普拉格雷在行经皮冠状动脉介入治疗的急性冠脉综合征患者中的应用效果
2016-06-28王树源黄家卓
王树源,黄家卓
·药物与临床·
普拉格雷在行经皮冠状动脉介入治疗的急性冠脉综合征患者中的应用效果
王树源,黄家卓
526020广东省肇庆市第一人民医院心血管内科
【摘要】目的观察普拉格雷在行经皮冠状动脉介入治疗(PCI)的急性冠脉综合征(ACS)患者中的应用效果。方法选取2013年11月—2014年7月在肇庆市第一人民医院心血管内科住院治疗的ACS患者62例,随机分为对照组和观察组,每组31例。两组患者均进行PCI,对照组患者于PCI术前3 d口服阿司匹林和氯吡格雷,术后继续口服氯吡格雷维持治疗1年;观察组患者于PCI术前3 d口服阿司匹林和普拉格雷,术后继续口服普拉格雷维持治疗1年。比较两组患者PCI术前及术后12 h血小板反应指数(PRI)、TIMI血流3级率和术后12 h PRI<50%者所占比例;两组患者出院后均随访1年,记录其主要终点事件、次要终点事件和联合终点事件发生情况。结果两组患者术前PRI、TIMI血流3级率比较,差异均无统计学意义(P>0.05);观察组患者术后12 h PRI低于对照组,术后12 h PRI<50%者所占比例高于对照组(P<0.05);而两组患者术后12 h TIMI血流3级率比较,差异无统计学意义(P>0.05)。两组患者主要终点事件发生率及发生风险比较、次要终点事件发生率及发生风险比较,差异均无统计学意义(P>0.05);而观察组患者联合终点事件发生率及发生风险均低于对照组(P<0.05)。结论普拉格雷能有效抑制血小板聚集,降低ACS患者术后联合终点事件发生率,具有较好的临床应用前景。
【关键词】急性冠脉综合征;血管成形术,气囊,冠状动脉;普拉格雷;氯吡格雷;治疗效果
王树源,黄家卓.普拉格雷在行经皮冠状动脉介入治疗的急性冠脉综合征患者中的应用效果[J].实用心脑肺血管病杂志,2016,24(5):109-112.[www.syxnf.net]
Wang SY,Huang JZ.Application effect of prasugrel in acute coronary syndrome patients treated by PCI[J].Practical Journal of Cardiac Cerebral Pneumal and Vascular Disease,2016,24(5):109-112.
急性冠脉综合征(ACS)是一种临床上常见的严重心血管疾病,其以冠状动脉粥样硬化斑块破裂或侵袭继发完全或不完全闭塞性血栓形成为主要病理改变,常见于老年男性、吸烟及有高血压、高脂血症、糖尿病、肥胖及冠心病家族史者[1]。ACS主要临床表现为发作性胸痛、胸闷等,可导致心律失常、心力衰竭甚至猝死,严重影响患者的生命安全和生活质量。据统计,全球每年约有(800~900)万人因ACS而死亡[2]。近十年来我国ACS发病率逐年升高并已接近国际平均水平,而经皮冠状动脉介入治疗(PCI)作为ASS的首选治疗方法,其在有效改善患者临床症状的同时也存在一些弊端,如术后支架内再狭窄、冠状动脉内血栓形成等[3]。
普拉格雷是第三代噻吩并吡啶类抗血小板药物,对P2Y12的抑制作用较氯吡格雷更快、更强[4]。有学者指出,PCI术后接受普拉格雷治疗的ACS患者再缺血事件发生风险明显低于接受氯吡格雷治疗的ACS患者,但部分患者出血并发症发生风险增高,而与此相反的是,采用非侵入性方式治疗的ACS患者接受普拉格雷治疗后并不能达到满意效果[5]。因此,欧洲心脏病学会(ESC)和美国心脏病协会(AHA)推荐ST段抬高型心肌梗死(STEMI)患者和非ST段抬高ACS患者接受PCI和普拉格雷治疗[6],但鉴于普拉格雷会引起部分患者出血风险增高,因此临床用药过程中不断修改和完善了普拉格雷的适应证和使用剂量:有卒中或短暂性脑缺血发作史的患者应避免使用普拉格雷;年龄≥75岁和体质量<60 kg的患者每日维持剂量减少至5 mg[7]。本研究旨在观察普拉格雷在行PCI的ACS患者中的应用效果,现报道如下。
