Psychology of Sport Injury:A Holistic Approach to Rehabilitating the Injured Athlete
2010-05-12JordanHamsonUtleyPhDLATATC
J.Jordan Hamson-Utley,PhD,LAT,ATC
Weber State University,Ogden,UT
Sports medicine practitioners mustconsider both physical and mental aspects of injury to fully rehabilitate the injured athlete.The psychological distress that follows injury has been well documented and calls for a change in the rehabilitation of injured athletes[1-3].With the recent emergence of sport psychology and the emphasis on competitive sport in the United States and beyond,psychological skills are no longer solely utilized by the elite athlete;college and high school athletes are gaining instruction on the use of psychological skills from sport psychologists,coaches,and fellow teammates.Psychological skills have been shown to be effective in improving positive outlook,reducing pain,improving relaxation,increasing adherence,reducing recovery time,and increasing overall satisfaction with rehabilitation,which make them invaluable tools for those who lead the rehabilitation of injured athletes[1,4-6].
During an athlete’s lifespan,undoubtedly they will become injured and drawn away from their team,their comfortzone,and from whatthey loveto do most.Sport-injury places both a physical and mental challenge on the athlete,however,the mental challenge is one that many athletes cannot manage alone.The athlete can attend physical therapy/rehabilitation to heal the physical injury,however the mental side of the injury often causes a struggle for which they are provided minimal to no care.Sports medicine practitioners(e.g.,athletic trainers,physical therapists)are experts in injury prevention,assessment,treatment and rehabilitation,however all too often,the practitioner’s focus is solely physical.What’s promising for the injured athlete,the current trend in rehabilitation is a holistic plan,encompassing both physical and mental exercises that prepare the athlete to return to play.Research supports the holistic approach citing the need for social support during recovery as a key to success[7,8].
Being removed from sport and having their personal athletic identity challenged,athletesmay turn to psychosocial support networks to deal with the negative side effects that have become reality.The integrated model of response to sport injury,a cognitive appraisal model by Wiese-Bjornstal and colleagues[9]highlights the psychological impact of injury by outlining pre-injury factors,personal factors,and situational factors that all affect how the athlete responds to the injury situation.The model is of theoretical importance because it highlights the role of the practitioner in the post-injury psychological healing process.
Paying attention to the pre-injury factors is important for the sports medicine practitioner as they assess the psychological needs of the athlete.Pre-injury factors include the athlete’s personality,history of stressors,coping resources,and prior use of psychological interventions.The athlete is likely to respond differently to the first ACL tear,compared to the second or third,because they know what to expect(e.g.,amount of pain,time spent in rehabilitation,typical setbacks).They also gather coping resources from prior injury experiences and begin to“know what works best”for them in certain setback situations.Prior use of psychological interventions is key when implementing these tools within the athlete’s rehabilitation program;a technique will likely be successful if used prior to rehabilitation.Finally,personality of the athlete is important to consider when managing motivation during a long rehabilitation program.If an athlete is intrinsically motivated(self-motivated),they may need less from the practitioner compared to an athlete who is extrinsically motivated(other-motivated);motivational techniques,both verbal and nonverbal,can be implemented by the athletic trainer or physical therapist to ensure the athlete gets the most out of the rehabilitation process[10].
Personal factors outlined in the model center on injury factors and individual differences.Of the personal factors,pain tolerance is important due to its correlation with rehabilitation adherence;researchers have theorized that a low pain tolerance correlates with non-adherent behavior,which in turn is related to a slower recovery[9].In addition to personal factors,situational factors also help the sports medicine practitioner understand how the athlete will process the injury process.Research on type of sport,level of competition,playing/scholarship status,and time in season suggests that these factors may play a role in how the athlete responds to injury.Furthermore,teammate,coach,and family dynamics are important social support provisions;the role of the sports medicine team as social support providers should not be underestimated due to time spent with the injured athlete.Practitioners are often the main source of such support and need to know how to offer this assistance to the athlete in need.
