叶酸治疗冠状动脉粥样硬化患者效果评估
2018-01-08许富康孟立平吕海涛池菊芳彭放郭航远
许富康 孟立平 吕海涛 池菊芳 彭放 郭航远⋆
叶酸治疗冠状动脉粥样硬化患者效果评估
许富康 孟立平 吕海涛 池菊芳 彭放 郭航远⋆
目的 观察叶酸对合并高血压病、高同型半胱氨酸血症(HCY)冠状动脉粥样硬化患者冠状动脉狭窄程度、症状、运动耐力及不良心血管事件治疗效果。方法 自2013年5月选取冠状动脉CT检查提示冠状动脉狭窄25%~50%患者22例,分为常规治疗组、联合治疗组(常规用药+叶酸),每组各11例,对治疗前后冠状动脉最狭窄部位及其前正常部位直径进行测量,对治疗前后血管内皮功能、血HCY、血基质金属蛋白酶-2(MMP-2)、血脂水平、单核细胞计数进行测定及平板运动试验检查,并同时记录患者有无不良心血管事件发生等情况。结果 随访36个月,两组患者冠状动脉狭窄程度均减轻,联合治疗组减轻明显,差异有统计学意义(P<0.01);两组均无心肌梗塞、心绞痛、猝死等不良心血管事件发生;均无平板运动试验阳性患者。两组患者低密度脂蛋白、甘油三酯水平治疗后均较治疗前降低(P<0.01);但两组间比较差异无统计学意义(P>0.05)。两组患者血管内皮功能、MMP-2较治疗前均有改善,且联合治疗组较常规治疗组改善明显(P<0.05)。常规治疗组血HCY、血单核细胞计数无明显降低,联合治疗组较治疗前降低明显,两组比较差异有统计学意义(P<0.01)。结论 降压治疗联合阿托伐他汀钙能抑制冠状动脉粥样硬化进展,叶酸联合常规用药对高HCY患者能进一步降低冠状动脉粥样硬化狭窄程度;通过降低HCY水平、降低单核细胞计数、改善血管内皮功能、降低MMP-2水平可能是其主要机制;对于高血压病合并高HCY血症的冠状动脉粥样硬化患者,联合降HCY治疗可能能进一步抑制冠状动脉粥样硬化进展,对患者长期预后有利。
冠状动脉粥样硬化 叶酸 高同型半胱氨酸血症
Objectives To study the effect of the treatment of folic acid in coronary heart disease patients with hypertension and hyperhomocysteinemia. Methods 22 patients with coronary artery stenosis 25%~50% according to coronary CT angiography were selected and separated into two groups randomly:conventional therapy group and combined therapy group. The patients in conventional therapy group were treated with atorvastatin and Enalapril Maleate Tablets;the patients in combined therapy group were treated with atorvastatin,Enalapril Maleate and Folic Acid Tablets.All the patients were followed up for 36 months.Before and after the treatment,the diameter of coronary artery stenosis were measured,the vascular endothelial function,the levels of homocysteine,blood lipid,matrix metalloprotease-2 and monocyte were determined,treadmill exercise test was done,and also the adverse cardiovascular events were recorded. Results After 36 months therapy,the stenosis of the coronary of the patients in two groups was improved and it was improved more in the combined treatment group than that in the conventional treatment group(P<0.01).There were no adverse cardiovascular events in two groups and no treadmill exercise test positive in two groups before and after treatment.The levels of low density lipoprotein cholesterol and triglyceride were decreased by treatment at the end in the two groups (All P<0.001),but with no statistically signif i cant difference between the two groups (P=0.058 and P=0.673). The vascular endothelial function of patients in two groups were all improved and it was improved more in the combined treatment group than that in the conventional treatment group(P<0.05). The levels of homocysteine in the two groups were high and decreased at the end of treatment in the combined treatment group(P<0.001),but not decreased in the conventional treatment group(P=0.592).The levels of MMP-2 in the two groups were high but with no statistically signif i cant difference between the two groups (P=0.789). The levels of MMP-2 in the conventional treatment group were not decreased at the end of treatment,but in the combined treatment group and there was a statistically signif i cant difference between the two groups(P<0.05).There was no statistically signif i cant difference of monocyte counts between the two groups before treatment (P=0.983) and no change in the conventional treatment group after treatment,but there was a signif i cant decrease in the combined treatment group(P=0.001)and it was statistically significantly different between the two groups of the change of the monocyte counts after the treatment(P<0.05).Conclusions Antihypertensive treatment combined with atorvastatin can inhibit the progression of coronary atherosclerosis;conventional therapy combined with folic acid can reduce the degree of coronaryartery stenosis in patients with high homocysteine. The main mechanisms may reduce the level of Hcy and the count of monocytes,improve the function of vascular endothelium and decrease the level of MMP-2. For patients with coronary artery disease complicated with hypertension and hyperhomocysteinemia,folic acid combined with conventional treatment may further inhibit the progression of coronary atherosclerosis and provide a favorable long-term prognosis for patients.
