结直肠腺瘤切除术后复发风险研究
2014-01-19黄应龙苏秉忠
黄应龙 苏秉忠 姜 泊 龚 伟
结直肠腺瘤切除术后复发风险研究
黄应龙1苏秉忠1姜 泊2龚 伟2
目的探讨结直肠腺瘤切除后不同时间段腺瘤复发风险。方法对1976年至2007年在广州南方医院消化内镜中心所有经结肠镜下诊断并切除腺瘤患者的随访结果进行回顾性总结,根据初次结肠镜检查患者腺瘤特征对患者进行分层,即非高危腺瘤和高危腺瘤患者,分析不同患者在不同时间段的腺瘤复发风险。结果1 356例腺瘤患者在腺瘤切除术后1年到20年间接受了3次以上的有效随访结肠镜检查。基础腺瘤(初次结肠镜检查中发现腺瘤)为高危腺瘤患者,在1~3年、3~5年、5~10年和10~20年4个时间段内高危腺瘤的累计复发率分别是3.8%、13.1%、34.7%和52.0%,任意腺瘤的复发率分别是32.6%、58.1%、75.8%和86.2%。基础腺瘤为非高危腺瘤患者,高危腺瘤的累计复发率分别是0.9%、3.9%、5.8%和29.2%,任意腺瘤的复发率为11.5%、28.9%、45.3%和62.5%。两种类型基础腺瘤(即高危腺瘤和非高危腺瘤)患者比较,复发高危腺瘤或任意腺瘤的累计风险均存在很大差异(P=0.000)。结论腺瘤切除后复发腺瘤或高危腺瘤累计风险随时间延长明显增加,高危腺瘤患者腺瘤切除后复发风险在不同时间段均明显高于非高危腺瘤患者。
结直肠腺瘤;复发;结肠镜检查
在中国,大肠癌是第四大常见恶性肿瘤,在癌症死亡病因中排第五位[1]。随着中国饮食结构变化,近年来大肠癌的发病率呈逐年上升趋势。大肠癌的发生、发展是一分阶段的动态演进过程。研究表明绝大多数散发型大肠癌是由腺瘤发展而来,这就为大肠癌的预防提供了机会。多项研究证实结肠镜作为筛查和治疗大肠肿瘤的有效方法明显降低了大肠癌的发病率和死亡率[2-3]。而腺瘤患者在腺瘤完整切除后仍有再发生腺瘤甚至癌的可能[4-5]。因此,为了进一步降低大肠癌发病率,腺瘤切除后结肠镜的随访显得尤为重要。而我国目前就结肠腺瘤切除术后不同时间段腺瘤复发情况以及如何进行结肠镜随访均缺乏系统研究,本研究旨在对此问题进行研究,希望为我国结肠镜随访方案的制定奠定基础。
资料与方法
一、病例收集
结直肠腺瘤患者登记记录从1976年开始建立。所有在1976年至2007年经结肠镜下诊断并切除腺瘤的特征及患者特征被记录在广州南方医院消化内镜中心内镜检查病历档案及电子内镜病历记录系统。包括腺瘤的大小、部位、数量、形态和组织病理结果,以及患者年龄、性别和随访结肠镜检查结果。
二、病例入选标准
①年龄>20岁;②每次结肠镜检查均为完整结肠镜检查;③患者在初次结肠镜检查后半年内至少接受过一次结肠镜复查,其目的是为了祛除初次结肠镜检查中漏诊的腺瘤;④能够获得完整的随访结肠镜检查发现腺瘤的特征包括腺瘤大小、数量及组织病理学结果等终点资料。
具有家族性腺瘤性息肉病、炎症性肠病及大肠癌病史的患者除外。
三、完整结肠镜检查
完整结肠镜检查必须包括下列三部分内容:结肠镜到达盲肠,良好的肠道准备,结肠镜检查中所发现腺瘤均通过内镜下息肉切除术或黏膜切除术完全切除。第一次结肠镜检查后半年内进行的所有结肠镜复查所发现腺瘤均被认为是第一次检查漏诊腺瘤,归类为第一次结肠镜检查结果。随访结肠镜检查中在以前腺瘤切除形成瘢痕位置发现的腺瘤被认为是内镜切除不完全的局部残留腺瘤。当在既往腺瘤切除形成的瘢痕位置无腺瘤成份残留则称为完整切除。复发腺瘤是指在随访结肠镜检查中所发现的异时腺瘤。腺瘤完整切除六个月以后的结肠镜随访中发现腺瘤或高危腺瘤作为随访终点,发现腺瘤或高危腺瘤的时间或最后一次结肠镜检查时间作为随访终止时间。随访间期至少在一年以上,随访时间分类偏差不超过6个月。
四、资料分析方法
