Pseudohyperkalemia with Myelofibrosis after Splenectomy
2016-10-13ShengliLiuLuweiZhangandJunTian
Sheng-li Liu, Lu-wei Zhang, and Jun Tian*
Pseudohyperkalemia with Myelofibrosis after Splenectomy
Sheng-li Liu, Lu-wei Zhang, and Jun Tian*
Center of Kidney Transplantation and Hemodialysis,Qilu Hospital of Shandong University, Jinan 250012, China
pseudohyperkalemia; serum potassium; plasma potassium; myelofibrosis; splenectomy
Chin Med Sci J 2016; 31(4):258-260
SEUDOHYPERKALEMIA refers the serum potassium level is higher than plasma potassium due to various reasons in vitro monitoring, but actual potassium level in vivo is at the normal range. A series of inappropriate clinical interventions due to initial failure to recognize it may actually decrease potassium level,which could cause life-threatening condition. Here we report a patient with myelofibrosis who occurred spurious hyperkalemia after splenectomy, aiming at emphasizing the importance of recognizing pseudodyperkalemia.
Case Description
A 63-year-old Chinese male presented at the hospital for increasingly aggravated symptoms of anemia and abdominal discomfort. He was diagnosed as myelofibrosis and had been given intermittent infusion of red blood cells and conservative treatment for 4 years. Now the patient strongly urged to be hospitalized for splenectomy. Physical examination revealed enlarged spleen with nearly 20cm in Ⅰ-line, 25cm in Ⅱ-line and almost +4.5 cm in Ⅲ-line. Laboratory investigation demonstrated a moderate anemia (RBC 2.35×1012/L,HGB 62g/L), mild thrombocytopenia (85´109/L), normal leukocyte count (9.6×109/L) and normal serum potassium level (4.2 mmol/L). The patient was hospitalized and received splenectomy under general anesthesia after preoperative preparation. His postoperative condition was stable accompanied with improvement of blood routine index(RBC 3.80×1012/L, platelet 179´109/L, leukocyte 31.2×109/L)(Fig. 1)excepted that the serum potassium level gradually rose up to 7.47 mmol/L (Fig. 2) on the seventh day after operation.
In this circumstance, the doctors made a careful investigation for the reason of elevated serum potassium. Neither did the patient use potassium-containing drugs, nor eat potassium-related food. Renal function tests were normal and there were no clinical evidence of adrenal insufficiency and diabetes mellitus. Vital sign was stable, the ECG monitoring showed no sign of hyperkalemia. To prevent severe life-threaten event, the treatments of rehy- dration, diuresis, pushing calcium, and sodium bicarbonate infusion were given to reduce serum potassium level. However, it remained at a level of 7.0 mmol/L. Blood dialysis treatment was performed then on eighth day after operation, and serum potassium level was down to 3.5 mmol/L. However, it returned to 7.4 mmol/L the next day.
This phenomenon raised caution of doctors,and further investigations were undertook. Considering the drawbacks that self-condensate tube had, and routine transportation of pneumatic tube we used for serum potassium exami- nation, we measured plasma potassium level using a heparinized sample of arterial blood gas with manual transport, which turned out to be 2.1 mmol/L. After a careful review of patient’s medical information, we believed this result was reasonable. We carried out potassium supplement therapy in order to prevent severe events caused by hypokalemia. Since then the patient's plasma potassium level kept stable as shown in Fig. 2, with the discrepancy around 3.3 mmol/L till discharged from the hospital on the twelfth day after operation.
Discussion
Clinically potassium imbalance is one of the most common electrolyte disorders. Hyperkalemia is generally defined as that the potassium level is higher than 5.5 mmol/L in vivo.1The symptoms are mainly the toxic effect of potassium on the myocardium and skeletal muscle. When the potassium level is higher than 7.0 mmol/L, the patients may have cardiac arrest and muscle numbness. Therefore, it is of great clinical significance to diagnose and treat hyperkalemia in time.
Pseudohyperkalemia is characterized by marked elevation of serum potassium level without clinical symptoms of electrolyte imbalance.2Currently, it is defined as that the serum potassium concentration exceeds the plasma potassium 0.4 mmol/L when the samples are collected in strict operation, stored under room temperature and tested in 30 minute.3Therefore, joint measurements of serum potassium and plasma potassium are essential for diagnosis of pseudohyperkalemia. In this case, the great discrepancy between plasma potassium and serum potassium indicated pseudohyperkalemia, and the absence of clinical symptom and ECG was consistent with the diagnosis.