Recent research on athletes’expectations about athletic training practitioners found that that athlete’s expect athletic trainers to provide social support following injury(unpublished data).Being a good listener is the most valuable tool in providing effective social support to the injured athlete.Often,sports medicine practitioners find that they do not have time to be a quality member of the support network;if the support in rehabilitation is limited,the athlete may need to be referred to a mental health practitioner who can be an effective listening/support agent.In addition to being there for the athlete,the sports medicine practitioner can also provide education on the injury and rehabilitation process as another highly effective counseling tool.Providing education about the injury can lessen the athlete’s anxiety about the injury and rehabilitation process.Stress and anxiety have been linked to negative rehabilitation outcomes such as slower recovery times,non-adherence,and non-compliance[11-14].Other factors that can limit the progress of rehabilitation include an inconvenient location of rehabilitation services and a negative rehabilitation environment[9].These final two factors emphasize again,the role of the practitioner in the success of the rehabilitation;a positive environment with education,encouragement,and motivation to persist through pain,combined with convenient location and suitable scheduling of appointments,can optimize the recovery process.
To summarize thus far,the integrated model of response to sport-injury points to the sports medicine practitioner as an influential component of the athlete’s recovery.Practitioners can help to ensure a timely recovery by providing social support,education regarding sport-injury and the anticipated healing process,and a positive environment that encourages and motivates the athlete to face the many challenges of recovery and return to sport.Additionally,the practitioner can create and employ various psychological skills(e.g.,mental imagery,relaxation,goal setting,self-talk)with the athlete in attempt to address the current trend of holistic rehabilitation.
Presently,many sports medicine practitioners fail to use such techniques with their injured athletes.Although educated on the effectivenessand implementation of psychological skills with injured athletes,athletic trainers who work closely with the injured athletes report low levels of implementation(unpublished data);both preparation and confidence have been cited as reasons for nonuse.Additionally,attitudes about effectiveness can limit the use of aforementioned skills with injured athletes,however,attitudeshave grown positive over the past decade[8,15],as research in the field has documented the effectiveness of various psychological skills to improve the overall recovery process of the injured athlete[5].
The education of athletic training students,guided by the Commission on Accreditation of Athletic Training Education(CAATE),requires instruction on the Psychosocial Intervention and Referral content area.This area includes recognition,treatment and referral of various psychosocial disorders or struggles that athletes commonly face following injury and through out the season.Specifically,as this article focuses on the implementation of psychological skills to aid the athlete in recovery from injury,skills included in the education of athletic training students are mental imagery,relaxation,goal setting,motivation,self-talk/cognitive restructuring,systematic desensitization,and pain management/disassociation[16].This requirementundoubtedly suggestsa holistic approach to healing the injured athlete.The education ofphysical therapy students does not yet include such detailed training on the creation and implementation of psychological skills based on the athlete’s need for such care.
Psychologicalskills thatare mosteffective for use with the injured athlete:What,When,How,and Why
Defining the Phases of Injury Rehabilitation[17]
The first phase of rehabilitation is the initial injury phase.This phase is accompanied by the physical symptoms of swelling,muscle spasm,pain,and lack of mobility.Psychologically,the athlete may be experiencing anxiety and excessive worry about the uncertainty of the future.They may also experience grief due to the injury(perceived as a loss) and potentially anger if the injury was caused by an identifiable outside agent.As a result,the athlete will likely have a negative mind-set.A low self-esteem may also surface during this stage correlated with the strength of the athletic identity of the injured athlete.
The second phase of rehabilitation is the strengthening phase,which is physiologically characterized by a return of mobility and a reduction of swelling,allowing for strengthening to begin.The athlete is likely to continue to struggle with time spent away from sport and may have difficulty staying motivated to attend rehabilitation f it is painful,lacking results (due to experiencing setbacks),or long in terms of injury recovery.