在研究期间,我们分析了所有腺瘤切除患者的内镜报告和病理报告,并收集腺瘤的大小、形态、部位、数目、病理等特征的资料以及患者年龄、性别等资料。腺瘤的大小是通过结肠镜活检钳张开口径大小(6 mm)或通过测量切除标本最大直径来衡量。部位分为近端结肠、远端结肠和直肠。近端结肠包括盲肠、升结肠、肝曲、横结肠、脾区,远端结肠包括降结肠、乙状结肠和直肠。腺瘤的形态分为两类即隆起型和非隆起型。非隆起型腺瘤根据巴黎肿瘤内镜下形态分类进一步分为平坦浅表型、平坦隆起型和平坦凹陷型[6]。所有腺瘤组织病理由一名消化病理专家根据世界卫生组织结直肠肿瘤分类进行审阅[7]。多发腺瘤患者的分类是按照腺瘤的大小、部位及组织学分别以最大腺瘤、最近端部位以及最高病理形态腺瘤进行分类。高危腺瘤是指具有下列特征的腺瘤:直径大于10 mm的腺瘤,绒毛状腺瘤(含绒毛成分大于25%)或伴高级别瘤变腺瘤。非高危腺瘤是指直径小于10 mm的管状腺瘤。任意腺瘤是指包括高危腺瘤和非高危腺瘤的所有腺瘤。
五、统计分析
按照初次结肠镜检查发现腺瘤的特征对患者进行危险分层,即高危腺瘤患者和非高危腺瘤患者,通过Kaplan-Meier生存分析法评价不同患者复发任意腺瘤和高危腺瘤的累计风险。P值小于0.05认为结果具有统计学意义。所有数据分析采用SPSS 13.0软件包和SAS 9.12软件包完成。
结果
一、患者初次结肠镜检查结果
6 462例腺瘤患者经内镜下腺瘤切除,2 484例患者接受了随访结肠镜检查(图1)。在这些随访患者中,1 002例只接受了一次随访,105例为炎症性肠病、家族性腺瘤性息肉病和Peutz-Jeghers综合征患者。另外21例患者随访结肠镜检查不完整。总共1 356例腺瘤患者在腺瘤切除术后1~20年接受了有效的随访结肠镜检查。1 356例有效结肠镜随访患者中,男性863例,女性493例。初次结肠镜检查时平均年龄为(52.4±12.5)岁(20~84岁)。初次结肠镜检查中非高危腺瘤患者714例(52.7%),高危腺瘤患者642例(47.3%)。808例(59.6%)患者仅有单发腺瘤,528例(40.4%)为多发腺瘤患者。

图1 患者的入选及结果(FAP:家族性腺瘤性息肉病;IBD:炎症性肠病;P-J:Peutz-Jeghers综合征)
二、结直肠腺瘤的累计复发率
在不同时间段的结肠镜随访中任意腺瘤及高危腺瘤的累计复发率在表1中列出。对于在初次结肠镜检查中发现腺瘤的所有患者,在腺瘤切除后1~3年、3~5年、5~10年和10~20年四个时间段内,高危腺瘤的累计复发率分别是2.2%、8.6%、21.0%和37.7%,而任意腺瘤的复发率分别为21.1%,43.9%,61.3%和75.5%。当基础腺瘤(初次结肠镜检查中发现腺瘤)按高危腺瘤和非高危腺瘤分类后,对于高危腺瘤患者,在1~3年、3~5年、5~10年和10~20年四个时间段内高危腺瘤的累计复发率分别是3.8%、13.1%、34.7%和52.0%,任意腺瘤的复发率分别是32.6%、58.1%、75.8%和86.2%。而对于基础腺瘤为非高危腺瘤患者,高危腺瘤的累计复发率分别是0.9%、3.9%、5.8%和29.2%,任意腺瘤的复发率为11.5%、28.9%、45.3%和62.5%。两种类型基础腺瘤即高危腺瘤和非高危腺瘤比较,复发高危腺瘤或任意腺瘤的累计风险均存在很大差异(P=0.000)(图2)。
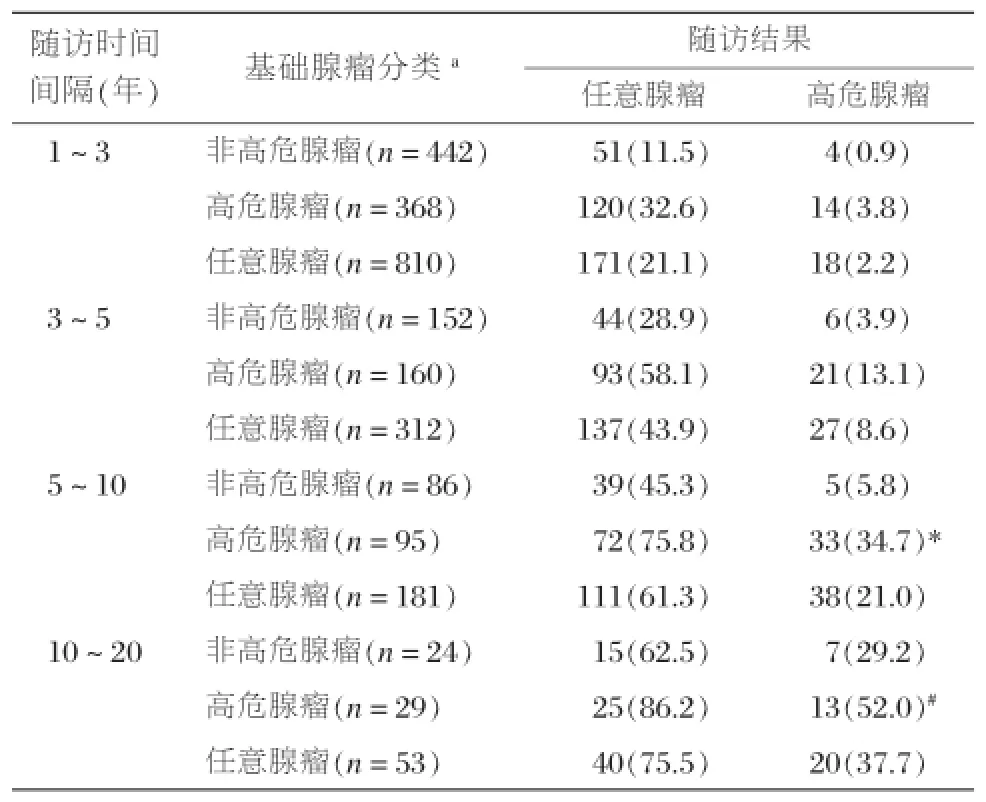
表1 不同类型基础腺瘤在结肠镜随访中任意腺瘤及高危腺瘤的累计复发率[n(%)]
讨论

图2 初次结肠镜检查为高危腺瘤和非高危腺瘤患者在不同随访时间复发的累计风险
多项研究表明第一次结肠镜检查发现腺瘤患者在腺瘤完整切除后3~5年再发腺瘤的比例约20%~50%,其中20%的复发腺瘤为高危腺瘤[2-3,8-11],约0.5%~5%进展为浸润型癌[12-14]。为了能够更好的在有效随访时间内发现属于可治愈期的高危腺瘤及早期癌,当前美国结肠镜随访指南提出根据初次结肠镜检查腺瘤的特征决定结肠镜随访时间间隔[5]。然而,由于结肠镜检查中漏诊问题的存在以及内镜医师对大肠肿瘤自然发展史的认识差异,该随访规范很难在结肠镜检查实践中得到应用[15-16]。而且由于人种的不同、饮食结构等的不同,西方国家的随访规范能否直接应用于中国人群一直是困扰中国内镜医生的主要问题。当前,在中国没有规范而可执行的结肠镜随访方案。大多数中国内镜医师认为腺瘤患者在腺瘤切除后一年内应接受结肠镜随访,使得结肠镜检查数量猛增。如此频繁的结肠镜检查势必导致大量的医疗资源浪费。而对于中国人群中的结直肠腺瘤患者在腺瘤完整切除后不同时间腺瘤的复发率以及真正的随访时间间隔应该多长需要我们进一步证明。