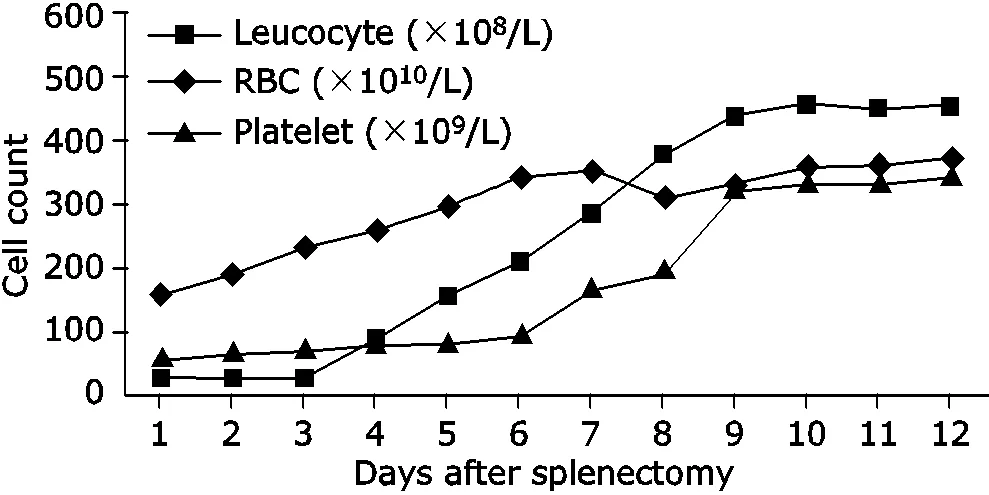
Figure 1. Measurements of blood cells and platelets rose gradually by days after splenectomy.
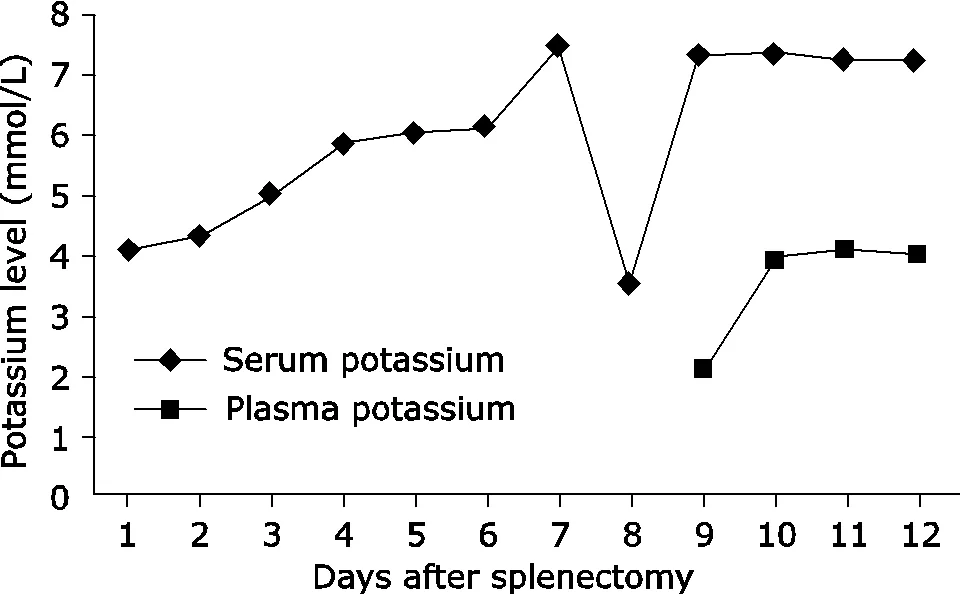
Figure 2. Measurements of serum potassium and plasma pota- ssium changed by days after splenectomy.
Ong YL4had reported, based on a large sample study, that main aetiology of pseudohyperkalemia were acute and chronic myeloproliferative related primary thrombocytosis or leukocytosis, followed by reactive thro- mbocytosis in condition of rheumatoid arthritis, splenectomy, as well as renal cancer. Rarely, pseudohyperkalemia has been associated with hereditary spherocytosis and infec- tious mononucleosis. The case we report here is a myelofi- brosis patient with splenectomy, indicating both the primary and secondary hematological disorders could lead to this spurious phenomenon.
