脊柱布氏杆菌感染的临床特征表现及其治疗
2017-08-01苏菲吴子祥桑宏勋樊勇崔轶白博崔唯雷伟
苏菲 吴子祥 桑宏勋 樊勇 崔轶 白博 崔唯 雷伟
脊柱布氏杆菌感染的临床特征表现及其治疗
苏菲 吴子祥 桑宏勋 樊勇 崔轶 白博 崔唯 雷伟
目的 探讨脊柱布氏杆菌病的临床特点、治疗策略及预后。方法 回顾性分析 2 0 0 9 年 9 月至2 0 1 6 年 6 月,西京医院骨科收治的脊柱布氏杆菌感染经临床确诊、具有完整病历及随访资料的患者共 2 1 例,其中男 1 7 例,女 4 例;年龄 1 1~6 7 岁,平均 ( 4 6.9±1 2.5 ) 岁;病程 1 4~2 4 0 天,平均 ( 8 0.7±6 4.1 ) 天。对该组患者的发病特点、临床表现以及血清学、病原学、影像学的特征进行归纳分析,并观察采取不同治疗方案的临床预后。结果 本组 2 1 例均有局部疼痛症状,1 8 例有羊接触史,1 6 例有发热病史,1 0 例有多汗病史,8 例有乏力病史,5 例有肌肉疼痛病史,4 例有睾丸疼痛 ( 附睾炎 ) 病史。实验室检查结果:所有患者的布氏杆菌冷凝集试验均为阳性,结核 T-S p o t 试验均为阴性;4 例布氏杆菌血培养呈阳性。入院血沉 2 2.8~9 3 m m / h,平均 ( 5 7.2±2 0.5 ) m m / h;超敏 C 反应蛋白 6.1 2~1 5 2 m g / L,平均 ( 4 5.5±3 1.7 ) m g / L。本组病例中,颈椎 2 例,胸椎 1 例,腰骶段 3 例,腰椎 1 5 例,1 1 例存在椎管内和 ( 或 ) 椎旁脓肿形成,但仅有 1 例患者存在明显神经功能障碍 ( 肌力<3 级 ) 。所有患者 X 线片及 C T 均出现受累椎间隙狭窄或稍变窄,椎体骨质不同程度破坏。M R I 显示病变椎体在 T1像上表现为不均匀中等偏低信号,在 T2像上呈现不同程度高信号。7 例 ( 2 例颈椎,5 例腰椎 ) 接受病灶清理+植骨融合内固定手术,1 4 例接受保守治疗。所有患者均采用WH O 推荐的治疗方案:其中 3 例采用三联抗炎,1 8 例采用两联抗炎。1 5 例采用盐酸多西环素+利福平联合治疗,3 例采用盐酸多西环素+利福平+左氧氟沙星联合治疗,2 例采用链霉素+利福平联合治疗,1 例采用米诺环素+利福平联合治疗,抗炎药物使用时间 6~1 0 周,平均 ( 7.5±1.6 ) 周。术后随访 2~8 0 个月,平均( 2 5.7±1 8.5 ) 个月,患者感染局部及全身症状明显消失,椎管内脓肿吸收,神经功能恢复良好,无感染复发病例。结论 脊柱布氏杆菌病最常累及腰骶椎,局部疼痛、发热及牛羊接触的病史是较为典型的临床特征。患者血沉和超敏 C 反应蛋白显著升高,但布氏杆菌血培养阳性率较低。冷凝集试验是确诊本病的重要手段。手术指征应当严格控制,对于椎管内脓肿较多出现严重神经功能障碍患者,可考虑行手术治疗,多数患者保守治疗有效。
脊柱;布氏杆菌病;感染;疾病特征;治疗
布氏杆菌病是一种地方性人畜共患传染病,西北、东北、青藏高原及内蒙古地区多见。羊、牛及猪为主要的传染源,可经皮肤黏膜接触、呼吸道、消化道传播[1]。布氏杆菌病可累及全身多处组织或器官,如骨骼肌肉、肝脏、脾脏、脑、心脏等[2],但脊柱感染最为常见[3]。本病早期临床表现混杂,实验室检查及影像学改变与脊柱结核和脊柱肿瘤相类似[4-6],因此早期诊断比较困难,误诊率较高。回顾性研究 2 0 0 9 年 9 月至 2 0 1 6 年 6 月,第四军医大学西京医院骨科收治的 2 1 例确诊为脊柱布氏杆菌感染患者的临床资料,对其发病特点、临床表现以及血清学、病原学、影像学的特征进行归纳分析,并随访不同治疗方案的临床预后,现总结如下。
资料与方法
一、一般资料