国外研究报道腺瘤患者在腺瘤切除后的结肠镜随访中腺瘤复发率明显高于初次结肠镜检查正常的患者[11,17-19]。因此,对腺瘤患者的结肠镜随访在进一步降低大肠癌发病率中扮演重要角色。我们的研究提供了中国南方人群腺瘤患者在腺瘤切除后的不同时间段结肠镜随访中腺瘤和高危腺瘤的复发率。近年来,多向研究结果表明腺瘤患者在腺瘤切除3~4年后随访腺瘤的复发率约15%~60%,其中高危腺瘤大约占复发腺瘤的15%[2,8,20-21]。Bertario等[22]对腺瘤患者在腺瘤完整切除后的2年、3年、5年和10年进行结肠镜随访,腺瘤的复发率分别为18%、23%、31%和40%。我们的结果与其结果相似。在我们的研究中,初次结肠镜检查为高危腺瘤的患者在腺瘤切除后的不同随访时间段任意腺瘤和高危腺瘤的复发率明显高于初次结肠镜检查为非高危腺瘤的患者。为了进一步证实这一结果,我们对两种不同类型基础腺瘤患者在腺瘤切除后复发任意腺瘤或高危腺瘤的累积复发风险通过Kaplan-Meier生存分析方法对其进行了评估,结果完全支持这一研究结论。这一结果也与近年来国外的多项研究结果一致[11,23-25]。从另一角度也说明当前西方国家关于对基础腺瘤分类为高危腺瘤和非高危腺瘤而进行的结肠镜随访中腺瘤复发率的评价也适用于中国南方人群。
当然,我们的研究是一项回顾性研究,对于其他影响腺瘤复发的因素我们未能全面考虑,比如患者性别、年龄及家族史等,希望将来能进行多中心前瞻性研究对我国结直肠腺瘤切除术后腺瘤复发风险进行全面研究。
1Zheng S,Cai S.Colorectal cancer epidemiology and prevention study in China.The Chinese-German Journal of Clinical Oncology, 2003;2(2):72-75.
2Zauber AG,Winawer SJ,O′Brien MJ,et al.Colonoscopic polypectomy and long-term prevention of colorectal-cancer deaths.N Engl J Med,2012,366(8):687-696.
3Winawer SJ,Zauber AG,Ho MN,et al.Prevention of colorectal cancer by colonoscopic polypectomy.The National Polyp Study Workgroup.N Engl J Med,1993,329(27):1977-1981.
4Lieberman DA,Rex DK,Winawer SJ,et al.Guidelines for colonoscopy surveillance after screening and polypectomy:a consensus update by the US Multi-Society Task Force on Colorectal Cancer.Gastroenterology,2012,143(3):844-857.
5Rex DK,Kahi CJ,Levin B,et al.Guidelines for colonoscopy surveillance after cancer resection:a consensus update by the American Cancer Society and the US Multi-Society Task Force on Colorectal Cancer.Gastroenterology,2006;130(6):1865-1871.
