Primary hepatic carcinosarcoma
2011-07-07MehmetelikbilekKemalDenizEdipTorunTarArtErsinzaslankkebrahimKarahanTahirErcanPatroluandmerzbak
Mehmet Çelikbilek, Kemal Deniz, Edip Torun, Tarık Artış, Ersin Özaslan, Ökkeş İbrahim Karahan, Tahir Ercan Patıroğlu and Ömer Özbakır
Kayseri, Turkey
Case Report
Primary hepatic carcinosarcoma
Mehmet Çelikbilek, Kemal Deniz, Edip Torun, Tarık Artış, Ersin Özaslan, Ökkeş İbrahim Karahan, Tahir Ercan Patıroğlu and Ömer Özbakır
Kayseri, Turkey
BACKGROUND:Primary hepatic carcinosarcoma is a rare malignant tumor containing an intimate mixture of carcinomatous and sarcomatous elements. Reports on risk factors, epidemiology, and pathogenesis of the tumor as well as the experience in its treatment are limited.
METHOD:We present a case of primary carcinosarcoma of the liver in a 69-year-old man who complained of right hypochondrial pain and weight loss for two months.
RESULTS:Magnetic resonance imaging revealed a 14×12 cm mass in segments 7-8 and 4 of the liver with vena hepatica invasion. An ultrasonography-guided biopsy showed osteoid tissue without osteoblastic rimming. Vascular structures accompanied the osteoid tissue. The patient underwent surgery after a diagnosis of hemangioma. Intraoperative frozen sections revealed a carcinosarcoma associated with an osteosarcoma and cholangiocellular carcinoma components.
CONCLUSIONS:Preoperative diagnosis of this rare primary hepatic malignant tumor may be difficult by biopsy owing to intratumoral heterogeneity. Highly mature areas of the osteosarcomatous component may lead to misdiagnosis of metaplastic bone tissue. Clinicopathologic features of this rare entity are discussed.
(Hepatobiliary Pancreat Dis Int 2011; 10: 101-103)
carcinosarcoma; liver neoplasms; osteosarcoma; cholangiocarcinoma
Introduction
The World Health Organization (WHO) defines primary hepatic carcinosarcoma as a malignant tumor containing an intimate mixture of carcinomatous and sarcomatous elements.[1]Hepatic carcinosarcoma is a rare entity with poor prognosis. Up to the present, approximately 20 cases of primary hepatic carcinosarcoma have been reported in the English literature. The studies on risk factors, epidemiology, pathogenesis of the tumor as well as the experience in its treatment are limited. We present a case of primary hepatic carcinosarcoma containing cholangiocellular carcinoma and osteosarcoma. Clinicopathologic features of this rare entity are discussed.
Case report
A 69-year-old man was admitted to another hospital because of right hypochondrial pain and 8 kg weight loss for two months. The patient was referred to our hospital with radiologic results and the results of ultrasonography of the abdomen, which revealed a 14-cm heterogeneous hypoechoic mass with calcification and cystic areas in segments 7-8 of the liver, and computed tomography (CT) scan of the abdomen, which revealed an 11-cm heterogeneous solid mass with calcification in the right hepatic lobe. A physical examination revealed right upper abdomen tenderness with palpation. The medical history of the patient included regular hypertension. The laboratory data at our center were: total bilirubin 2.3 mg/dl (0.3-1.2), serum alanine aminotransferase 47 IU/L (0-35), serum aspartate aminotransferase 80 IU/L (0-31), alkaline phosphatase 311 IU/L (30-120), and γ-glutamyl-transpeptidase 76 IU/L (0-38). The tumor markers, carcinoembryonic antigen (CEA), serum α-fetoprotein (AFP), and carbohydrase antigen 19-9 (CA19-9), were within the normal range. Hepatitis B surface antigen, hepatitis B core antibody, and hepatitis D antibody were positive. HBV DNA was <150 IU/ml (normal). Upper gastrointestinal endoscopy revealed noesophageal varices. Magnetic resonance imaging (MRI) revealed a heterogeneous hypointensity on the T1-weighted images and heterogeneous hyperintensity on the T2-weighted images of a 14×12 cm mass in segments 7-8 and 4 of the liver with vena hepatica invasion (Fig. 1). Thoracic CT was normal.