1资料与方法
1.1一般资料选取2013年11月—2014年7月在肇庆市第一人民医院心血管内科住院治疗的ACS患者62例,年龄30~75岁,均符合“2012年不稳定型心绞痛和非ST段抬高型心肌梗死诊断治疗指南”中不稳定型心绞痛(UA)或急性心肌梗死(AMI)的诊断标准,并经冠状动脉造影检查证实,排除糖尿病、肝肾功能不全、心力衰竭、严重感染及合并其他严重器质性疾病患者。将所有患者随机分为对照组和观察组,每组31例。两组患者性别、年龄、病程、体质指数、收缩压、舒张压及吸烟率比较,差异均无统计学意义(P>0.05,见表1),具有可比性。所有患者对本研究内容知情并签署知情同意书。
1.2治疗方法两组患者均采用Judkins法进行冠状动脉造影并按照相应操作指南完成PCI手术,对照组患者于PCI术前3 d口服阿司匹林(沈阳康芝制药有限公司生产,国药准字H20103712)100 mg/d和氯吡格雷〔赛诺菲(杭州)制药有限公司生产,国药准字H20056410〕75 mg/d,术后继续口服氯吡格雷75 mg/d维持治疗1年;观察组患者于PCI术前3 d口服阿司匹林100 mg/d和普拉格雷(美国礼来公司生产)30 mg/d,术后继续口服普拉格雷10 mg/d维持治疗1年,体质量<60 kg和/或年龄>75岁的患者普拉格雷剂量减为5 mg/d。
1.3观察指标比较两组患者PCI术前及术后12 h血小板反应指数(PRI)、TIMI血流3级率和术后12 h PRI<50%者所占比例;两组患者出院后均随访1年,记录其主要终点事件、次要终点事件和联合终点事件发生情况,其中主要终点事件包括死亡、再梗死和卒中等,次要终点事件包括再入院、其他部位血栓、心功能不全等,主要终点事件与次要终点事件合计为联合终点事件。

2结果
2.1PRI、TIMI血流3级率及术后12 h PRI<50%者所占比例两组患者术前PRI、TIMI血流3级率比较,差异均无统计学意义(P>0.05)。观察组患者术后12 h PRI低于对照组,术后12 h PRI<50%者所占比例高于对照组,差异均有统计学意义(P<0.05);而两组患者术后12 h TIMI血流3级率比较,差异无统计学意义(P>0.05,见表2)。
表2两组患者PRI、TIMI血流3级率及术后12 h PRI<50%者所占比例比较
Table 2Comparison of PRI and the proportion of patients with 3-grade TIMI blood flow before PCI and after 12 hours of PCI,and PRI less than 50% after 12 hours of PCI between the two groups
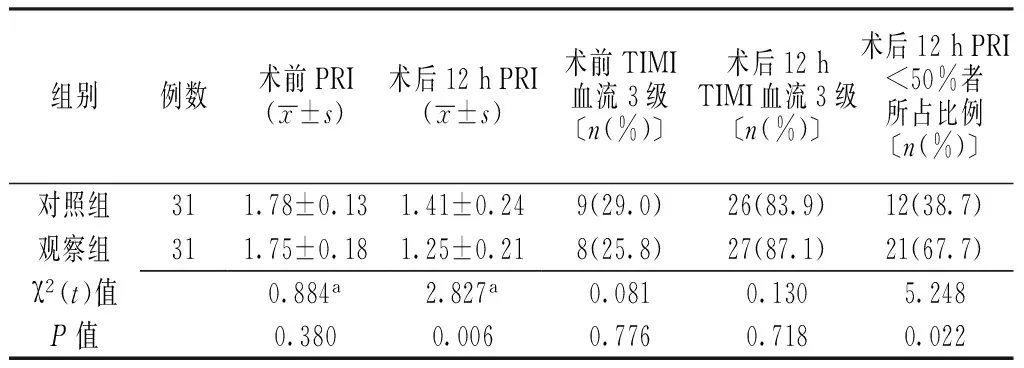
组别例数术前PRI(x±s)术后12hPRI(x±s)术前TIMI血流3级〔n(%)〕术后12hTIMI血流3级〔n(%)〕术后12hPRI<50%者所占比例〔n(%)〕对照组311.78±0.131.41±0.249(29.0)26(83.9)12(38.7)观察组311.75±0.181.25±0.218(25.8)27(87.1)21(67.7)χ2(t)值0.884a2.827a0.0810.1305.248P值0.3800.0060.7760.7180.022
