Impaired consciousness caused by injury of the lower ascending reticular activating system: evaluation by diffusion tensor tractography
2016-12-02SungHoJang,SeongHoKim,HanDoLee
IMAGING IN NEURAL
Impaired consciousness caused by injury of the lower ascending reticular activating system: evaluation by diffusion tensor tractography
A 34-year-old male patient underwent conservative management for traumatic hemorrhage in the right frontal lobe (Figure 1A). The patient lost consciousness for approximately 4 weeks and experienced post-traumatic amnesia continuously from the time of the accident. The patient’s Glasgow Coma Scale score (Teasdale et al., 1974) was 6 when he arrived at the hospital. At 5 weeks after onset, he was transferred to the rehabilitation department to undergo rehabilitation. Brain MRI showed malactic lesions in both the frontal lobes and right thalamus (Figure 1B). The patient exhibited impaired consciousness, with a Glasgow Coma Scale score of 9 and Coma Recovery Scale-Revised score of 8 (Giacino et al., 2004).
Diffusion tensor tractography (DTT) data were obtained at 6 weeks after onset using a 6-channel head coil on a 1.5 T Philips Gyroscan Intera (Philips, Best, the Netherlands) with single-shot echo-planar imaging. Imaging parameters were as follows: acquisition matrix = 96 × 96; reconstructed matrix = 192 × 192; field of view = 240 × 240 mm2; repetition time = 10,726 ms; echo time = 76 ms; parallel imaging reduction factor (SENSE factor) = 2; EPI factor = 49; b = 1,000 s/mm2; number of excitations = 1; and a slice thickness of 2.5 mm. FACT algorithm was used for fiber tracking. For ascending reticular activating system (ARAS) analysis, the seed region of interest (ROI) was given on the pontine reticular formation. According to previous reports (Yeo et al., 2013; Jang et al., 2014), the target ROI was placed on the thalamic intralaminar nuclei to analyze the connectivity of the intralaminar nuclei. The patient showed intact neural connectivity between the thalamic intralaminar nuclei the frontal lobe. However, the left lower ARAS between pontine reticular formation and thalamic intralaminar nuclei was thinner than the right lower one of the same patient and those in five age-matched healthy control subjects (Figure 1C).
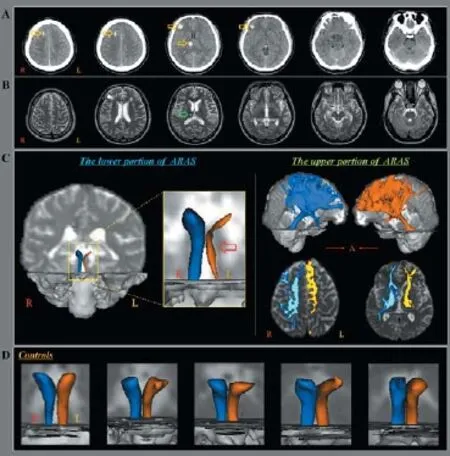
Figure 1 Brain CT images, magnetic resonance images and diffusion tensor tractography (DTT) images of a 34-year-old male patient with traumatic brain injury.
In this study, we evaluated the ARAS in a patient with severe traumatic brain injury through two portions: First, three-dimensional reconstruction at the lower ARAS between the pontine reticular formation and the thalamic intralaminar nuclei, second, neural connectivity of the upper ARAS between the thalamic intralaminar nuclei and the cerebral cortex. Our results showed that the left lower ARAS was thinner than that of the right side of the patient and those of normal subjects. These findings appear to suggest an injury of the left lower ARAS. This injury was attributed to traumatic axonal injury because the conventional brain MRI of the patient was normal in the left thalamus and brainstem. Before analysis of the ARAS, we assumed that the main lesion would be located in the right ARAS and left upper ARAS because the brain MRI showed malactic lesions in both frontal lobes and the right thalamus. The main lesion site was detected in the left lower ARAS between the thalamic reticular formation and the thalamic intralaminar nuclei (Edlow et al., 2013; Jang et al., 2015a, b). Our results suggest that analysis of the ARAS using DTT would be useful for elucidating the cause of impaired consciousness. However, limitation of DTT with 1.5 T MRI should be considered, because a higher tesla MRI such as 3.0 T, can show better resolution and identify small tract more precisely.
This work was supported by the National Research Foundation (NRF) of Korea Grant funded by the Korean Government (MSIP), No. 2015R1A2A2A01004073.
Sung Ho Jang, Seong Ho Kim, Han Do Lee*
Department of Physical Medicine and Rehabilitation, College of Medicine, Yeungnam University, Namku, Daegu, Republic of Korea (Jang SH, Lee HD)
Department of Neurosurgery, College of Medicine, Yeungnam University, Namku, Daegu, Republic of Korea (Kim SH)
*Correspondence to: Han Do Lee, M.S., lhd890221@hanmail.net.
Accepted: 2016-01-16
orcid: 0000-00002-1668-2187 (Han Do Lee)
Edlow BL, Haynes RL, Takahashi E, Klein JP, Cummings P, Benner T, Greer DM, Greenberg SM, Wu O, Kinney HC, Folkerth RD (2013) Disconnection of the ascending arousal system in traumatic coma. J Neuropathol Exp Neurol 72:505-523.
Giacino JT, Kalmar K, Whyte J (2004) The JFK coma recovery scale-revised: measurement characteristics and diagnostic utility. Arch Phys Med Rehabil 85:2020-2029.
Jang SH, Lim HW, Yeo SS (2014) The neural connectivity of the intralaminal thalamic nuclei in the human brain: a diffusion tensor tractography study. Neurosci Lett 2014;579:140-144.
Jang SH, Lim HW, Yeo SS (2015a) Injury of the ascending reticular activating system by transtentorial herniation in a patient with intracerebral haemorrhage: a diffusion tensor tractography study. J Neurol Neurosurg Psychiatry 86:1164-1166.
Jang SH, Kim SH, Lim HW, Yeo SS (2015b) Recovery of injured lower portion of the ascending reticular activating system in a patient with traumatic brain injury. Am J Phys Med Rehabil 94:250-253.
Teasdale G, Jennett B (1974) Assessment of coma and impaired consciousness. A practical scale. Lancet 2:81-84.
Yeo SS, Chang PH, Jang SH (2013) The ascending reticular activating system from pontine reticular formation to the thalamus in the human brain. Front Hum Neurosci 7:416.
10.4103/1673-5374.177746 http://www.nrronline.org/
How to cite this article: Jang SH, Kim SH, Lee HD (2016) Impaired consciousness caused by injury of the lower ascending reticular activating system: evaluation by diffusion tensor tractography. Neural Regen Res 11(2):352.
杂志排行

中国神经再生研究(英文版)的其它文章
- Tissue-type plasminogen activator is a modulator of the synaptic vesicle cycle
- Epalrestat protects against diabetic peripheral neuropathy by alleviating oxidative stress and inhibiting polyol pathway
- Considering calcium-binding proteins in invertebrates: multi-functional proteins that shape neuronal growth
- Cardiovascular dysfunction following spinal cord injury
- Practical application of the neuroregenerative properties of ketamine: real world treatment experience
- Exergames: neuroplastic hypothesis about cognitive improvement and biological effects on physical function of institutionalized older persons