA21-1、CEA联合检测(AUC=0.707,95%CI=0.660~0.756,诊断灵敏度为66.53%,特异度为71.95%)相比有更高的诊断价值。结论FR+-CTCs联合肿瘤标志物CEA、CYFRA21-1检测可提高NSCLC诊断的灵敏度及特异度。
[关键词]肿瘤细胞,循环;癌,非小细胞肺;癌胚抗原;角蛋白19
[中图分类号]R734.2[文献标志码]A[文章编号]2096-5532(2021)01-0073-04
[ABSTRACT]ObjectiveTo investigate the value of folate receptor-positive circulating tumor cells (FR+-CTCs) combined with the tumor markers carcinoembryonic antigen (CEA) and cytokeratin 19 fragment (CYFRA21-1) in the diagnosis of non-small lung-cancer (NSCLC). MethodsA retrospective analysis was performed for the results of CEA, CYFRA21-1, and FR+-CTCs of 146 patients with NSCLC (NSCLC group), 25 patients with benign lung diseases (benign lung disease group), and 20 individuals who underwent physical examination (healthy control group), and the receiver operating characteristic (ROC) curve was used to investigate the diagnostic value of each index. ResultsThe NSCLC group had a significantly higher positive rate of FR+-CTCs than the healthy control group and the benign lung disease group (75.3% vs 5.0%/8.0%, χ2=11.412,P<0.01). Tumor diameter and tumor stage were the main factors affecting the expression of FR+-CTCs in the patients with NSCLC (Z=2.354,P<0.01;H=9.924,P<0.01), which was not associated with age, sex, and smoking history (P>0.05). In the NSCLC group, the combined measurement of CEA, CYFRA21-1, and FR+-CTCs had an area under the ROC curve (AUC) of 0.778 (95%CI=0.720-0.816), a diagnostic sensitivity of 77.50%, and a specificity of 78.08%, while the combined measurement of CEA and CYFRA21-1 had an AUC of 0.707 (95%CI=0.660-0.756), a diagnostic sensitivity of 66.53%, and a specificity of 71.95%, suggesting that the combined measurement of CEA, CYFRA21-1, and FR+-CTCs had a higher diagnostic value than the combined measurement of CEA and CYFRA21-1. ConclusionFR+-CTCs combined with the tumor markers CEA and CYFRA21-1 can improve the sensitivity and specificity of the diagnosis of NSCLC.