The final phase of rehabilitation is return to sport.This phase begins when the athlete has near-normal(90%or better)function and strength in the injured joint.Psyhologically,the athlete faces the challenge of returning o a stage on which they were invincible and performed lawlessly prior to injury.Self-confidence,in the self and n the rehabilitated joint,is the main psychological issue n thisstage.Building and maintaining self-confidence an be achieved through the use of various psychological kills outlined below.
Mental Imagery(seeing is believing)
Imagery is defined as creating an image in the mind by retrieving memories of past events;successful imagery uses the five senses[18].Athletes can use imagery to aid n the rehabilitation from sport-injury by focusing on positive,pain-free,successfulsport-performance images,or by focusing on healing,relaxing images.Imagery is best used in the first stages of rehabilitation to foster a positive mind-set,to control pain,and to promote healng.When injured,the athlete may benefit from using magery to guide the healing process as it occurs within he body.This is commonly termed “healing imagery”nd has been shown to speed up the recovery process n injured athletes[19].Healing imagery guides the injured thlete to“see”healing occurring in the injured joint(e.g.,seeing the bloodstream bring healing to the injury site nd carrying away damaged cells thereby reducing welling,and repairing the damaged area) and to“feel”issues getting stronger(e.g.,visualizing ligaments feeling s strong as steel,or as many fibers linking together).Healing imagery may also be effective due to the relaxtion component that often accompanies the use of imgery techniques[17].
Imagery can be used during the strengthening phase of rehabilitation to motivate and to master rehabilitation xercises.In the final stages of rehabilitation and return o sport,imagery can be used to improve confidence in he rehabilitated body part, self-esteem, and overall elf-confidence. Performance imagery, where by nstructing the athlete to recallimagesofwhen they xperienced success in their sport, has three main psychological functions:(1) motivational to keep working hard at rehabilitation, (2) self-confidence building,and 3) remaining engaged through skill and strategy ehearsal while away from their sport.If an athlete is not confident