Atherosclerosis Homocysteine Folic acid
冠状动脉粥样硬化是引起冠心病、导致心肌梗塞的基本病因[1]。临床及基础研究表明血脂异常是导致动脉粥样硬化的主要原因[2],他汀类药物的应用对抑制动脉粥样硬化进展、改善预后起重要作用。但近年来多项研究显示高同型半胱氨酸血症也是动脉粥样硬化发生的重要危险因素[3-4]。临床治疗中,合并高同型半胱氨酸血症的患者仍有冠状动脉狭窄病变加重[5],出现活动后胸闷胸痛,甚至出现心肌梗死可能[6]。叶酸是同型半胱氨酸代谢的重要辅助成分,既往研究证实叶酸口服能降低同型半胱氨酸水平[7]。本文探讨通过降低同型半胱氨酸水平能否进一步降低冠状动脉粥样硬化狭窄程度及其可能机制。
1 临床资料
1.1 一般资料 选择2013年5月至12月本院合并高血压病、高同型半胱氨酸血症冠状动脉狭窄25%~50%的患者22例,男13例,女9例,平均年龄(51.64±7.84)岁。排除并发肿瘤、肝肾功能不全、病毒性肝炎、近期感染等疾病。随机分成2组,每组各11例。常规治疗组:马来酸依那普利片,10mg/次,1次/d;阿托伐他汀钙片,20mg/次,1次/d;阿司匹林肠溶片,100mg/次,1次/d。联合治疗组:马来酸依那普利叶酸片,10mg/次,1次/d;阿托伐他汀钙片,20mg/次,1次/d;阿司匹林肠溶片,100mg/次,1次/d,治疗36个月。
1.2 方法 药物治疗根据患者的冠状动脉CT检查结果,确定入选者,所有入选者均于入选第二天行平板运动试验、血管内皮功能检查及血常规、血脂水平、血HCY水平、血MMP-2水平、肝肾功能测定,随后开始行药物治疗,随访1次/1个月,记录心肌梗死等不良心血管事件发生情况。在随访过程中,每3个月复查患者肝肾功能。在入选者药物干预36个月后行冠状动脉CT、平板运动试验、血管内皮功能检查及血常规、血脂水平、血HCY水平、血MMP-2水平复查。血管内皮功能采用Endo-PAT2000无创血管内皮诊断系统,依据外周动脉张力测定法原理,通过测定指端动脉张力变化获取内皮功能评估指数(ReactiveHyperemia index,RHI)进行检测。Endo-PAT2000(以色列Itamar Medical公司生产)购买自华东医药股份有限公司。冠状动脉CT检查时,以最狭窄处前后对照,记录最狭窄部位直径,并计算前后两次狭窄部位直径的差值。64排螺旋CT购自飞利浦(中国)投资有限公司。
1.3 统计学方法 采用SPSS22.0统计软件。计量资料以(x±s)表示,采用t检验。P<0.05为差异有统计学意义。
2 结果
2.1 冠状动脉狭窄程度的变化 见表1。
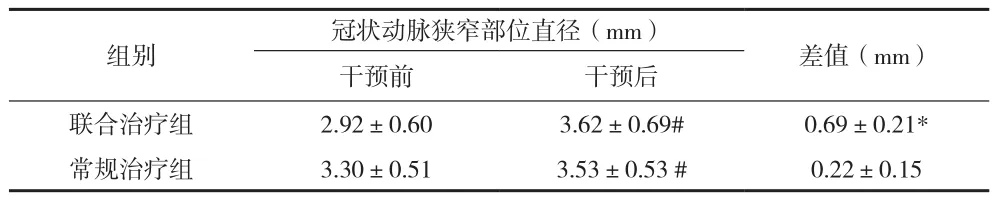
表1 两组患者干预前后冠状动脉狭窄部位直径变化比较(x±s)