[KEY WORDS]neoplastic cells, circulating; carcinoma, non-small-cell lung; carcinoembryonic antigen; keratin-19
据统计,肺癌是所有癌症类型中发病率和致死率最高的恶性肿瘤[1],其中占比最高的是非小细胞肺癌(NSCLC)。有研究发现,Ⅰ期肺癌病人接受手术治疗5年生存率为58%~73%,远高于肺癌总体5年生存率15%[2]。对肺癌高危人群进行低剂量螺旋CT(LD-CT)筛查,对高度怀疑肺癌的病人进行手术治疗,术后组织病理学检查显示有21.4%为良性病变[3]。组织病理学和细胞病理学为肺癌诊断的金标准,虽然其准确度高,但因为其创伤性和花费巨大,不适合作为门诊筛查的常规手段。血清肿瘤标志物可用于肺癌病人的诊斷和预后监测[4],但不同肿瘤标志物在不同病理类型肺癌病人中表达的灵敏度和特异度不同[5],且在早期肺癌病人中呈低表达,因此在早期肺癌的诊断中阳性率低。已有研究结果表明,循环肿瘤细胞(CTCs)在肺癌的诊断中具有较高的灵敏度[6],在肺癌早期就可检测到,但特异度较低。本文探讨叶酸受体阳性循环肿瘤细胞(FR+-CTCs)联合癌胚抗原 (CEA)、细胞角蛋白19片段(CYFRA21-1)在早期NSCLC诊断中的作用。
1资料和方法
1.1一般资料
收集青岛大学附属医院胸外科2018年6月15日—2019年8月15日收治肺癌病人146例(肺癌组,C组)、肺良性疾病病人25例(肺良性病变组,B组)的临床资料,肺癌组146例均为NSCLC;肺良性病变组病人中肺炎11例,肺结核7例,支气管扩张2例,错构瘤5例。肺癌、肺良性疾病病人术前经胸部CT检查证实肺部结节,术后经组织病理学或者细胞病理学检查确诊。按照国际肺癌研究协会第8版TNM分期系统进行临床疾病分期。排除标准:①重要脏器功能严重不全病人;②合并其他脏器恶性肿瘤病人;③合并严重感染性疾病病人;④合并造血系统疾病者;⑤精神异常、依从性较差者;⑥临床资料不完善者。选取同期健康体检者20例为健康对照组(A组),均接受了低剂量螺旋CT扫描,以排除潜在的胸部疾病。本文研究获得青岛大学附属医院伦理委员会批准,研究对象均知情同意。
1.2FR+-CTCs及肿瘤标志物的检测
采集受检者肘静脉血3 mL,应用配体靶向聚合酶链式反应(LT-PCR)方法检测FR+-CTCs,在3 mL血液中检测到1个叶酸受体(FR)阳性细胞定义1个叶酸单位(FU)[7],以FR+-CTCs≥8.70 FU作为FR+-CTCs阳性标准。采集肘静脉血5 mL,以2 500 r/min离心10 min,使用罗氏免疫学分析仪(德国)检测CEA及CYFRA21-1,CEA>3.4 μg/L定义为阳性,CYFRA21-1>3.3 μg/L定义为阳性。
1.3统计学处理
应用SPSS 22.0软件进行统计学处理。非正态分布计量资料以M(P25,P75)形式表示,两组数据间比较采用Wilcoxon秩和检验,多组间比较采用Kruskal-Wallis秩和检验。应用GraphPad Prism 8软件绘制受试者工作曲线(ROC曲线),计算曲线下面积(AUC)。应用Logistic回归分析比较联合肿瘤标记物检测和单独肿瘤标记物检测的灵敏度和特异度。以P<0.05为差异有统计学意义。
2结果
2.1各组 FR+-CTCs及肿瘤标志物表达比较