本组 2 1 例中,其中男 1 7 例,女 4 例,年龄1 1~6 7 岁,平均 ( 4 6.9±1 2.5 ) 岁;1 0 例来自甘肃省,6 例来自山西省,3 例来自宁夏回族自治区,1 例来自青海省,1 例来自陕西省;临床表现胸背部疼痛 2 1 例,发热 1 6 例,多汗 1 0 例,乏力 8 例,肌肉痛 5 例,睾丸疼痛 4 例,神经损伤症状 8 例。首次出现症状到最后确诊时间为 1 4~2 4 0 天,平均 ( 8 0.6 7±6 4.1 ) 天。1 7 例存在饲养牛、羊史或与牛羊、牛羊肉、牛羊皮制品接触史,1 例有喝羊奶史。
二、实验室检查
入院时,患者红细胞沉降率为 2 2.8~9 3 m m / h,平均 ( 5 7.2±2 0.5 ) m m / h,超敏 C 反应蛋白 6.1 2~1 5 2 m g / L,平均 ( 4 5.5±3 1.7 ) m g / L。所有患者的布氏杆菌冷凝集试验结果均为阳性 ( 表 1 )。
三、影像学检查
所有患者均行 X 线和 C T、M R I 检查。X 线片及 C T 显示所有患者受累椎间隙狭窄或稍变窄,受累椎体骨质不同程度破坏 ( 图 1、2 );M R I 显示病变椎体在 T1像上表现为不均匀中等偏低信号,在 T2像上呈现不同程度高信号 ( 图 3 )。受累节段
显示:单节段 1 8 例,双节段 3 例。其中腰椎 1 5 例( 共 1 7 个节段,3 2 个椎体 ),腰骶段 3 例 ( 共 3 个节段,6 个椎体 ),胸椎 1 例 ( 共 2 个节段,3 个椎体 ),颈椎 2 例 ( 共 2 个节段,4 个椎体 )。2 1 例中1 1 例 ( 5 2.4% ) 于病变附近出现脓肿 ( 椎旁脓肿、腰大肌脓肿 )。7 例行核素骨扫描结果显示相应椎体骨代谢活跃。

表1 21 例脊柱布氏杆菌感染患者的临床、实验室检查特点及治疗方法Tab.1 Clinical and laboratory features and treatment for 21 patients with brucellar spondylitis
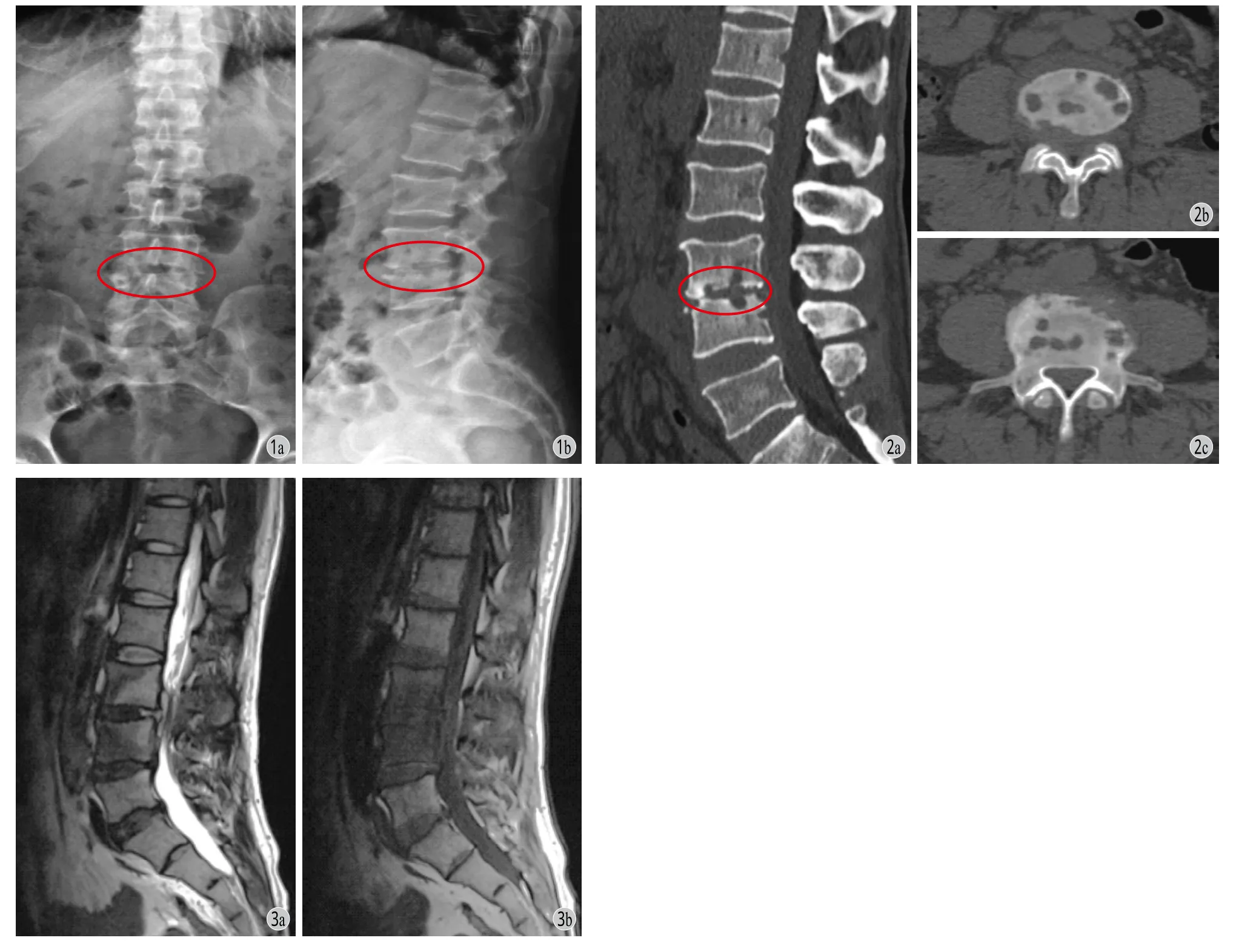
图1 患者,男,35 岁,L3~4布氏杆菌感染,X 线片可见受累节段椎间隙变窄,受累椎体出现反应性骨硬化图 2 患者,男,46 岁,L3~4布氏杆菌感染,CT 可见受累椎体的骨质破坏,椎间隙变窄,椎体边缘骨赘形成图 3 患者,男,46 岁,L3~4布氏杆菌感染,MRI 可见受累节段在T2上显示高信号,T1上显示低信号Fig.1 A 35-year-old man with L3-4brucellar spondylitis. The X-ray showed intervertebral space narrowing, and reactive bone sclerosis in the affected segmentsFig.2 A 46-year-old man with L3-4brucellar spondylitis. The CT showed bone destruction, intervertebral space narrowing and vertebral osteophyte formation in the affected segmentsFig.3 A 46-year-old man with L3-4brucellar spondylitis. The MRI showed hypointense on T1-weighted images and hyperintense on T2-weighted sequences of the intervertebral disc
四、治疗