2.2 生化及血管内皮功能指标 干预后,联合治疗组血管内皮功能、LDL-C、TG、HCY、MMP-2、单核细胞计数与干预前比较,差异有统计学意义(P<0.01);常规治疗组血管内皮功能、LDL-C、TG、MMP-2与干预前比较,差异有统计学意义(P<0.01);联合治疗组血管内皮功能、HCY、MMP-2、单核细胞计数与常规治疗组比较,差异有统计学意义(P<0.05),见表2。
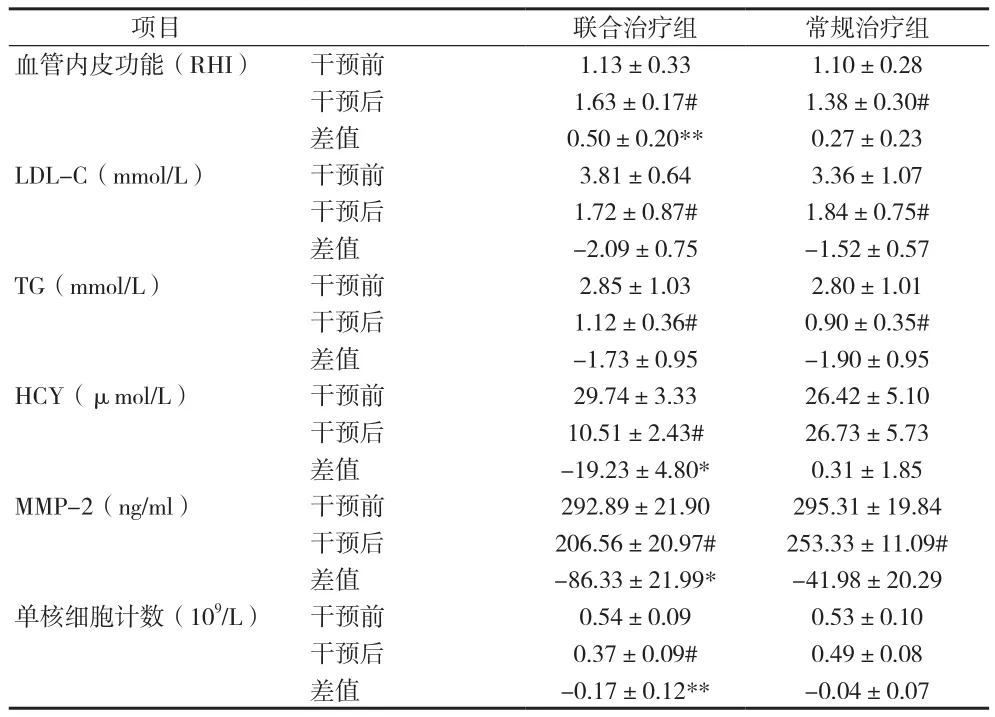
表2 两组患者干预前后各指标比较(x±s)
2.3 不良心血管事件及平板运动试验检查结果 两组患者在干预过程中无不良事件发生。治疗前后均无平板运动试验阳性患者。
3 讨论
冠心病目前是导致人类死亡的重要原因[8]。随着我国经济水平的提高及伴随的对饮食、生活等习惯的改变,使冠心病等慢性疾病增加、年轻化[9],导致猝死等发生率增高[10]。如何规范人们良好的生活习惯,认识日常健康饮食、运动等习惯的重要性,是我国人民目前实现与不断提高的经济水平相匹配的生活方式的重要方面。
高蛋白、少蔬菜等不良饮食习惯,导致同型半胱氨酸产生增加或代谢异常而引起血浆同型半胱氨酸水平升高[11]。多项研究发现,同型半胱氨酸水平的升高与冠心病、脑梗塞等动脉粥样硬化性疾病发生增加相关[4]。同型半胱氨酸是蛋白质代谢的中间产物,减少饮食中蛋白质的摄入量,或增加饮食中富含维生素蔬菜摄入,可以降低血同型半胱氨酸水平[12]。通过改变人们的饮食习惯,可能对降低血同型半胱氨酸水平、减少动脉粥样硬化性疾病发生有利。
叶酸是同型半胱氨酸代谢的重要辅助成分,通过协助同型半胱氨酸代谢可降低血同型半胱氨酸水平。既往研究发现,通过摄入叶酸可降低同型半胱氨酸水平[12],本资料显示摄入叶酸可降低血同型半胱氨酸水平,与既往研究一致。
血管内皮是动脉壁重要组成部分,内皮功能代谢异常、受损是动脉粥样硬化形成的重要机制[13]。同型半胱氨酸水平升高,可导致血管内皮细胞受损,影响血管内皮功能[14]。Dong D等研究认为,同型半胱氨酸水平升高可导致内皮细胞活性异常,甚至死亡[15]。Sharma S等动物实验发现高同型半胱氨酸血症可导致血管内皮功能异常,通过激活PI3K和其下游的PDK/Akt及eNOS是其可能机制[16]。本资料中,通过摄入叶酸可降低同型半胱氨酸水平;同时,叶酸摄入组血管内皮功能改善明显,这可能是联合叶酸治疗抗动脉粥样硬化的机制之一,即通过降低血同型半胱氨酸水平,改善血管内皮功能,抑制动脉粥样硬化的发生及进展。