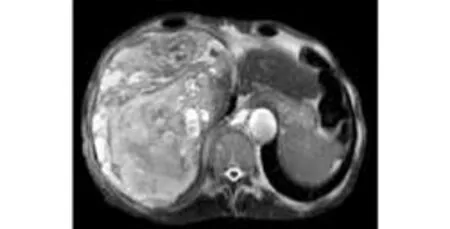
Fig. 1. MRI showing a 14×12 cm mass in segments 7-8 and 4 of the liver with vena hepatica invasion.

Fig. 2. Fragments of the large tumor composed of bony tissue and highly necrotic hemorrhagic tumor tissue.
An ultrasonography-guided biopsy showed osteoid tissue without osteoblastic rimming. Vascular structures were accompanied with the osteoid tissue. The patient underwent surgery after a presumptive diagnosis of hemangioma with metaplastic osteoid tissue.
Highly necrotic hemorrhagic tumor tissue was observed at the right lobe during laparotomy. Large amounts of bony tissue were present in the central area of the tumor mass (Fig. 2). Intraoperative frozen sections revealed the diagnosis of carcinosarcoma.
Light microscopic examination of the tumor showed that it was composed of sarcomatous and epithelial components. The sarcomatous areas were consistent with osteosarcoma and made up the major component of the tumor. There were small foci of cholangiocellular carcinoma as the carcinomatous component (Fig. 3). Immunohistochemically, pancytokeratin and cytokeratin 7 were positive in the cholangiocellular component. Vimentin was positive in the sarcomatous areas. Both components of the tumor were negative for HepPar, CD31, actin, desmin, S100, CD117, CK19, and CDX2.

Fig. 3. Light microscopy showing the sarcomatous component consisting of osteosarcoma and undifferentiated sarcomatous elements (A, B) with adenoid structures (HE, original magnification ×200(A) , ×100(B)). (C) Cytokeratin positivity in carcinomatous areas (HE, original maginification×100) and (D) vimentin positivity in sarcomatous areas (HE, original magnification ×100).
The patient died five months after operation.
Discussion
Hepatic carcinosarcoma is a rare disease and the term carcinosarcoma is defined by the WHO classification as a malignant mixed tumor containing both carcinomatous (either hepatocellular or cholangiocellular) and sarcomatous components. According to Ishak et al,[2]mixed liver tumors associated with well-differentiated sarcomatous and carcinomatous elements in the absence of hepatocellular carcinoma are designated as non-hepatocytic malignant tumors. In our patient, the carcinomatous component was pathologically cholangiocarcinoma and the sarcomatous component was osteosarcoma. Only one reported case of hepatic carcinosarcoma included cholangiocellular and osteosarcoma components similar to ours.[3]According to the WHO definition, our case is considered to be a primary hepatic carcinosarcoma.
The pathogenesis of hepatic carcinosarcoma is controversial. Some authors suggest that the carcinomatousand sarcomatous elements of this tumor originate from single stem cells.[4]Among others, the most accepted explanation for the pathogenesis of hepatic carcinosarcomas is that the carcinomatous elements transform to sarcomatous elements by a metaplastic process. According to this pathogenetic mechanism, researchers termed the tumor "carcinoma with sarcomatous differentiation (metaplasia)".[5]
Clinically, our patient was admitted for upper abdominal pain and weight loss similar to the previous cases reported. Hepatitis B surface antigen and hepatitis D antibody were positive with no sign of cirrhosis. Tumor markers including AFP, CEA, and CA19-9 were within normal ranges. Ultrasonography, CT, and MRI showed no distinctive characteristics compared to ordinary liver cancer. The literature revealed that a final diagnosis of liver carcinosarcoma was made during exploratory laparotomy, after operation, or at autopsy. Ultrasonographically-guided biopsy in our patient did not lead to a definitive decision. Intraoperative and postoperative histopathologic and immunohistochemical studies were conducted to reach a diagnosis.