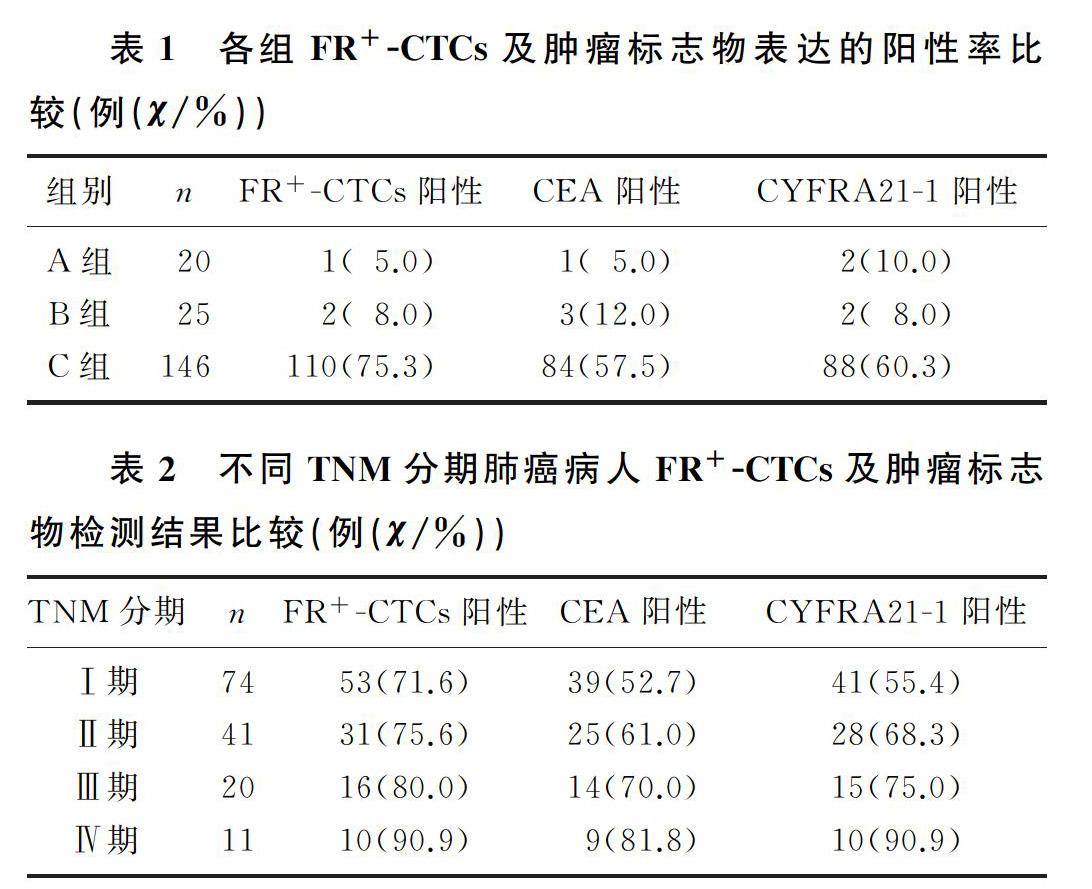
肺癌组FR+-CTCs阳性病人占比高于肺良性病变组及健康对照组(χ2=11.412,P<0.01);肺癌组CEA和CYFRA21-1阳性率与肺良性病变组及健康对照组比较差异无显著性(P>0.05)。随着肺癌分期的进展,FR+-CTCs、CEA和CYFRA21-1表达明显升高,差异有显著性(χ2=11.345~13.632,P<0.01)。见表1~2。
2.2肺癌病人FR+-CTCs影响因素
不同年龄、性别以及有无吸烟史肺癌病人的FR+-CTCs检测结果比较,差异无统计学意义(P>0.05);而最大肿瘤直径<3 cm与≥3 cm、不同TNM分期肺癌病人FR+-CTCs检测结果比较,差异具有统计学意义(Z=2.354,P<0.01;H=9.924,P<0.01)。见表3。
2.3CEA、CYFRA21-1及FR+-CTCs单独检测及联合检测对NSCLC的诊断价值
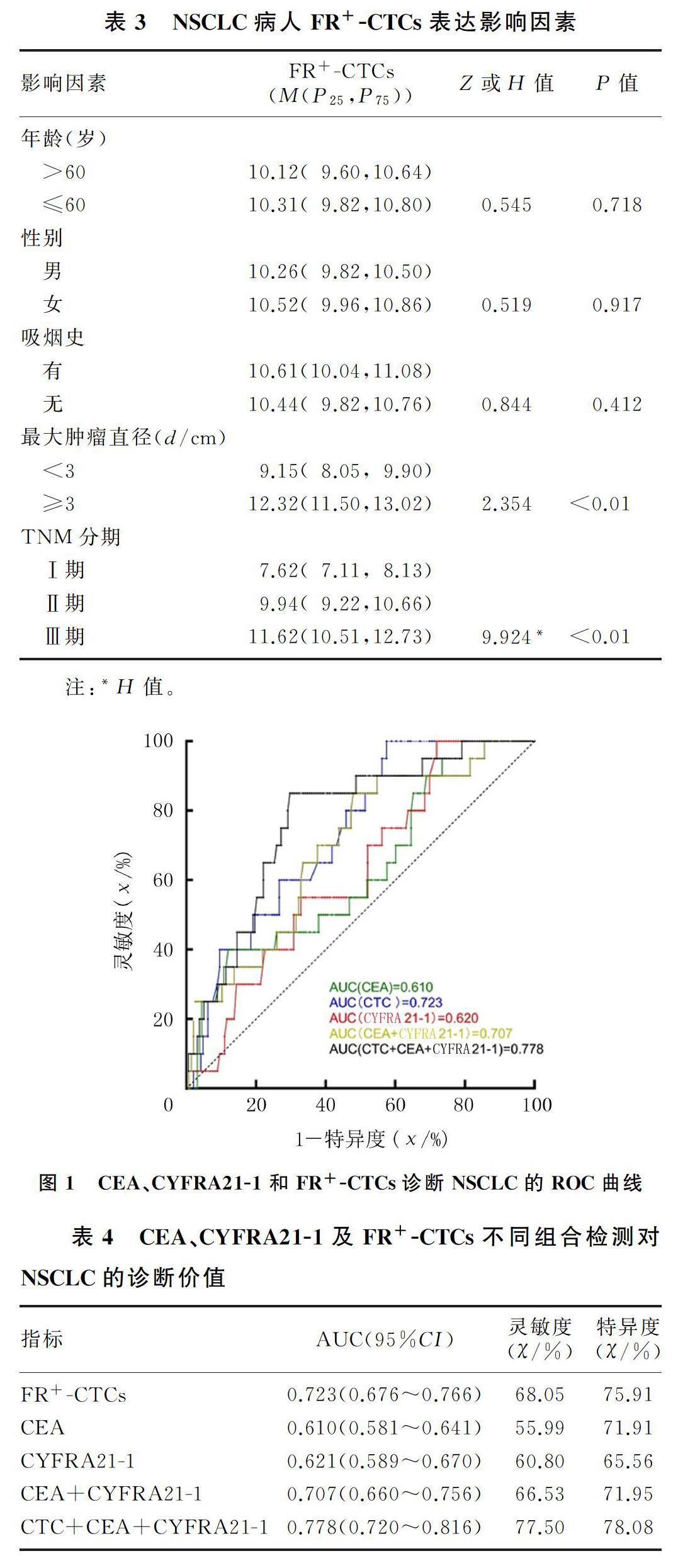
Logistic回归及ROC曲线分析显示,血清肿瘤标志物CEA和CYFRA21-1联合检测诊断NSCLC的AUC=0.707(95%CI=0.660~0.756),诊断灵敏度为66.53%,特异度为71.95%,均低于FR+-CTCs、CEA、CYFRA21-1联合检测组(AUC=0.778,95%CI=0.720~0.816,诊断灵敏度为77.50%,特异度为78.08%),但AUC值和诊断灵敏度及特异度均高于FR+-CTCs、CEA、CYFRA21-1单独检测。见图1、表4。
3讨论
ASHWORTH教授在19世纪60年代提出了CTCs概念[8],CTCs常见于恶性肿瘤病人的血液中,在良性疾病病人和健康者的血液中较少表达或者不表达[9]。细胞搜索(Cell Search)系统是第一个也是唯一一个获得美国食品和药物管理局(FDA)批准,用于除肺癌以外的乳癌、结直肠癌和前列腺癌的CTCs检测,但其应用于NSCLC病人检测阴性比例升高[10-11],需要改进检测方法来提高检测的准确度和灵敏度。
近年来,出现了一种新的检测方法,即FR+-CTCs方法。叶酸是人体必需的维生素,但人自身不能合成,需要由外界摄取。叶酸通过与细胞表面叶酸受体(FR)结合后被内吞进入细胞,在正常人的血液中,除FR活化的巨噬细胞外几乎检测不到FR的表达[12]。相反,FR在各种肿瘤细胞表面过度表达,NSCLC病人FR在CTCs表面的表达也明显升高[13-14]。在NSCLC病人中有72%~83%检测到FR阳性[15]。采用新型的LT-PCR方法检测FR+-CTCs在NSCLC病人中表达具有良好的临床应用价值。
腫瘤标志物是由肿瘤细胞产生、正常细胞缺乏或含量极微的抗原性物质,可以用于临床肿瘤筛查、预后监测及治疗效果监测等。CEA和CYFRA21-1是最早应用于NSCLC检测的肿瘤标志物[16-17],常被用来辅助诊断NSCLC病人,但其灵敏度较低,仅为20%~70%[18-19]。与CEA和CYFRA21-1相比,基于LT-PCR方法检测到的FR+-CTCs水平在诊断NSCLC时显示出较高的灵敏度[20-21],但特异度较低。因此,FR+-CTCs水平可以作为NSCLC有效的辅助诊断指标。
本文研究探讨FR+-CTCs联合肿瘤标记物检测对NSCLC诊断的灵敏度和特异度。研究结果显示,FR+-CTCs对NSCLC病人诊断的灵敏度和特异度均高于血清肿瘤标志物CEA、CYFRA21-1,且FR+-CTCs联合CEA、CYFRA21-1对NSCLC诊断的灵敏度和特异度高于CEA与CYFRA21-1联合诊断及FR+-CTCs检测单独诊断。WANG等[19]的一项研究纳入197例肺癌病人、119例肺良性疾病病人以及52例健康对照组,应用ROC曲线对诊断的特异度以及灵敏度进行分析,其研究结果显示AUCCEA+CYFRA21-1+NSE(0.649 5) 综上所述,FR+-CTCs联合CEA、CYFRA21-1检测对NSCLC诊断的特异度和灵敏度较单纯FR+-CTCs检测或CEA、CYFRA21-1联合检测均有明显提高。