所有患者均使用抗炎药物治疗,其中 3 例采用三联抗炎,1 8 例采用两联抗炎。1 5 例采用盐酸多西环素+利福平联合治疗,3 例采用盐酸多西环素+利福平+左氧氟沙星联合治疗,2 例采用链霉素+利福平联合治疗,1 例采用米诺环素+利福平联合治疗。药物的使用主要根据治疗的持续时间、临床特点、患者对药物的反应以及治疗期间药物的副作用进行选择。本研究中,抗炎药物使用时间 6~1 0 周,平均为 ( 7.5±1.6 ) 周。
7 例 ( 2 例颈椎,5 例腰椎 ) 因脓肿较多压迫导致神经功能障碍者接受病灶清理+植骨融合内固定手术,其中 2 例颈椎布氏杆菌感染患者采用前路手术,2 例腰椎布氏杆菌感染者采用侧前方入路手术,3 例腰椎布氏杆菌感染者采用后路手术 ( 表 1 )。所有接受手术的患者,术后送病理检查。其中 4 例术后病理结果显示慢性肉芽肿性炎,3 例显示慢性炎症细胞浸润。
结 果
一、流行病学特点
1. 人群分布:本组 2 1 例中,男 1 7 例,所占比例大 ( 8 1% ),女 4 例 ( 1 9% ),年龄 1 1~6 7 岁,主要集中在 3 0~6 0 岁,占病例数的 8 1%。
2. 职业分布:2 1 例中,农民 1 9 例 ( 9 0% ),市民 2 例。1 9 例农民中,1 7 例有饲养牛、羊史或与牛羊、牛羊肉、牛羊皮制品有接触史;市民 2 例中,1 例有喝羊奶史。
二、临床表现
本组病例最常见的症状是患区疼痛 ( 1 0 0% )、发热 ( 7 6.2% )、多汗 ( 4 7.6% ) 和乏力 ( 3 8.1% )。此外,还有部分患者可出现肌肉痛、睾丸肿痛等症状。
三、实验室检查
2 1 例血清学检查均存在血沉和 C 反应蛋白显著升高,布氏杆菌冷凝集试验均为阳性,但布氏杆菌血培养阳性率很低 ( 1 9% )。因此冷凝集试验是确诊本病的重要手段。
四、辅助检查
本组 2 1 例 X 线片及 C T 显示受累椎间隙狭窄或稍变窄,受累椎体骨质不同程度破坏;M R I 显示病变椎体在 T1像上表现为不均匀中等偏低信号,在 T2像上呈现不同程度高信号。7 例行核素骨扫描结果显示相应椎体骨代谢活跃。影像学检查在脊柱布氏杆菌感染的诊断中具有重要作用,尤以 M R I 的诊断价值更高。
五、治疗结果
本组随访 2~8 0 个月,平均 ( 2 5.7±1 8.5 ) 个月,随访期间所有患者均无复发。其中 1 3 例保守治疗患者临床症状缓解,病灶治愈,无任何并发症;1 例保守治疗患者病灶治愈,遗留腰背部僵硬感,行腰背肌理疗及功能锻炼后均缓解。7 例手术患者,病灶均骨性融合,其中 2 例遗留不同程度腰背部僵硬,但均不影响生活,经腰背肌理疗及功能锻炼后均缓解。1 8 例复查布氏杆菌冷凝集试验结果为阴性,血沉及 C 反应蛋白降至正常,3 例因特殊原因未能复查,5 例复查 M R I 显示脓肿信号较前缩小或消失。典型病例见图 4。
讨 论
一、脊椎布氏杆菌病的临床特点
人布氏杆菌病在许多国家仍然是一个重要的公共健康难题[7]。这种人畜共患的地方传染性疾病通常是由于食用被布氏杆菌感染的羊奶或者奶制品而被传播的,因其可累及多种器官及组织,所以临床表现广泛[8]。这些非特异性的临床症状常表现为发热、多汗、乏力、骨关节不适、焦虑或者沮丧以及肝胆或胃肠道的畸形,甚至引起死亡。
脊柱的布氏杆菌感染率为 8%~5 3%[9-13],最常发生在 5 0~6 0 岁之间[11]。国外研究发现,这些患者大多数为居住在农村的男性,多具有职业暴露因素存在,这与本研究的结果相符。腰背部疼痛是最常见的症状[14],有时可作为腰椎间盘受累的预兆。其原因可能是在疾病早期,由于周围软组织受损或者椎间盘的炎症反应导致脊神经受压[15-16]。本研究所有患者均出现背部疼痛的症状。因此,对于处在布氏杆菌病流行区或者有疾病高危因素 ( 牛羊接触史等 ) 的患者出现腰背部疼痛症状时应考虑到布氏杆菌病这一诊断,并进行进一步的检查。在本研究中,从出现首发症状到确诊的时间间隔为 1 4~2 4 0 天,平均为 ( 8 0.6 7±6 4.1 ) 天,主要原因为这些患者与设备完善的或者具有诊断布氏杆菌病经验丰富的医疗机构之间的距离较远。

