伊伐布雷定在冠心病患者中的应用进展
2018-05-21黎土娣张仁丹综述曾智桓董吁钢审校
黎土娣、张仁丹综述,曾智桓、董吁钢审校
当前,我国心血管疾病负担日渐加重,已成为重大的公共卫生问题,其中冠心病患者约1 100万,发病率和死亡率呈持续上升态势[1]。研究显示心率增快与冠心病发病及死亡风险密切相关[2]。心率控制不佳在冠心病患者中普遍存在,与疼痛或焦虑导致的交感神经兴奋有关,亦与部分患者合并心功能不全有关[3]。心率增快使心肌耗氧增加、冠状动脉(冠脉)灌注下降,引起氧供需失衡,心绞痛症状反复发作;还促进有害自由基产生,损伤血管内皮,导致动脉粥样硬化进展;同时增加斑块破裂、血栓形成的风险,甚至诱发心原性猝死[4]。有学者认为应将冠心病患者心率控制在70次/分以下,以增加冠脉灌注,预防心绞痛发作,改善临床转归[5]。
β受体阻滞剂是冠心病药物治疗的基石,但由于该药本身对房室传导、心肌及支气管平滑肌的作用可导致心力衰竭(心衰)甚至心原性休克等不良反应的产生,限制了它的临床应用。而伊伐布雷定减慢窦性心率时对房室传导、心肌收缩、支气管平滑肌无干扰[6],在冠心病治疗有良好的应用前景。
1 伊伐布雷定的药理学特性
心率快慢取决于窦房结细胞4期自动去极化的速度。起搏电流在该过程中率先被激活,直接影响后续离子通道的开放时间,进而影响RR间期。伊伐布雷定可选择性、特异性抑制起搏电流,在超极化激活的环核苷门控通道开放状态下从细胞内侧进入,与窦房结细胞If通道内的位点结合,特异性抑制If电流,降低去极化速度,减慢心率(图1),对心肌收缩、心室复极化及心内传导时间均无直接影响。
伊伐布雷定在0.5~24 mg范围内的药代动力学呈线性改变,单次口服给药后迅速吸收,1 小时达血药浓度峰值。肾功能损害对该药物及其主要代谢产物有一定的影响,因为约20%的原药和代谢产物经肾脏排泄。轻度肝功能损害者服用时无需调整剂量,中度肝损伤者慎用,而严重肝功能不全是禁忌证[7]。
在临床研究中,无论是作为单药治疗[8]还是与β受体阻滞剂联用[9],伊伐布雷定均具有良好的耐受性,应用于伴随有哮喘或慢性阻塞性肺疾病的患者也是安全的[10]。在推荐剂量下,其最常见的不良事件是心动过缓和视觉症状[11]。心动过缓是意料之中的,在治疗剂量下,仅3%~4%出现心动过缓。视觉症状通常是轻度的,在治疗期间或之后可逐渐缓解,在临床试验中不到1%的患者因为视觉症状停止治疗[12]。
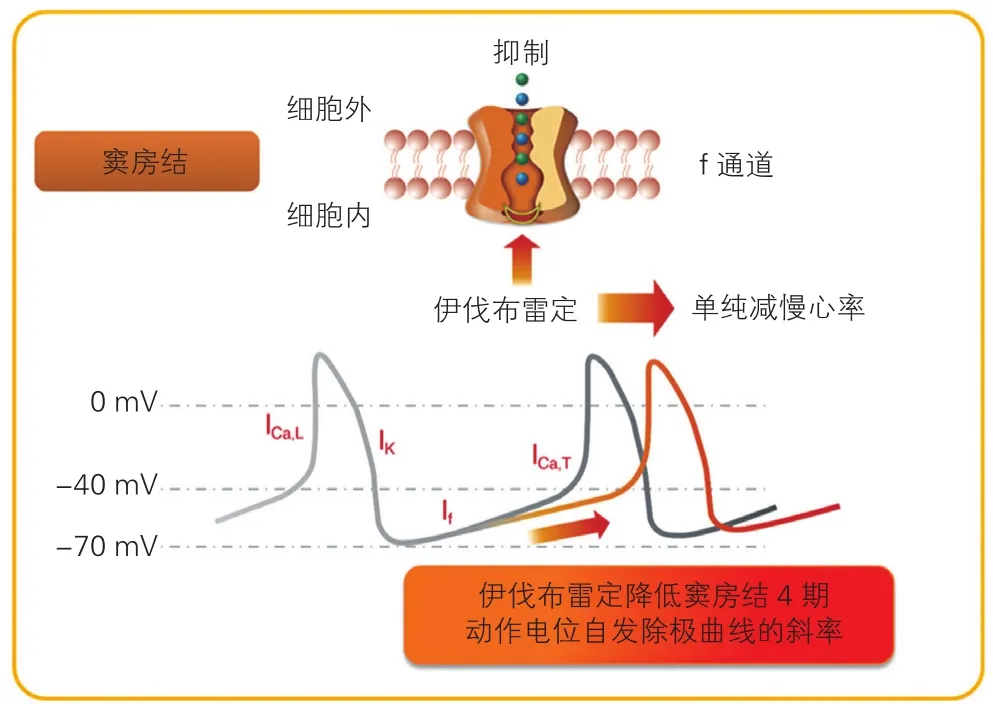
图1 伊伐布雷定的作用机制示意图
2 伊伐布雷定在不合并心力衰竭的稳定性冠心病患者中的应用
稳定性冠心病患者缺血事件发作频率与其平均心率密切相关。一项共纳入2 049例未合并心衰的稳定性冠心病患者的调查表明,83%的患者使用了β受体阻滞剂,但其中95%静息心率超过60次/分,因为73%未能足量使用,而限制其使用的主要原因是心动过缓和性功能障碍等副作用的发生[13]。全球最大的稳定性冠心病门诊患者注册研究显示,尽管β受体阻滞剂已被广泛应用,仍有40%的患者静息心率≥70次/分[14],提示当前冠心病患者心率控制仍待改善。
在慢性稳定性心绞痛患者中,与安慰剂相比,伊伐布雷定的抗缺血和抗心绞痛功效已被证实,且不劣于阿替洛尔或氨氯地平[15,16];长期与β受体阻滞剂联用可有效减慢心率,减少缺血事件和硝酸盐消耗,显著提高生活质量[12]。以未合并心功能不全的慢性稳定性冠心病患者为研究对象SIGNIFY研究结果显示,在常规药物治疗基础上,伊伐布雷定使用组心绞痛CCS分级改善比例显著高于安慰剂组,但两组间主要复合终点(心原性死亡和非致命性心肌梗死的发生率)并无显著差异[17],提示在该人群中,减慢心率治疗的主要获益源于心绞痛症状的控制,而非远期预后的改善。