注:a为t值;PRI=血小板反应指数

表1 两组患者一般资料比较
注:a为χ2值;1 mm Hg=0.133 kPa
2.2终点事件两组患者主要终点事件发生率及发生风险比较、次要终点事件发生率及发生风险比较,差异均无统计学意义(P>0.05);而观察组患者联合终点事件发生率及发生风险均低于对照组,差异均有统计学意义(P<0.05,见表3)。
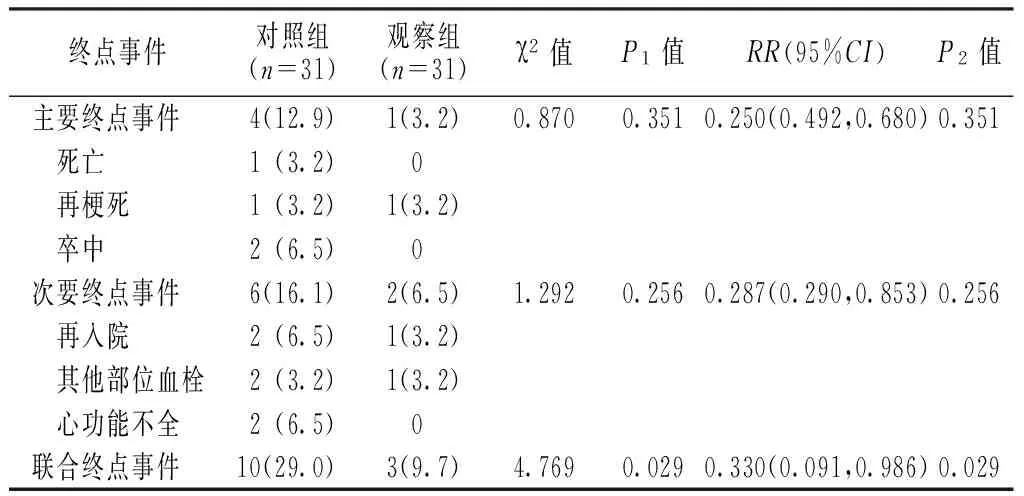
表3 两组患者终点事件发生情况比较〔n(%)〕
注:P1值为χ2值对应P值,P2值为RR值对应P值
3讨论
PCI是我国冠心病患者首选治疗方法,但其使缺血部位心肌重新恢复血运同时会因血运重建而导致缺血心肌再灌注损伤,这也是目前影响PCI效果的重要原因之一[8-9]。据文献报道,ACS患者PCI术后因再灌注损伤而导致的死亡或心力衰竭发生率约为20%[10];无复流、冠状动脉及其他部位血栓形成、支架内再狭窄、心功能不全等也会严重影响ACS患者PCI术后生存质量和预后。研究表明,血小板活性增强、血液处于高凝状态是ACS患者PCI术中或术后易产生微血栓、冠状动脉或其他部位血管栓塞并导致再狭窄的主要原因[11-12]。
普拉格雷为第三代噻吩并吡啶类抗血小板药物,可有效抑制P2Y12受体,具有体内代谢快、活性成分转化率高、抗血小板聚集作用强等优势。2011年ESC将普拉格雷列为非ST段抬高型心肌梗死(NSTEMI)、ACS和STEMI患者的治疗药物[13-15]。近年来有学者指出,普拉格雷在降低PCI术后患者再梗死及支架内血栓形成风险方面较氯吡格雷更具优势,虽然普拉格雷相关并发症发生风险会有所增高,但亚组分析结果显示出血并发症风险增高仅限于年龄>75岁、体质量<60 kg和有卒中病史的患者[16-17]。Kurz等[7]通过对9 502例ACS患者进行研究发现,普拉格雷联合PCI在年轻ACS患者中的应用效果较好,出血并发症的发生风险较低。
本研究结果显示,观察组患者术后12 h PRI低于对照组,术后12 h PRI<50%者所占比例高于对照组,说明普拉格雷能更快更强更持久地发挥抗血小板作用;随访1年发现,两组患者主要终点事件发生率及发生风险、次要终点事件发生率及发生风险间均无明显差异,而观察组患者联合终点事件发生率及发生风险均低于对照组,提示普拉格雷能有效降低ACS患者术后联合终点事件发生率,这与Verdoia等[4]研究结果一致。Saito等[18]通过对1 363例ACS患者进行回顾性分析发现,治疗24~48周后,普拉格雷联合阿司匹林组患者主要不良心血管事件发生率为9.4%,低于氯吡格雷联合阿司匹林组的11.8%。
综上所述,普拉格雷作为新一代强效抗血小板药物,能有效抑制血小板聚集,降低ACS患者术后联合终点事件发生率,具有较好的临床应用前景。但本研究为回顾性研究,且排除了糖尿病、肝肾功能不全、心力衰竭等患者,可能存在一定的选择偏倚,普拉格雷的应用效果仍有待于在今后的研究中进一步证实。
参考文献
[1]De Luca G,Verdoia M,Schaffer A,et al.Switching from high-dose clopidogrel to prasugrel in ACS patients undergoing PCI:a single-center experience[J].J Thromb Thrombolysis,2014,38(3):388-394.