图4 患者,男,45 岁,C6~7布氏杆菌感染。对患者行“前路 C6~7病变清除、活检,取髂骨植骨融合内固定术”a~b:术前患者颈椎 X 线片显示 C6~7椎间隙变窄,椎体周围骨质增生;c~f:术前颈椎 MRI 显示受累椎体 C6~7在 T1像为低信号、T2高信号改变;g~h:显示术后 2 年显示内固定位置满意,C6~7融合较好Fig.4 A 45-year-old man presented with C6-7brucellar spondylitis underwent the surgery of focal cleaning, bone graft fusion and internal fi xation by an anterior approach a - b: Preoperative anteroposterior and lateral X-rays showed intervertebral space narrowing, and reactive bone sclerosis in the affected segments; c - f: Preoperative MRI showed hypointense on T1-weighted images and hyperintense on T2-weighted sequences of the C6-7; g - h: At 2 years after the operation, the implantation showed satisfactory fi xation position, and C6-7fusion was better
给脊柱布氏杆菌诊断带来困难的原因之一就是该病缺乏特异性的临床症状及体征。常规抽血化验的异常结果也较少,且缺乏特异性。但是,红细胞沉降率以及 C 反应蛋白的升高对脊柱布氏杆菌病与椎间盘突出的鉴别具有重要意义,本研究中的所有患者上述两项指标均明显增高。病原菌的培养是诊断布氏杆菌病的金标准,通常选用血培养以缩短培养时间[17]。血培养的敏感度为 1 7%~8 5%,与涉及的菌种、疾病进展程度及前期抗生素的使用有关[18-19]。本组仅 4 例 ( 1 9% ) 血培养结果显示培养出布氏杆菌,这可能与患者前期服用抗生素有关。随着疾病的进展,所有布氏杆菌菌种的敏感性均会下降。因此,对脊柱布氏杆菌感染的初步诊断需要依靠血清学指标[20]。通常血清布氏杆菌抗体滴度大于 1 / 1 6 0 就被认为是阳性结果。其可提供即时的信息,结果也令人满意,其敏感度及特异度均高达9 8% 左右[2,11,21],在本研究中,所有患者的布氏杆菌冷凝集试验结果均为阳性,与上述研究相一致,足以显示出其良好的敏感度及特异度。
腰椎是脊柱布氏杆菌最常侵犯的区域,其次为胸椎和颈椎[9,11,21]。在本研究中,腰椎受累的比例最高,为 7 8%,但仅有 3 例 ( 1 4.3% ) 发生多节段感染,与国外报道 9%~2 0% 的比例相符[11]。
二、脊柱布氏杆菌病的影像学特征
脊柱感染在 X 线片上的典型特征出现在感染开始后 3~5 周[18],表现为布氏杆菌对受累椎体上、下终板的侵蚀破坏,形成骨骺炎。病灶弥漫至椎间盘导致椎间隙明显变窄或消失也比较常见[18]。但与结核性的脊柱感染相比,布氏杆菌对骨质的破坏较轻。病灶周围骨赘形成常出现在椎体终板的前缘,这种成骨性的改变出现较结核性脊柱炎早。因骨重建进展较慢,放射影像学的变化不能够轻易将其与退变性的脊柱疾病相鉴别,所以脊柱的感染性疾病常常借助于 C T、M R I 或骨扫描进行诊断及鉴别诊断[22]。