伊伐布雷定增加冠脉血流储备的效应在心率校正后仍然保持,表明其可改善冠脉微循环[18]。此外,还有学者提出伊伐布雷定通过保护皮功能、促进侧支循环的建立和开放等多种机制,改善冠脉和心肌的结构及功能[19,20]。自2013年起,欧洲心脏病学会(ESC)稳定性冠心病治疗指南将其列为预防心绞痛发作的首选二线联合药物[21]。
3 伊伐布雷定在合并心力衰竭的稳定性冠心病患者中的应用
现已证实心率加快是影响慢性心衰患者远期预后的独立危险因素,直接影响包括增加心肌能量消耗、减少冠脉血供、抑制心肌收缩力等;长期持续的心率加快则可导致心肌重构,加速心功能不全进展,导致不良的临床结局[22]。以心肌梗死后左心室射血分数(LVEF)<40%且心率≥60次/分的患者为研究对象的BEAUTIFUL研究表明,相比于心率在60~70次/分之间的患者,心率超过70次/分者心原性死亡风险增加34%,住院率增加53%[23],应用伊伐布雷定治疗后,这些患者因急性心肌梗死、不稳定性心绞痛或再次冠脉血运重建接受入院治疗的风险均显著下降[24]。
SHIFT研究共分析了6 505例心率≥70次/分的慢性心衰患者(LVEF≤35%),其中4 418例为缺血性心衰。在最优化的常规药物治疗基础上,与安慰剂组相比,伊伐布雷定组主要复合终点(心血管死亡或心衰恶化入院)发生风险显著下降18%,该结果在缺血或非缺血两个预设亚组中保持一致[25]。亚组事后分析表明,与安慰剂相较,伊伐布雷定组患者主动脉顺应性和左心室后负荷显著改善,左心室舒张末期和收缩末期容积指数下降更为显著,提示减慢心率的作用可能转化为对心肌重构有益的影响[26,27]。
伊伐布雷定还可提高缺血性心衰患者对β受体阻滞剂的耐受性。Bagriy等[28]将未接受β受体阻滞剂治疗的缺血性心衰患者随机分为两组,由初始剂量卡维地洛开始,据患者耐受情况逐渐上调剂量,其中一组联用伊伐布雷定,随访5个月后,联合用药组的卡维地洛剂量显著高于对照组,达到最大剂量所需时间亦显著短于单用卡维地洛组,提示伊伐布雷定的使用提高了患者对β受体阻滞剂的耐受性,对于慢性心衰患者至关重要。在当前的ESC心衰指南中,伊伐布雷定被推荐用于经最优化常规药物治疗后仍有症状的LVEF≤35%、窦性心率≥70次/分人群,特别是当合并有稳定性心绞痛时(推荐级别为Ⅱa,证据水平为B级)[29]。
4 伊伐布雷定在急性冠脉综合征患者中的研究进展
心率水平与急性冠脉综合征患者的临床症状和远期预后亦存在关联。Bordejevic等[30]研究发现,入院时心率快的急性ST段抬高型心肌梗死患者院内死亡风险增加,即使在接受血运重建后结果亦然。一项纳入了25个随机对照临床试验,共计30 904例陈旧性心肌梗死患者的荟萃分析结果显示,静息心率每降低10次/分,心原性死亡降低30%、心原性猝死风险降低39%、全因死亡风险降低20%[31]。伊伐布雷定在此类患者中可能具有广阔的应用前景,因其具有减慢心率改善心肌缺血时对心肌收缩、心内传导无影响的优势。
有个案报道在难治性不稳定性心绞痛或急性心肌梗死患者应用伊伐布雷定可有效缓解胸痛症状[32,33],小样本研究发现其还降低急性心肌梗死患者血清生物标志物水平、降低左心室舒张和收缩末期容积、提高LVEF[34-37],提示其可改善心肌重构。这可能与伊伐布雷定有效减轻缺血性损伤,促进昏迷或冬眠心肌的恢复,以及抑制急性期炎症反应等作用有关[34,37]。应当指出,由于目前缺乏更高质量的临床研究证据,伊伐布雷定在急性冠脉综合征患者中的应用尚未获得任何药监部门的批准,在此人群中长期应用的有效性和安全性数据仍有待于进一步研究。