about returning to sport,or has fears of e-injury,the athlete is likely to be re-injured.A sample of a healing imagery script for use in the early stages of rehabilitation is given in Table 1;images may need to be provided to the athlete of their body part and the healing/rebuilding process to optimize this technique.A sample healing imagery script for a knee can be found on iTunes at:http://itunes.apple.com/WebObjects/MZStore.woa/wa/viewPodcast?i=62448746&id=337761098.
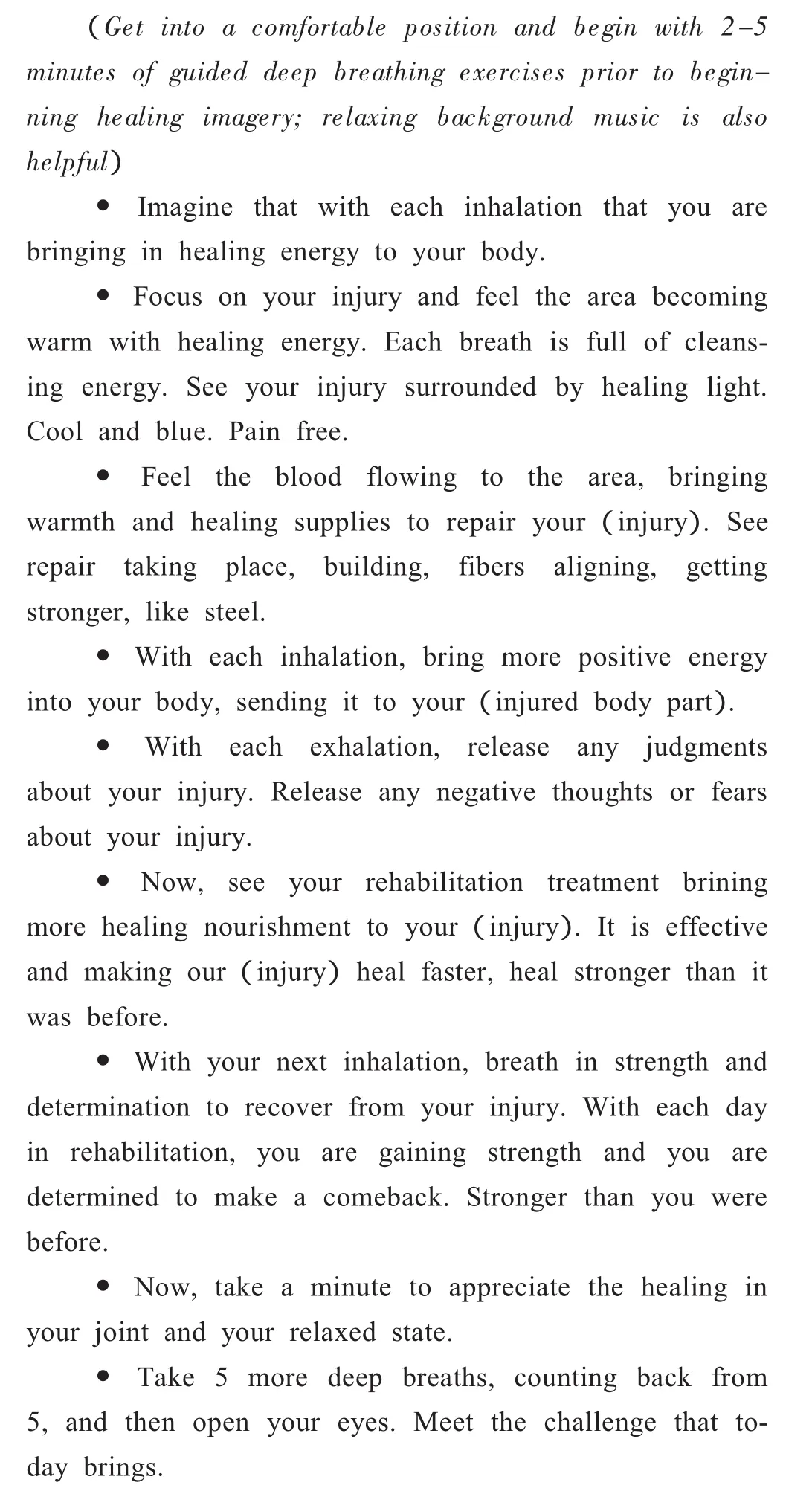
Table 1 Healing Mental Imagery Script(15 minutes)
Relaxation(maintaining a restful,healing state)
When the athlete becomes injured,blood flow increases to the joint or injured area resulting in swelling,pain,and various levels of immobility.Pain that follows injury is somewhat produced by muscle spasms,which is evidence of the body’s attemptto protectthe injured area from further damage.Relaxation can alter the post-injury response by buffering the physical changes(e.g.,reducing muscle spasm)at the injury site.Relaxation imagery(e.g.,imaging a pleasant scene such as a waterfall,a soothing stream,or a sunset)promotes physical relaxation of the musculature surrounding the injured joint,allowing for blood flow to return to normal and encouraging healing and rebuilding in the area.Relaxation can be helpful in the face of physiological and psychological stress and has been shown to aid in reducing pain associated with injury and injury rehabilitation[1,4].By implementing a relaxation imagery script,the practitioner can promote healing by lessening the stress response to injury and rehabilitation.Recent research shows that utilizing a 15-minute relaxation script reduces saliva cortisol levels(associated with the stress response) in healthy,college-aged athletes(unpublished data).Use of such scripts by the athlete prior to injury will likely hasten the relaxation effect,resulting in a more immediate relaxation response.Within rehabilitation,a script can be implemented prior to the therapy session to lessen anxiety,or following the therapy session during cryotherapy treatment.A sample relaxation script(in Japanese) can be found at:http://itunes.apple.com/WebObjects/MZStore.woa/waview-Podcast?i=62423500&id=337761098;the author suggests that it be individualized with audio and/or visuals chosen by the athlete to optimizeResults.