C T 检查可在疾病早期发现受累椎间盘出现低密度改变、椎间隙变窄、椎间盘破坏,以及椎体终板的侵蚀破坏[23]。也可发现椎旁脓肿影与椎体破坏区相连,形态不规则,界限清晰。但是对椎管内硬膜外脓肿造成的硬膜压迫常常要借助于增强 C T 检查,然而其效果往往没有 M R I 明显,因此对于怀疑有椎旁软组织及椎管内脊髓受累的患者应行 M R I 检查[18,22]。本组患者中有 1 1 例于病变附近出现脓肿 ( 椎旁脓肿、腰大肌脓肿 ),未见脓肿流注的直接征象。
MR I 在脊柱布氏杆菌病的诊断及后期随访中具有重要作用。其对早期的脊柱布氏杆菌病具有很高的敏感性,可以早期发现骨和周围累及的软组织信号异常、椎间隙变窄、椎体呈不均匀信号,并发现椎旁脓肿、椎管内硬膜外脓肿、破坏的椎间盘或炎性肉芽组织突入椎管导致的相应水平脊髓受压[18,23]。本研究急性的布病感染 M R I 检查,病变部位在 T2上显示高信号,T1上显示低信号,压脂像高信号,与国外文献报道相符[18,24-27]。
三、脊柱布氏杆菌病的治疗策略选择
笔者的治疗方案是采用 WT O 建议的一线用药,两种或者三种抗炎药物联合使用[28]:1 5 例采用盐酸多西环素 ( 2 0 0 m g / 天,口服 )+利福平 ( 9 0 0 m g /天,口服 ) 联合治疗;3 例采用盐酸多西环素( 2 0 0 m g / 天,口服 )+利福平 ( 9 0 0 m g / 天,口服 )+左氧氟沙星 ( 4 0 0 m g / 天,口服 ) 联合治疗;2 例采用链霉素 ( 1 g / 天,口服 )+利福平 ( 9 0 0 m g / 天,口服 ) 联合治疗;1 例采用米诺环素 ( 2 0 0 m g / 天,口服 )+利福平 ( 9 0 0 m g / 天,口服 ) 联合治疗。所有患者经过平均 7.5 周的药物使用,截止 2 0 1 6 年 8 月随访的所有患者预后均较好,与国外 2 0%~2 6% 的失败率相比,结果差距较大,结合文献报道考虑原因可能是:本组病例数较少,无法大宗病例观察;再者,感染布氏杆菌的菌株不同以及人种对药物敏感性及对布氏杆菌抵抗力存在差异[29]。
对脊柱布氏杆菌病的治疗仍存在争议,主要是在抗生素的选择、治疗的疗程及是否手术等方面。对于非手术就能确诊的脊柱布氏杆菌病,那么通过抗布氏杆菌的药物保守治疗,效果是很好的。当出现脊髓神经压迫症状的情况下才考虑手术治疗。文献报道有 3%~2 9% 的患者行手术治疗[30]。本组脊柱布氏杆菌病患者,7 例行病灶清除+植骨融合内固定手术,均为明显脊髓、神经根压迫,与国外观点一致[30-31]。手术治疗脊柱布氏杆菌病可以通过有效清创、去除病灶、充分引流、牢固融合,从而能恢复脊柱稳定性、加快康复速度、减少神经的损伤、减少并发症,使患者早期进行功能锻炼,对整个疾病的康复过程有着重要的意义。因此不能一味地追求保守治疗,严格掌握手术适应证是获得良好疗效的关键。
脊柱布氏杆菌病最常累及腰骶椎,局部疼痛、发热及牛羊接触的病史是较为典型的临床特征。患者 E S R 和 C R P 显著升高,但布氏杆菌血培养阳性率较低。冷凝集试验是确诊本病的重要手段。多数患者保守治疗有效,手术指征应当严格控制,对于椎管内脓肿较多出现严重神经功能障碍患者,可考虑行手术治疗。
[1]Yang SJ, Ren H. Infectious disease[M]. Seventh Edition, Peoples Medical Publishing House. 2008: 179-182.