参考文献
[1] 陈伟伟, 高润霖, 刘力生, 等. 《中国心血管病报告2016》概要[J].中国循环杂志, 2017, 32(6): 521-530. DOI: 10. 3969/j. issn. 1000-364. 2017. 06. 001.
[2] Ho JE, Larson MG, Ghorbani A, et al. Long-term cardiovascular risks associated with an elevated heart rate: the Framingham Heart Study[J].J Am Heart Assoc, 2014, 3(3): e000668. DOI: 10. 1161/JAHA. 113.000668.
[3] 林蓉香, 张亚萍. 控制心率在冠心病治疗中的重要价值[J]. 中西医结合心血管病杂志, 2017, 15(8): 944-946. DOI: 10. 3969/j. issn.1672-1349. 2017. 08. 013.
[4] Custodis F, Schirmer SH, Baumhäkel M, et al. Vascular Pathophysiology in Response to Increased Heart Rate[J]. J Am Coll Cardiol, 2010, 24(56): 1973-1983. DOI: 10. 1016/j. jacc. 2010. 09.014.
[5] Ambrosetti M, Scardina G, Favretto G, et al. Heart rate as a therapeutic target after acute coronary syndrome and in chronic coronary heart disease[J]. G Ital Cardiol (Rome), 2017, 18(3 Suppl 1): 3S-16S. DOI:10. 1714/2685. 27479.
[6] 时珊珊, 吴晓羽. 伊伐布雷定在心血管疾病中的临床研究进展[J].中国循环杂志, 2015, 6(30): 613-616. DOI: 10. 3969/j. issn. 1000-3614. 2015. 06. 028.
[7] Deedwania P. Selective and specific inhibition of If with ivabradine for the treatment of coronary artery disease or heart failure[J]. Drugs,2013, 73(14): 1569-1586. DOI: 10. 1007/s40265-013-0117-0.
[8] Borer JS, Fox K, Jaillon P, et al. Antianginal and antiischemic effects of ivabradine, an I(f) inhibitor, in stable angina: a randomized,double-blind, multicentered, placebo-controlled trial[J]. Circulation.2003, 107(6): 817-823. DOI: 10. 1161/01. CIR. 0000048143. 25023.87.