但由于本次纳入研究的肺癌病人绝大多数属于早期肺癌,导致本文联合检测的灵敏度和特异度较低。FR+-CTCs与CEA、CYFRA21-1联合检测在NSCLC病人的早期诊断中的作用需要进一步研究。 [参考文献] [1]BRAY F, FERLAY J, SOERJOMATARAM I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA: a Cancer Journal for Clinicians, 2018,68(6):394-424. [2]WOOD S L, PERNEMALM M, CROSBIE P A, et al. Mole-cular histology of lung cancer: from targets to treatments[J]. Cancer Treatment Reviews, 2015,41(4):361-375. [3]VERONESI G, MAISONNEUVE P, SPAGGIARI L, et al. Diagnostic performance of low-dose computed tomography screening for lung cancer over five years[J]. Journal of Thoracic Oncology, 2014,9(7):935-939. [4]LIU L J, TENG J L, ZHANG L J, et al. The combination of the tumor markers suggests the histological diagnosis of lung cancer[J]. BioMed Research International, 2017, 2017:2013989. [5]CHEN Z Q, HUANG L S, ZHU B. Assessment of seven cli-nical tumor markers in diagnosis of non-small-cell lung cancer[J]. Disease Markers, 2018, 2018:9845123. [6]CHEN X X, ZHOU F, LI X F, et al. Folate receptor-positive circulating tumor cell detected by LT-PCR-based method as a diagnostic biomarker for non-small-cell lung cancer[J]. Journal of Thoracic Oncology, 2015,10(8):1163-1171. [7]WAN J W, GAO M Z, HU R J, et al. A preliminary study on the relationship between circulating tumor cells count and cli-nical features in patients with non-small cell lung cancer[J]. Annals of Translational Medicine, 2015,3(22):352. [8]PARKER N,TURK M J,WESTRICK E, et al. Folate receptor expression in carcinomas and normal tissues determined by a quantitative radioligand binding assay[J]. Analytical Biochemistry, 2005,338(2):284-293.