[2]Franco MP, Mulder M, Gilman RH, et al. Human brucellosis[J]. Lancet Infect Dis, 2007, 7(12):775-786.
[3]Hashemi SH, Keramat F, Ranjbar M, et al. Osteoarticular complications of brucellosis in Hamedan, an endemic area in the west of Iran[J]. Int J Infect Dis, 2007, 11(6):496-500.
[4]Calik S, Gokengin AD. Human brucellosis in Turkey: a review of the literature between 1990 and 2009[J]. Turk J Med Sci, 2011, 41(3):549-555.
[5]Erdem H, Ulukilic A, Kilic S, et al. The eff i cacy and tolerability of antibiotic combinations in neuro-brucellosis: results of the Istanbul study[J]. Antimicrob Agents Chemother, 2012, 56(3):1523-1528.
[6]Gul HC, Erdem H, Bek S. Overview of neurobrucellosis: a pooled analysis of 187 cases[J]. Int J Infect Dis, 2009, 13(6): 339-343.
[7]Pappas G, Papadimitriou P, Akritidis N, et al. The new global map of human brucellosis[J]. Lancet Infect Dis, 2006, 6(2): 91-99.
[8]Haque N, Bari MS, Hossain MA, et al. An overview of brucellosis. Mymensingh[J]. Med J, 2011, 20(4):742-747.
[9]Gonzalez-Gay MA, Garcia-Porrua C, Ibanez D, et al. Osteoarticular complications of brucellosis in an Atlantic area of Spain[J]. J Rheumatol, 1999, 26(1):141-145.
[10]Khateeb MI, Araj GF, Majeed SA, et al. Brucella arthritis: a study of 96 cases in Kuwait[J]. Ann Rheum Dis, 1990, 49(12):994-998.
[11]Solera J, Lozano E, Martinez-Alfaro E, et al. Brucellar spondylitis: review of 35 cases and literature survey[J]. ClinInfect Dis, 1999, 29(6):1440-1449.
[12]Turan H, Serefhanoglu K, Karadeli E, et al. Osteoarticular involvement among 202 brucellosis cases identif i ed in Central Anatolia region of Turkey[J]. Intern Med, 2011, 50(5):421-428.