血管内皮功能的异常、平滑肌细胞的迁移和增殖是导致动脉粥样硬化的重要机制。平滑肌细胞的迁移过程中,MMP-2起到重要的作用[17]。既往研究发现,高同型半胱氨酸可导致平滑肌细胞分泌MMP-2增加[18-19],高蛋氨酸饮食可导致同型半胱氨酸水平升高,血MMP-2水平升高[20]。这可能是高同型半胱氨酸致动脉粥样硬化的重要机制。本资料显示,叶酸联合治疗可降低血同型半胱氨酸水平,同时血MMP-2水平亦降低,这对抑制平滑肌细胞的迁移及抑制动脉粥样硬化进展可能起重要作用。本资料中进一步行冠状动脉CT检查亦证实,叶酸联合治疗组干预后较常规治疗组冠状动脉狭窄程度改善明显,这可能是叶酸联合治疗抑制动脉粥样硬化的重要机制,即通过降低血同型半胱氨酸,降低血MMP-2水平,抑制平滑肌细胞的迁移和增殖,进而抑制动脉粥样硬化的发生和进展。单核细胞活性的高低,对血管内皮功能及动脉粥样硬化的形成有重要的影响。过高的单核细胞活性,可引起内皮细胞损伤,影响内皮功能,或进入内皮下,形成巨噬细胞,参与动脉粥样硬化的形成及加重动脉粥样硬化等。既往研究曾发现高同型半胱氨酸血症可导致单核细胞产生增加及加重动脉粥样硬化[21]。本资料显示,叶酸联合治疗组在降低血同型半胱氨酸水平的同时,单核细胞计数亦降低,这可能是联合治疗抑制动脉粥样硬化进展的另一重要机制,即通过降低血同型半胱氨酸水平,减少单核细胞数量,改善血管内皮功能,进而抑制动脉粥样硬化的发生及进展。
[1] Smith SC Jr, Benjamin EJ, Bonow RO,et al. AHA/ACCF Secondary Prevention and Risk Reduction Therapy for Patients with Coronary and other Atherosclerotic Vascular Disease: 2011 update: a guideline from the American Heart Association and American College of Cardiology Foundation. Circulation,2011,124(22): 2458-2473.
[2] Stone NJ, Robinson JG, Lichtenstein AH, et al.American College of Cardiology/American Heart Association Task Force on Practice Guidelines.2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol,2014,63(25 Pt B):2889-2934.
[3] McCully KS. Homocysteine and the pathogenesis of atherosclerosis.Expert Rev Clin Pharmacol,2015,8(2):211-219.