[2]Levine GN,Jeong YH,Goto S,et al.Expert consensus document:World Heart Federation expert consensus statement on antiplatelet therapy in East Asian patients with ACS or undergoing PCI[J].Nat Rev Cardiol,2014,11(10):597-606.
[3]胡云东,胡敏,曲波,等.国产氯吡格雷用于经皮冠状动脉介入治疗的可行性及安全性研究[J].实用心脑肺血管病杂志,2015,23(2):21-24.
[4]Verdoia M,Barbieri L,Suryapranata H,et al.Switching from Clopidogrel to Prasugrel in patients undergoing PCI:A meta-analytic overview[J].Platelets,2015.[Epub 2015 May 13]
[5]Zhou BD,Zu LY,Mi L,et al.An analysis of patients receiving emergency CAG without PCI and the value of GRACE score in predicting PCI possibilities in NSTE-ACS patients[J].J Geriatr Cardiol,2015,12(3):246-250.
[6]杨军,程文伟.非ST抬高急性冠脉综合征患者经皮冠脉介入治疗术后氯吡格雷使用方法的探讨[J].实用心脑肺血管病杂志,2009,17(2):83-85.
[7]Kurz DJ,Radovanovic D,Seifert B,et al.Comparison of prasugrel and clopidogrel-treated patients with acute coronary syndrome undergoing percutaneous coronary intervention:A propensity score-matched analysis of the Acute Myocardial Infarction in Switzerland(AMIS)-Plus Registry[J].Eur Heart J Acute Cardiovasc Care,2015.[ Epub 2015 Jan 22]
[8]Trenk D,Stone GW,Gawaz M,et al.A randomized trial of prasugrel versus clopidogrel in patients with high platelet reactivity on clopidogrel after elective percutaneous coronary intervention with implantation of drug-eluting stents:results of the TRIGGER-PCI(Testing Platelet Reactivity In Patients Undergoing Elective Stent Placement on Clopidogrel to Guide Alternative Therapy With Prasugrel)study[J].J Am Coll Cardiol,2012,59(24):2159-2164.
[9]陈青,米树华,周芸,等.冠心病经皮冠状动脉介入治疗患者糖化血清清蛋白水平与冠状动脉病变关系的研究[J].中国全科医学,2014,17(4):418-421.
[10]Sardella G,Calcagno S,Mancone M,et al.Comparison of therapy with Ticagrelor,Prasugrel or high Clopidogrel dose in PCI patients with high on treatment platelet reactivity and genotype variation.TRIPLETE RESET trial[J].Int J Cardiol,2015,194:60-62.
[11]Zeymer U,Mochmann HC,Mark B,et al.Double-blind,randomized,prospective comparison of loading doses of 600 mg clopidogrel versus 60 mg prasugrel in patients with acute ST-segment elevation myocardial infarction scheduled for primary percutaneous intervention:the ETAMI trial(early thienopyridine treatment to improve primary PCI in patients with acute myocardial infarction)[J].JACC Cardiovasc Interv,2015,8(1 Pt B):147-154.