[9] Amosova E, Andrejev E, Zaderey I, et al. Efficacy of ivabradine in combination with beta-blocker versus uptitration of beta-blocker in patients with stable angina[J]. Cardiovasc Drugs Ther, 2011, 25(6):531-537. DOI: 10. 1007/s10557-011-6327-3.
[10] Tendera M, Borer JS, Tardif JC. Efficacy of I(f) inhibition with ivabradine in different subpopulations with stable angina pectoris[J].Cardiology, 2009, 114(2): 116-125. DOI: 10. 1159/000219938.
[11] Savelieva I, Camm AJ. If inhibition with ivabradine:electrophysiological effects and safety[J]. Drug Saf, 2008, 31(2): 95-107. DOI: 10. 2165/00002018-200831020-00001.
[12] Werdan K, Ebelt H, Nuding S, et al. Ivabradine in combination with beta-blocker improves symptoms and quality of life in patients with stable angina pectoris: results from the ADDITIONS study[J]. Clin Res Cardiol, 2012, 101(5): 365-373. DOI: 10. 1007/s00392-011-0402-4.
[13] Kinsara AJ, Najm HK, Anazi MA, et al. Resting heart rate in patients with ischemic heart disease in Saudi Arabia and Egypt[J]. J Saudi Heart Assoc, 2011, 23(4): 225-232. DOI: 10. 1016/j. jsha. 2011. 05.001.
[14] Tendera M, Fox K, Ferrari R, et al. Inadequate heart rate control despite widespread use of beta-blockers in outpatients with stable CAD: findings from the international prospective CLARIFY registry[J].Int J Cardiol, 2014, 176(1): 119-124. DOI: 10. 1016/j. ijcard. 2014.06. 052.
[15] Tardif JC, Ford I, Bourassa MG, et al. Efficacy of ivabradine, a new selective If inhibitor, compared with atenolol in patients with chronic stable angina[J]. Eur Heart J, 2005, 26(23): 2529-2536. DOI: 10.1093/eurheartj/ehi586.
[16] Ruzyllo W, Tendera M, Ford I, et al. Antianginal efficacy and safety of ivabradine compared with amlodipine in patients with stable effort angina pectoris: a 3-month randomised, double-blind, multicentre,noninferiority trial[J]. Drugs, 2007, 67(3): 393-405. DOI: 10.2165/00003495-200767030-00005.
[17] Fox K, Ford I, Steg PG, et al. Ivabradine in stable coronary artery disease without clinical heart failure[J]. N Engl J Med, 2014, 371(12):1091-1099. DOI: 10. 1056/NEJMoa1406430.
[18] Skalidisa EI, Hamilosa MI, Chlouverakisb G, et al. Ivabradine improves coronary flow reserve in patients with stable coronary artery disease[J]. Atherosclerosis, 2011, 215(1): 160-165. DOI: 10. 1016/j.atherosclerosis. 2010. 11. 035.
[19] Jedlickova L, Merkovska L. Jackova L, et al. Effect of ivabradine on endothelial function in patients with stable angina pectoris: assessment with the Endo-PAT 2000 device[J]. Adv Ther, 2015, 32(10): 962-970.DOI: 10. 1007/s12325-015-0253-x.
[20] Heusch G, Skyschally P, Gres P, et al. Improvement of regional myocardial blood flow and function and reduction of infarct size with ivabradine: protection beyond heart rate reduction[J], Eur Heart J,2008, 29 (23): 2265-2275. DOI: 10. 1093/eurheartj/ehn337.
[21] Task Force Members, Montalescot G, Sechtem U, et al. 2013 ESC guidelines on the management of stable coronary artery disease: the task force on the management of stable coronary artery disease of the European Society of Cardiology[J]. Eur Heart J, 2013, 34(38): 2949-3003. DOI: 10. 1093/eurheartj/eht296.
[22] Böhm M, Swedberg K, Komajda M, et al. Heart rate as a risk factor in chronic heart failure (SHIFT): the association between heart rate and outcomes in a randomised placebo-controlled trial[J]. Lancet, 2010,376(9744): 886-894. DOI: 10. 1016/S0140-6736(10)61259-7.