[4] Ganguly P, Alam SF. Role of homocysteine in the development of cardiovascular disease. Nutr J,2015, 14(1):1-10.
[5] Gariglio L, Riviere S, Morales A, et al.Comparison of homocysteinemia and MTHFR 677CT polymorphism with Framingham Coronary Heart Risk Score. Arch Cardiol Mex,2014,84(2): 71-78.
[6] Task Force Members, Montalescot G, Sechtem U,et al.2013 ESC guidelines on the management of stable coronary artery disease: the Task Force on the management of stable coronary artery disease of the European Society of Cardiology. Eur Heart J,2013, 34(38):2949-3003.
[7] Clarke R,Frost C,Sherliker P,et al. Dose-dependent effects of folic acid on blood concentrations of homocysteine: a meta-analysis of the randomized trials. Am J Clin Nutr,2005,82(4):806-812.
[8] Zhu KF, Wang YM, Zhu JZ, et al. National prevalence of coronary heart disease and its relationship with human development index: A systematic review. Eur J Prev Cardiol,2016,23(5):530-543.
[9] Li Y, Liu S, Wang L, et al.Burden of disease attributable to main behavioral risk factor of chronic disease inactivity in China, 1990 and 2010. Zhonghua Yu Fang Yi Xue Za Zhi,2015,49(4):303-8.
[10] Zhang S. Sudden cardiac death in China: current status and future perspectives. Europace,2015,17(Suppl 2):ii14-8.
[11] Chwatko G, Boers GH, Strauss KA, et al. Mutations in methylenetetrahydrofolate reductase or cystathionine beta-synthase gene, or a high-methionine diet, increase homocysteine thiolactone levels in humans and mice. FASEB J,2007,21(8):1707-1713.
[12] Cook S, Hess OM. Homocysteine and B vitamins. Handb Exp Pharmacol,2005, 170(170):325-338.
[13] Gimbrone MA Jr, García-Cardeña G. Vascular endothelium,hemodynamics, and the pathobiology of atherosclerosis.Cardiovasc Pathol,2013,22(1):9-15.
[14] Lai WKC, Kan MY. Homocysteine-Induced Endothelial Dysfunction. Ann Nutr Metab,2015,67(1):1-12.
[15] Dong D, Wang B, Yin W, et al.Disturbance of copper homeostasis is a mechanism for homocysteine-induced vascular endothelial cell injury. PLoS One,2013,8(10):e76209.
[16] Sharma S, Singh M, Sharma PL. Mechanism of hyperhomocysteinemia-induced vascular endothelium dysfunctionpossible dysregulation of phosphatidylinositol-3-kinase and its downstream phosphoinositide dependent kinase and protein kinase B. Eur J Pharmacol, 2013, 721(1-3): 365-372.
[17] Li Z, Li L, Zielke R, et al. Increased expression of 72-kd type IV collagenase (MMP-2) in human aortic atherosclerotic lesions. Am J Pathol,1996,148 (1):121-128.
[18] Liu T, Lin J, Ju T, et al. Vascular smooth muscle cell differentiation to an osteogenic phenotype involves matrix metalloproteinase-2 modulation by homocysteine. Mol Cell Biochem, 2015,406(1-2):139-149.
[19] Doronzo G, Russo I, Mattiello L, et al.Homocysteine rapidly increases matrix metalloproteinase-2 expression and activity in cultured human vascular smooth muscle cells. Role of phosphatidyl inositol 3-kinase and mitogen activated protein kinase pathways.Thromb Haemost,2005,94(6):1285-1293.
[20] Ding H, Gan HZ, Fan WJ, et al.Homocysteine promotes intestinal fibrosis in rats with trinitrobenzene sulfonic acid-induced colitis.Dig Dis Sci,2015,60(2):375-381.
[21] Zhang D, Jiang X, Fang P, et al.Hyperhomocysteinemia promotes inflammatory monocyte generation and accelerates atherosclerosis in transgenic cystathionine beta-synthase-deficient mice. Circula tion,2009,120(19):1893-1902.
浙江省科技计划项目(2016F81SA600116)
312000 浙江省绍兴市人民医院
*通信作者