[13]Buzgan T, Karahocagil MK, Irmak H, et al. Clinical manifestations and complications in 1028 cases of brucellosis: a retrospective evaluation and review of the literature[J]. Int J Infect Dis, 2010, 14(6):e469-478.
[14]Rajapakse CN, Al-Aska AK, Al-Orainey I, et al. Spinal brucellosis[J]. Br J Rheumatol, 1987, 26(1):28-31.
[15]Ibero I, Vela P, Pascual E. Arthritis of shoulder and spinal cord compression due to Brucella disc infection[J]. Br J Rheumatol, 1997, 36(3):377-381.
[16]Kilic T, Ozer AF, Ozgen S, et al. Brucellar spondylitis mimicking lumbar disc herniation[J]. Paraplegia, 1995, 33(3): 167-169.
[17]Andriopoulos P, Tsironi M, Deftereos S, et al. Acute brucellosis: presentation, diagnosis, and treatment of 144 cases[J]. Int J Infect Dis, 2007, 11(1):52-57.
[18]Chelli BM, Ladeb MF, Chakroun M, et al. Spinal brucellosis: a review[J]. Skeletal Radiol, 2008, 37(9):785-790.
[19]Sharif HS, Aideyan OA, Clark DC, et al. Brucellar and tuberculous spondylitis: comparative imaging features[J]. Radiology, 1989, 171(2):419-425.
[20]Araj GF. Update on laboratory diagnosis of human brucellosis[J]. Int J Antimicrob Agents, 2010, 36(1 Suppl): S12-17.
[21]Yilmaz E, Parlak M, Akalin H, et al. Brucellar spondylitis: review of 25 cases[J]. J Clin Rheumatol, 2004, 10(6):300-307.
[22]Al-Shahed MS, Sharif HS, Haddad MC, et al. Imaging features of musculoskeletal brucellosis[J]. Radiographics, 1994, 14(2):333-348.
[23]Raininko RK, Aho AJ, Laine MO. Computed tomography in spondylitis. CT versus other radiographic methods[J]. Acta Orthop Scand, 1985, 56(5):372-377.
[24]Ben Taarit Ch, Turki S, Ben Maiz H. Infectious spondylitis. Study of a series of 151 cases[J]. Acta Orthop Belg, 2002, 68(4):381-387.
[25]Tali ET, Koc AM, Oner AY. Spinal Brucellosis[J]. Neuroimaging Clin N Am, 2015, 25(2):233-245.
[26]Yang XH, Zhang Q, Guo XH. Value of magnetic resonance imaging in brucellar spondylodiscitis[J]. Radiol Med, 2014, 119(12):928-933.
[27]Oztekin O, Calli C, Adibelli Z, et al. Brucellar spondylodiscitis: magnetic resonance imaging features with conventional sequences and diffusion-weighted imaging[J]. Radiol Med, 2010, 115(5):794-803.
[28]Alp E, Doganay M. Current therapeutic strategy in spinal brucellosis[J]. Int J Infect Dis, 2008, 12(6):573-577.
[29]Li XP, Ma XX, Yue B, et al. Diagnosis and treatment of spinal brucellosis disease[J]. Chin J Bone Joint Surg, 2016, 9(2): 118-121.
[30]Katonis P, Tzermiadianos M, Gikas A, et al. Surgical treatment of spinal brucellosis[J]. Clin Orthop Relat Res, 2006, 444(444): 66-72.
[31]Turgut M, Turgut AT, Koşar U. Spinal brucellosis: Turkish experience based on 452 cases published during the last century[J]. Acta Neurochir (Wien), 2006, 148(10):1033-1044.