[23] Fox K, Ford I, Steg PG, et al. Heart rate as a prognostic risk factor in patients with coronary artery disease and left-venticular systolic dysfunction (BEAUTIFUL): a subgroup analysis of a randomized controlled trial[J]. Lancet, 2008, 372(9641): 817-821. DOI: 10. 1016/S0140-6736(08)61171-X.
[24] Fox K, Ford I, Steg PG, et al. Ivabradine for patients with stable coronary artery disease and left-ventricular systolic dysfunction(BEAUTIFUL): a randomised, double-blind, placebo-controlled trial[J]. Lancet, 2008, 372(9641): 807-816. DOI: 10. 1016/S0140-6736(08)61170-8.
[25] Swedberg K, Komajda M, Böhm M, et al. Ivabradine and outcomes in chronic heart failure (SHIFT): a randomised placebo-controlled study[J]. Lancet, 2010, 376(9744): 875-885. DOI: 10. 1016/S0140-6736(10)61198-1.
[26] Reil JC, Tardif JC, Ford I, et al. Selective heart rate reduction with ivabradine unloads the left ventricle in heart failure patients[J]. J Am Coll Cardiol, 2013, 62(21): 1977-1985. DOI: 10. 1016/j. jacc. 2013.07. 027.
[27] Tardif JC, O'Meara E, Komajda M, et al. Effects of selective heart rate reduction with ivabradine on left ventricular remodelling and function:results from the SHIFT echocardiography substudy[J]. Eur Heart J,2011, 32(20): 2507-2515. DOI: 10. 1093/eurheartj/ehr311.
[28] Bagriy AE, Schukina EV, Samoilova OV, et al. Addition of ivabradine to β-blocker improves exercise capacity in systolic heart failure patients in a prospective, open-label study[J]. Adv Ther, 2015, 32(2):108-119. DOI: 10. 1007/s12325-015-0185-5.
[29] Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure[J]. Rev Esp Cardiol (Engl Ed) , 2016, 69(12): 2129-2200. DOI: 10. 1016/j. rec.2016. 11. 005.
[30] Bordejevic DA, Caruntu F, Mornos C, et al. Prognostic impact of blood pressure and heart rate at admission on in-hospital mortality after primary percutaneous intervention for acute myocardial infarction with ST-segment elevation in western Romania[J]. Ther Clin Risk Manag,2017, 13: 1061-1068. DOI: 10. 2147/TCRM. S141312.
[31] Cucherat M. Quantitative relationship between resting heart rate reduction and magnitude of clinical benefits in post-myocardial infarction: a meta-regression of randomized clinical trials[J]. Eur Heart J, 2007, 28(24): 3012-3019. DOI: 1 0. 1093/eurheartj/ehm489.
[32] Ripa C, Germano G, Caparra A, et al. Ivabradine use in refractory unstable angina: a case report[J]. Int J Immunopathol Pharmacol, 2009,3(22): 849-852. DOI: 10. 1177/039463200902200333.
[33] Chia PL, Foo D. Ivabradine is BEAUTIFUL in concurrent acute coronary syndrome and stroke[J]. Int J Cardiol, 2013, 163(2): 21-22.DOI: 10. 1016/j. ijcard. 2012. 08. 038.
[34] Dominguez-Rodriguez A, Abreu-Gonzalez P. Ivabradine and the antiinammatory effects in patients with ischemic heart disease[J]. Int J Cardiol, 2016, 221: 627-628. DOI: 10. 1016/j. ijcard. 2016. 07. 096.
[35] Gerbaud E, Montaudon M, Chasseriaud W, et al. Effect of ivabradine on left ventricular remodelling after reperfused myocardial infarction:A pilot study[J]. Arch Cardiovasc Dis, 2014, 107(1): 33-41. DOI: 10.1016/j. acvd. 2013. 12. 001.
[36] Barilla F, Pannarale G, Torromeo C, et al. Ivabradine in patients with ST-elevation myocardial infarction complicated by cardiogenic shock:a preliminary randomized prospective study[J]. Clin Drug Investig,2016, 36(10): 849-856. DOI: 10. 1007/s40261-016-0424-9.
[37] Priti K, Ranwa BL, Gokhroo RK, et al. Ivabradine versus metoprolol in patients with acute inferior wall myocardial infarction- ‘expanding arena for ivabradine’[J]. Cardiovasc Ther, 2017, 35(4): e12266. DOI:10. 1111/1755-5922. 12266.