[9]ALLARD W J, MATERA J, MILLER M C, et al. Tumor cells circulate in the peripheral blood of all major carcinomas but not in healthy subjects or patients with non-malignant di-seases[J]. Journal of Clinical Oncology, 2004,22(14 suppl):9552.
[10]LECHARPENTIER A, VIELH P, PEREZ-MORENO P, et al. Detection of circulating tumour cells with a hybrid (epithelial/mesenchymal) phenotype in patients with metastatic non-small cell lung cancer[J]. British Journal of Cancer, 2011,105(9):1338-1341.
[11]SEQUIST L V, NAGRATH S, TONER M, et al. The CTC-chip: an exciting new tool to detect circulating tumor cells in lung cancer patients[J]. Journal of Thoracic Oncology, 2009,4(3):281-283.
[12]STOTT S L, HSU C H, TSUKROV D I, et al. Isolation of circulating tumor cells using a microvortex-generating herringbone-chip[J]. Proceedings of the National Academy of Sciences of the United States of America, 2010,107(43):18392-18397.
[13]CHENG Y, LIU X Q, FAN Y, et al. Circulating tumor cell counts/change for outcome prediction in patients with extensive-stage small-cell lung cancer[J]. Future Oncology (London, England), 2016,12(6):789-799.
[14]YU Y, CHEN Z L, DONG J S, et al. Folate receptor-positive circulating tumor cells as a novel diagnostic biomarker in non-small cell lung cancer[J]. Translational Oncology, 2013,6(6):697-702.
[15]LOU J T, BEN S Q, YANG G H, et al. Quantification of rare circulating tumor cells in non-small cell lung cancer by ligand-targeted PCR[J]. PLoS One, 2013,8(12):e80458.
[16]NUNEZ M I, BEHRENS C, DENISE M W, et al. High expression of folate receptor alpha in lung cancer correlates with adenocarcinoma histology and mutation[J]. Journal of Thora-cic Oncology, 2012,7(5):833-840.
[17]MOLINA R, AUG J M, BOSCH X, et al. Usefulness of se-rum tumor markers, including progastrin-releasing peptide, in patients with lung cancer: correlation with histology[J]. Tumour Biology: the Journal of the International Society for Oncodevelopmental Biology and Medicine, 2009,30(3):121-129.
[18]TAKAHASHI H, KURISHIMA K, ISHIKAWA H, et al. Optimal cutoff points of CYFRA21-1 for survival prediction in non-small cell lung cancer patients based on running statistical analysis[J]. Anticancer Research, 2010,30(9):3833-3837.
[19]WANG L, WU C Y, QIAO L H, et al. Clinical significance of folate receptor-positive circulating tumor cells detected byligand-targeted polymerase chain reaction in lung cancer[J]. Journal of Cancer, 2017,8(1):104-110.
[20]ZHOU Qianjun, GENG Qing, WANG Lin, et al. Value of folate receptor-positive circulating tumour cells in the clinical management of indeterminate lung nodules: a non-invasive biomarker for predicting malignancy and tumour invasiveness[J]. Ebio Medicine, 2019,41:236-243.
[21]DING C, ZHOU X F, XU C, et al. Circulating tumor cell le-vels and carcinoembryonic antigen: an improved diagnostic method for lung adenocarcinoma[J]. Thoracic Cancer, 2018,9(11):1413-1420.
(本文編辑 黄建乡)