The highly invasive and metastatic hepatic carcinosarcoma often lead to a poor prognosis, and this aggressive behavior belongs to a sarcomatoid variant. Most of the reported cases had a short life-span after initial presentation or diagnosis.[4]Our patient showed vena hepatica invasion on MRI with no intrahepatic and extrahepatic metastasis.
In conclusion, carcinosarcoma contains two components, and preoperative diagnosis is difficult to make by clinical, radiologic, and histologic features. We present a rare entity with cholangiocellular and osteosarcomatous components diagnosed intraoperatively.
Funding:None.
Ethical approval:Not needed.
Contributors:CM, DK and TE wrote the first draft of this report. All authors contributed to the intellectual context and approved the final version. ÖÖ is the guarantor.
Competing interest:No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
1 Ishak KG, Anthony PP, Niederau C, Nakanuma Y. Mesenchymal tumours of the liver. In: Stanley RH, Lauri AA, editors. WHO International Histological Classification of Tumours, Pathology & Genetics of the Tumours of the Digestive System. Lyon: IARC Press; 2000:198.
2 Ishak KG, Goodman ZD, Stocker JT. Malignant mesenchymal tumors. In: Rosai J, Sobin LH, editors. Tumors of the Liver and Intrahepatic Bile Ducts. Atlas of Tumor Pathology; 3rd series, fascicle 31. Washington, DC: Armed Forces Institute of Pathology; 2001.
3 Kwon JH, Kang YN, Kang KJ. Carcinosarcoma of the liver: a case report. Korean J Radiol 2007;8:343-347.
4 Thompson L, Chang B, Barsky SH. Monoclonal origins of malignant mixed tumors (carcinosarcomas). Evidence for a divergent histogenesis. Am J Surg Pathol 1996;20:277-285.
5 Lao XM, Chen DY, Zhang YQ, Xiang J, Guo RP, Lin XJ, et al. Primary carcinosarcoma of the liver: clinicopathologic features of 5 cases and a review of the literature. Am J Surg Pathol 2007;31:817-826.
January 18, 2010
Accepted after revision September 28, 2010
Author Affiliations: Department of Gastroenterology (Çelikbilek M, Torun E and Özbakır Ö), Department of Pathology (Deniz K and Patıroğlu TE), Department of Surgery (Artış T), Department of Internal Medicine (Özaslan E), and Department of Radiology (Karahan Öİ), Erciyes University, Medical School, Kayseri, Turkey
Mehmet Çelikbilek, MD, Gültepe Mahallesi Gülhisar Sokak Örten sitesi C Blok No: 9/12, Melikgazi/Kayseri, Turkey (Tel: +90-505-661-53-75; Fax: +90-352-437-52-73; Email: drcelikbilek@yahoo.com)
© 2011, Hepatobiliary Pancreat Dis Int. All rights reserved.
杂志排行

Hepatobiliary & Pancreatic Diseases International的其它文章
- Expression oflamino acid transport system 1 and analysis of iodine-123-methyltyrosine tumor uptake in a pancreatic xenotransplantation model using fused high-resolution-micro-SPECT-MRI
- Laparoscopic liver resection for benign and malignant liver tumors
- Monday blues of deceased-donor liver transplantation
- Hepatobiliary & Pancreatic Diseases International (HBPD INT)
- Roles of sulfonylurea receptor 1 and multidrug resistance protein 1 in modulating insulin secretion in human insulinoma
- Atypical focal nodular hyperplasia of the liver