Myelofibrosis, as a disease that excessive deposition of collagen fiber in bone marrow tissue interfereing its hematopoietic function,is usually confirmed by biopsy.5Owing to its ineffective hematopoiesis and concurrent splenomegaly, the differentiation and maturation of RBC are affected, and there are even teardrop-like RBC in the peripheral blood.6So patients generally appear the severe symptom of anemia, but the leukocyte and platelet may maintain normally or even higher. According to the blood cells measurements before and after splenectomy in this case, we postulated that the patient might be at the late stage of myelofibrosis, most cells were in the immature stage and the fragile membrane was prone to rupture or hemolysis. Since in our hospital, extraction of serum usually go through 6 minutes of centrifugation at a speed of 4000 rpm/min, the mechanical force from routine pneumatic tube transport and centrifugation7might cause cells lysis, then potassium ions and other cellular components could release from disrupted RBC and leukocyte during the whole clotting process.
Some scholars believed that severe leukocytosis could cause excessive fuel consumption of cell metabolism, resu- lting in inactivity of Na-K-ATP enzyme, and leading to large amounts of potassium ions released from leukocytes.8Kellerman PS9reported that leukocyte could lead to significant pseudohyperkalemia when its counts reach over 100×109/L. In the case we report, the leukocyte level gradually increased up to 50´109/L after splenectomy, sug- gesting leukocytosis might contribute to the pseudohy- perkalemia as well.
In conclusion, this case reminds us that elevated serum potassium with absence of clinical symptoms or signs of hyperkalemia in the setting of abnormal blood components is suspicious for pseudohyperkalemia. Plasma potassium examination should be performed for early diagnosis, which is of important significance for clinical practice of doctors.
1. Weisberg LS. Management of severe hyperkalemia. Crit Care Med 2008; 36: 3246-51.
2. Sevastos N, Theodossiades G, Savvas SP, et al. Pseudohy- perkalemia in patients with increased cellular components of blood. Am J Med Sci 2006; 331: 17-21.
3. Sevastos N, Theodossiades G, Archimandritis AJ. Pseudo- hyperkalemia in serum: a new insight into an old pheno- menon. Clin Med Res 2008; 6: 30-32.
4. Ong Y L, Deore R, Elagnaf M. Pseudohyperkalaemia is a common finding in myeloproliferative disorders that may lead to inappropriate management of patients. Int J Lab Hematol 2010; 32: e151–7.
5. Mesa RA, Hanson CA, Rajkumar SV, et al. Evaluation and clinical correlations of bone marrow angiogenesis in myelofibrosis with myeloid metaplasia. Blood 2000; 96:3374-80.
6. Tefferi A. Myelofibrosis with Myeloid Metaplasia. New Engl J Med 2000; 342:1255-65.
7. Garwicz D, Karlman M. Early recognition of reverse pseudohyperkalemia in heparin plasma samples during leukemic hyperleukocytosis can prevent iatrogenic hypo- kalemia. Clin Biochem 2012; 45:1700-2.
8. Ruddy KJ, Wu D, Brown JR. Pseudohyperkalemia in chronic lymphocytic leukemia. J Clin Oncol 2008; 26: 2781-2.
9. Kellerman PS, Thornbery JM. Pseudohyperkalemia due to pneumatic tube transport in a leukemic patient. Am J Kidney Dis 2005; 46:746-8.
for publication September 17, 2015.
Tel 0531-82169527, Email juntianqlyy@sina.com
杂志排行

Chinese Medical Sciences Journal的其它文章
- Expression of miRNA-140 in Chondrocytes and Synovial Fluid of Knee Joints in Patients with Osteoarthritis△
- Effects of Lianhua Qingwen on Pulmonary Oxidative Lesions Induced by Fine Particulates (PM2.5) in Rats
- The Effect of Sleep Deprivation on Coronary Heart Disease△
- Uterine Artery Embolization for Management of Primary Postpartum Hemorrhage Associated with Placenta Accreta
- Meta-analysis of aspirin-heparin therapy for un-explained recurrent miscarriage
- A Case Report of Acute Arterial Embolization of Right Lower Extremity As the Initial Presentation of Nephrotic Syndrome with Minimal Changes△