[12]黄觊,钱海燕,李志忠,等.巴替非班在急性冠脉综合征患者经皮冠状动脉介入治疗中的应用价值[J].疑难病杂志,2013, 12(1):10-12.
[13]Olson WH,Ma YW,Crivera C,et al.Economic outcomes with prasugrel versus clopidogrel in acute coronary syndrome patients:observations from prasugrel users and matched clopidogrel users[J].J Med Econ,2015.[ 2015 Sep 25]
[14]Montalescot G,Collet JP,Ecollan P,et al.Effect of prasugrel pre-treatment strategy in patients undergoing percutaneous coronary intervention for NSTEMI:the ACCOAST-PCI study[J].J Am Coll Cardiol,2014,64(24):2563-2571.
[15]Alexopoulos D.Reloading patients chronically treated with P2Y12 inhibitors and presenting with ACS/PCI:facing a crossroad?[J].Int J Cardiol,2013,167(1):292-293.
[16]Bernlochner I,Mayer K,Morath T,et al.High frequency of CYP2C19*2 carriers in PCI-treated patients switched over from clopidogrel to prasugrel based on platelet function monitoring[J].Platelets,2013,24(6):500-502.
[17]Ponniah JP,Shamsul AS,Adam BM.Predictors of mortality in patients with Acute Coronary Syndrome(ACS)undergoing Percutaneous Coronary Intervention(PCI):Insights from National Cardiovascular Disease Database(NCVD),Malaysia[J].Med J Malaysia,2012,67(6):601-605.
[18]Saito S,Isshiki T,Kimura T,et al.Efficacy and safety of adjusted-dose prasugrel compared with clopidogrel in Japanese patients with acute coronary syndrome:the PRASFIT-ACS study[J].Circ J,2014,78(7):1684-1692.
(本文编辑:鹿飞飞)
Application Effect of Prasugrel in Acute Coronary Syndrome Patients Treated by PCI
WANGShu-yuan,HUANGJia-zhuo.
DepartmentofCardiovascularMedicine,theFirstPeople′sHospitalofZhaoqing,Zhaoqing526020,China
【Abstract】ObjectiveTo observe the application effect of prasugrel in acute coronary syndrome patients treated by PCI.MethodsFrom November 2013 to July 2014,a total of 62 inpatients with acute coronary syndrome were selected in the Department of Cardiovascular Medicine,the First People′s Hospital of Zhaoqing,and they were randomly divided into control group and observation group,each of 31 cases.Patients of both groups received PCI after admission,patients of control group received oral aspirin combined with clopidogrel before 3 days of PCI,and continuously received oral clopidogrel for 1 year after PCI;patients of observation group received oral aspirin combined with prasugrel before 3 days of PCI,and continuously received oral prasugrel for 1 year after PCI.Platelet reactivity index(PRI) and the proportion of patients with 3-grade TIMI flow before PCI and after 12 hours of PCI,and the proportion of patients with PRI less than 50% were compared between the two groups;patients of the two groups were followed up for 1 year to observe the incidence of primary end point events,secondary end point events and clinical endpoints.ResultsNo statistically significant differences of PRI or the proportion of patients with 3-grade TIMI flow was found between the two groups before PCI(P>0.05);after 12 hours of PCI,PRI of observation group was statistically significantly lower than that of control group,the proportion of patients with PRI less than 50% of observation group was statistically significantly higher than that of control group,while no statistically significant differences of the proportion of patients with 3-grade TIMI flow was found between the two groups(P>0.05).No statistically significant differences of incidence or occurrence risk of primary end point events or secondary end point events was found between the two groups(P>0.05),while incidence and occurrence risk of clinical endpoints of observation group was statistically significantly lower than those of control group,respectively(P<0.05).ConclusionPrasugrel can effectively inhibit the platelet aggregation and reduce the incidence of clinical endpoints of acute coronary syndrome patients undergoing PCI,has relatively good application prospect on clinic.
【Key words】Acute coronary syndrome;Angioplasty,balloon,coronary;Prasugrel;Clopidogrel;Treatment outcome
【中图分类号】R 542.2
【文献标识码】B
doi:10.3969/j.issn.1008-5971.2016.05.030
(收稿日期:2015-12-30;修回日期:2016-04-29)