Goal Setting(keeping your eye on the prize)
Athletes have a history of being driven by performance goals.This goal-directed behavior can easily be transferred to the rehabilitation setting.In fact,this psychological skill is favored over other psychological skills by athletic trainers and physical therapists alike and is currently utilized in a majority,if not all,sport-injury rehabilitation programs[8].Research on the use of this psychological skill shows that to be most effective,the athlete and the practitioner should set the goals for rehabilitation together;involving the athlete increases the level of investment and motivation to reach set goals[10,19].To facilitate goal setting with athletes,it may be best to work backward from a long-term goal(outcome goal),as the returning to sport is the light at the end of the tunnel.Then,set a series of mid-range goals,which should be supported by daily rehabilitation goals;both of these goal types are short-term and serve to guide behavior toward the outcome goal.Goals provide feedback to the athlete and can motivate them to adhere to the rehabilitation program.
Positive Self-talk(staying on track)
Simply stated,we are who we think we are.What an athlete“says to themselves”in their head,commonly referred to as self-talk,is crucial to the progress of recovery.Negative thoughts,such as “I can’t do this”when faced with a difficult or painful rehabilitation exercise,can only have a negative impact on healing[19].On the other hand,coaching the athlete to change the negative self-talk into positive self-talk,through a technique called“thought stopping”[20],can be highly useful and ultimately promote healing and shorten recovery time[21].To do this,first the athlete needs to identify the challenging situation that is causing the negative self-talk.Then,the nextstep is to documentword-for-word the negative self-talk that is being used when the challenge occurs.Next,have the athlete formulate words or phrases that are positive and empower the athlete to beat the challenge.Last,the athlete must practice,practice,practice,just like learning any new physical skill.When the challenge arises,the athlete should close their eyes and envision a red stop sign(this reminds the athlete to stop prior to saying something negative);then,insert the pre-identified positive phrase as a response to the challenge.For example,when the athlete experiences pain on a single leg squat,they could say to themselves,“I can do this,the pain is not harming me”.The use of positive self-talk has been shown to improve sport performance and can be easily transferred to the rehabilitation domain[22].
Conclusion s&Future Directions
The current trend in sport-injury rehabilitation calls fora holistic approach,integrating both physicaland mental skills into the recovery plan of the athlete.This movement underscores the mind-body connection and focuses on the role of the sports medicine practitioner to emphasize the inclusion of such techniques that address healing the mental side of the injury.Today,many athletes bring prior experience using psychological skills into the rehabilitation setting,thus,the transfer of these skills can be effortless and straightforward.
Using the integrated model of response to sport injury serves to guide the sports medicine practitioner to recognize at risk athletes and employ useful coping techniques in the rehabilitation plan.Additionally,identifying existing resources,such as the iTunes tracks,will lessen the practitioner’s time involved in using such techniques with injured athletes.A generic relaxation scriptisa good place to start and can be downloaded from the Internet;the individualized approach is suggested as more effective,however,exposing the athlete to psychological skills is the main focus.
The National Athletic Trainers’ Association(NATA)annual symposium is a venue to gain post-certification training on the creation and implementation of psychological skills.Workshops that train practitioners on the use of psychological skills at various points in the athlete’s rehabilitation are most useful.Continued research validating effectiveness of psychological techniques,through not only subjective measures butObjectivemarkers,is desired to provide strength to claims of effectiveness and encourage practitioners to implement such techniques with injured athletes.Finally,the goal and responsibility of the sports medicine practitioner is to return the athlete to the field ofplay when they are physically and mentally ready.
Bibliography
[1]Evans L,Hare R,Mullen R.Imagery use during rehabilitation from injury.J Imagery Res Sport Phys Activ.2006;1(1):1-19.
[2]Monsma E,Mensch J,Farroll J.Keeping you head in the game:Sport-specific imagery and anxiety among injured athletes.J Athl Train.2009;44(4):410-417.