6Cottet V,Jooste V,Fournel,et al.Long-term risk of colorectal cancer after adenoma removal:a population-based cohort study,Gut,. 2012,61(8):1180-1186.
7Hamilton SR,Vogelstein B,Kudo S.Carcinoma of the colon and rectum.In:Hamilton SR,Altonen IA eds,Tumours of the digestive system WHO classification of tumors.Lyon:IARC Press,2000: 113-114.
8van Heijningen EM,Lansdorp-Vogelaar I,Kuipers EJ,et al.Features of adenoma and colonoscopy associated with recurrent colorectal neoplasia based on a large community-based study.Gastroenterology,2013,144(7):1410-1418.
9Schatzkin A,Lanza E,Corle D,et al.Lack of effect of a low-fat, high-fiber diet on the recurrence of colorectal adenomas.Polyp Prevention Trial Study Group.N Engl J Med,2000,342(16):1149-1155.
10 Baron JA,Cole BF,Sandler RS,et al.A randomized trial of aspirin to prevent colorectal adenomas.N Engl J Med,2003,348(10)891-899.
11 Lieberman DA,Weiss DG,Harford WV,et al.Five-year colon surveillance after screening colonoscopy.Gastroenterology,2007, 133(4):1077-1085.
12 Pabby A,Schoen RE,Weissfeld JL,et al.Analysis of colorectal cancer occurrence during surveillance colonoscopy in the dietary Polyp Prevention Trial.Gastrointest Endosc,2005,61(3):385-391.
13 Bressler B,Paszat LF,Chen Z,et al.Rates of new or missed colorectal cancers after colonoscopy and their risk factors:a populationbased analysis.Gastroenterology,2007,132(1):96-102.
14 Leung K,Pinsky P,Laiyemo AO,et al.Ongoing colorectal cancer risk despite surveillance colonoscopy:the Polyp Prevention Trial Continued Follow-up Study.Gastrointest Endosc,2010,71(1):111-117.
15 Heresbach D,Barrioz T,Lapalus MG,et al.Miss rate for colorectal neoplastic polyps:a prospective multicenter study of back-to-back video colonoscopies.Endoscopy,2008,40(4):284-290.