Clinical characteristics and treatment of spinal brucellosis disease
SU Fei, WU Zi-xiang, SANG Hong-xun, FAN
Yong, CUI Yi, BAI Bo, CUI Wei, LEI Wei. Department of Orthopedics, Xijing Hospital, the fourth Military Medical University, Xi’an, Shaanxi, 710032, China
WU Zi-xiang, Email: wuzixiang@fmmu.edu.cn
Objective To analyze clinical data of patients with spinal brucellosis and to summarize clinical characteristics, treatment strategy and prognosis of the disease. Methods From September 2009 to June 2016, 21 patients with spinal brucellosis were treated in our hospital. The diagnosis was clinically confirmed, and all of them had complete medical records and follow-up data. There were 17 males and 4 females, with a mean age of ( 46.9 ± 12.5 ) years ( range: 11 - 67 years ). The average course was ( 80.7 ± 64.1 ) days ( range: 14 - 240 days ). Their clinical data were collected and analyzed retrospectively, including the complaints, clinical manifestations, serological and etiological results and imaging changes. The clinical outcomes of different treatment options were observed. Results They complained mainly about local pain ( n = 21 ), history of exposure to cattle or sheep ( n = 18 ), fever ( n = 16 ), sweats ( n = 10 ), fatigue ( n = 8 ), myalgia ( n = 5 ) and testicular pain ( epididymitis ) ( n = 4 ). As to thelaboratory examination, positive results were obtained in the standard tube agglutination test, and negative results in the T-spot TB test in all the patients. Cultures of blood specimens from 4 patients were positive for brucella melitensis. The mean value of erythrocyte sedimentation rate ( ESR ) was ( 57.2 ± 20.5 ) mm / h ( range: 22.8 - 93 mm / h ). The mean value of hypersensitive C-reactive protein ( CRP ) was ( 45.5 ± 31.7 ) mg / L ( range: 6.12 - 152 mg / L ). The defect site was noted in cervical spine of 2 cases, thoracic spine of 1 case, lumbosacral spine of 3 cases and lumbar spine of 15 cases. Paravertebral masses and / or epidural masses were detected in 11 patients, but only 1 patient had significant neurological dysfunction ( myodynamia < grade 3 ). The X-ray and CT showed infected intervertebral disc stenosis or slightly narrow and affected vertebral body bone destruction in 21 cases. The MRI showed uneven hypointense on T1-weighted images and uneven hyperintense on T2-weighted sequences of the intervertebral disc in 21 cases. Seven patients ( 2 cases of cervical spinal brucellosis and 5 cases of lumbar spinal brucellosis ) underwent the surgery of focal cleaning, bone graft fusion and internal fi xation, and 14 patients were treated by oral medicine. World Health Organization ( WHO ) recommended treatment was performed on all the patients, with a combination of 2 ( in 18 cases ) or 3 ( in 3 cases ) agents. Fifteen patients
a combination of tetracycline and rifampicin. Three patients received a combination of doxycycline, rifampicin, and levof l oxacin. Two patients received a combination of streptomycin and rifampicin. One patient received a combination of minocycline and rifampicin. The mean duration of antimicrobial treatment was ( 7.5 ± 1.6 ) weeks ( range: 6 - 10 weeks ). The mean duration of follow-up was ( 25.7 ± 18.5 ) months ( range: 2 - 80 months ). Good prognosis was achieved in all the patients, without any local infections or systemic symptoms. Resolution of epidural or paravertebral masses and recovery of neurological function occurred in all the patients. There were no clinical or radiological relapses. Conclusions The lumbar spine is the most frequent level involved in spinal brucellosis. Most patients have typical clinical features of local pain, fever and exposure to cattle or sheep. The ESR and CRP values increase signif i cantly, while the positive rate of brucella blood culture is lower. So the standard tube agglutination test is an important means in the diagnosis of this disease. The conservative treatment can be effective for most patients. Surgical indications should be strictly controlled. If a localized infection focus or extradural abscess compresses the spinal cord and / or the nerve root, causing severe neurological dysfunction, the surgical discectomy procedure should be used.
Spine; Brucellosis; Infection; Disease attributes; Therapy
10.3969/j.issn.2095-252X.2017.07.014
R681.2
2016-11-20 )
( 本文编辑:王萌 )
关于投稿请提供伦理委员会批准文件及受试对象知情同意书
国家自然科学基金面上项目 ( 8 1 2 7 0 9 5 9 )
7 1 0 0 3 2 西安,第四军医大学第一附属医院骨科 ( 苏菲、吴子祥、桑宏勋、白博、雷伟 );5 1 8 0 0 0 深圳,南方医科大学深圳医院骨科中心 ( 桑宏勋 );7 1 0 0 5 4 西安交通大学医学院附属红会医院 ( 樊勇 );6 5 0 0 3 2 昆明,解放军昆明总医院骨科 ( 崔轶 );1 1 6 0 2 3 大连医科大学第二附属医院 ( 崔唯 )
吴子祥,E m a i l: w u z i x i a n g@f m m u.e d u.c n
本刊要求,当论文的主体是以人为研究对象的试验时,作者应该说明其遵循的程序是否符合负责人体试验的委员会 ( 单位性的、地区性的或国家性的 ) 所制订的伦理学标准,并提供该委员会的批准文件,及受试对象的知情同意书。