16 van Rijn JC,Reitsma JB,Stoker J,et al.Polyp miss rate determined by tandem colonoscopy:a systematic review.Am J Gastroenterol, 2006,101(2):343-350.
17 Leung WK,Lau JY,Suen BY,et al.Repeat-screening colonoscopy 5 years after normal baseline-screening colonoscopy in average-risk Chinese:a prospective study.Am J Gastroenterol,2009,104(8): 2028-2034.
18 Imperiale TF,Glowinski EA,Lin-Cooper C,et al.Five-year risk of colorectal neoplasia after negative screening colonoscopy.N Engl J Med,2008,359(12):1218-1224.
19 Huang Y,Li X,Wang Z,et al.Five-year risk of colorectal neoplasia after normal baseline colonoscopy in asymptomatic Chinese Mongolian over 50 years of age.Int J Colorectal Dis,2012,27(12): 1651-1656.
20 Noshirwani KC,van Stolk RU,Rybicki LA,et al.Adenoma size and number are predictive of adenoma recurrence:implications for surveillance colonoscopy.Gastrointest Endosc,2000,51(4 Pt 1): 433-437.
21 Nusko G,Mansmann U,Kirchner T,et al.Risk related surveillance following colorectal polypectomy.Gut,2002,51(3):424-428.
22 Bertario L,Russo A,Sala P,et al.Predictors of metachronous colorectal neoplasms in sporadic adenoma patients.Int J Cancer,2003, 105(1):82-87.
23 Laiyemo AO,Murphy G,Albert PS,et al.Postpolypectomy colonoscopy surveillance guidelines:predictive accuracy for advanced adenoma at 4 years.Ann Intern Med,2008,148(6):419-426.
24 Loeve F,van Ballegooijen M,Boer R,et al.Colorectal cancer risk in adenoma patients:a nation-wide study.Int J Cancer,2004,111(1): 147-151.
25 Martínez ME,Baron JA,Lieberman DA,et al.A pooled analysis of advancedcolorectalneoplasiadiagnosesaftercolonoscopic polypectomy.Gastroenterology,2009,136(3):832-841.
Risk of adenoma recurrence after colorectal polypectomy
HANG Ying-long1,SU Bing-zhong1,JIANG Bo2,GONG Wei2.1)Department of Gastroenterology,Affiliated Hospital of Inner Mongolia Medical University,Huhhot,010050;2)Department of Gastroenterology,Nanfang Hospital,Southern Medical University, Guangzhou 510515
Subject To analyze the risk of adenoma recurrence after colorectal polypectomy during different time of surveillance.Method All cases of colorectal adenoma removed by colonoscopy for the first time were documented in the endoscopic center of the Department of Gastroenterology,Nanfang Hospital, Guangzhou,and the characteristics of every patient were summarized.According to the characteristics of adenoma removed,the patients were classified into non-advanced adenoma and advanced adenoma.Meanwhile, the risk of adenoma recurrence at defferent time was analyzed.Result A total of 1 356 patients underwent endoscopic polypectomy and completed three or more endoscopic surveillances from one year to twenty years after polypectomy.When baseline adenoma were stratified by advanced and non-advanced adenoma,the cumulative recurrence rates of advanced adenoma were 3.8%,13.1%,34.7%and 52.0%in patients with advanced adenoma at baseline during four different surveillance intervals,whereas,0.9%,3.9%,5.8%and 29.2%in patients with non-advanced adenoma at baseline.For patients with advanced adenoma at baseline,the cumulative recurrence rates of any adenoma during these same four different surveillance intervals were 32.6%,58.1%, 75.8%,and 86.2%,respectively,as compared with those of 11.5%,28.9%,45.3%,and 62.5%for patients with non-advanced adenoma at baseline.In terms of the cumulative risk of the recurrence of advanced adenoma or the recurrence of any adenoma at the surveillance examination,there was a significant difference between patients with advanced adenoma and those with non-advanced adenoma at baseline.Conclusion The cumulative risk of the recurrence of any adenoma and advanced adenoma during surveillance significantly increase with time prolonged.The rate of adenoma recurrence after polypectomy for patients with advanced adenoma at baseline are significantly higher than that for patients with non-advanced adenoma at baseline.
Colorectal adenoma;Recurrence;Colonoscopy
2014-06-26)
(本文编辑:李钊)
10.3961/j.issn.1672-2159.2014.04.007
1 010050内蒙古医科大学附属医院;
2 510515南方医科大学南方医院消化内科