[3]Rotella R,Hedgpeth E,Pickens M.The psychology of injury and rehabilitation.In:Perrin D,ed.The Injured Athlete.Philadelphia,PA:Lippincott-Raven;1999:175-186.
[4]Driediger M,Hall C,Callow N.Imagery use by injured athletes:a qualitative analysis.J Sports Sci.2006;24(3):261-71.
[5]Hamson J.The Effects of Mental Imagery on Recovery Time and Adherence to Sport-injury Rehabilitation Programs of College Athletes.American Alliance for Health,Physical Education,Recreation and Dance,Salt Lake City,Utah;April 2006.
[6]Sordoni C,Hall C,Forwell L.The use of imagery by athletes during injury rehabilitation.J Sport Rehabil.2000;9:329-38.
[7]Udry E.Coping and social support among injured athletes following surgery.J Sport Exerc Psychol.1997;19:71-90.
[8]Hamson-Utley JJ,Martin S,Walters J. (2008).Athletic Trainers’and Physical Therapists’perceptions of the effectiveness of psychological skills within sport-injury rehabilitation programs.J Athl Train.43(3):258-264.
[9]Wiese-Bjornstal D,Smith A,Shaffer S,Morrey M.An integrated model of response to sport injury.J Appl Sport Psychol.1998;10:46-70.
[10]Hamson-Utley JJ,Vazquez L.The Comeback:Rehabilitating the Psychological Injury.Athl Thera Today.2008;13(5):35-38.
[11]Anderson M,Williams J.A model of stress and athletic injury:Prediction and prevention.In:Smith D,Bar-Eli M,eds.Essential readings in sport and exercise psychology.New York,NY:Human Kinetics;2007:325-327.
[12]Cupal D.Psychological interventions in sport injury prevention and rehabilitation.J Appl Sport Psychol.1998;10:103-123.
[13]Daly J,Brewer B,Van Raalte J,Petitpas A,Sklar J.Cognitive appraisal,emotional adjustment,and adherence to rehabilitation following knee surgery.J Sport Rehabil.1995;4:23-30.
[14]Loundagin C,Fisher L.The relationship between mental skills and enhanced athletic injury rehabilitation.Poster presented at the Annual Meeting of the Association of Applied Sport Psychology and the Canadian Society for Psychomotorlearning and SportPsychology,Montreal,Canada;1993.
[15]Wiese D,Weiss M,Yukelson D.Sport psychology in the training room:A survey of athletic trainers.Sport Psychol.1991;5:15-21.
[16]National Athletic Trainers'Association.Athletic Training Educational Competencies.4th ed.Dallas,Texas:National Athletic Trainers'Association;2006:35-36.
[17]Hamson JJ.Using mental imagery to improve the return from sport injury.Podium Sports J. [serial online].April 2007. Available at: http://www.podiumsportsjournal.com/using-mental-imagery-to-improve-the-return-from-sport-injury/.Accessed December 1,2009.
[18]Vealey RS,Greenleaf CA.Seeing is believing:Understanding and using imagery in sport.In:Williams JM,ed.Applied Sport Psychology:Personal growth to peak performance.5thed.Boston,MA:McGraw-Hill;2001:284-311.
[19]Ievleva L,Orlick T.Mental links to enhanced healing:an exploratory study.Sport Psychol.1991;5:25-40.
[20]Zinsser N,Bunker L,Williams JM.Cognitive techniques for building confidence and enhancing performance.In:Williams JM,ed.Applied SportPsychology:Personal growth to peak performance.4thed.Mountain View,CA:Mayfield;2001:284-311.
[21]Heil J.Psychology of Sport Injury.Champaign,IL:Human Kinetics;1993.
[22]Scherzer C,Brewer B,Cornelius A,Van Raalte J,Peitipas A,Sklar J,et al.Psychological skills and adherence to rehabilitation after reconstruction of the anterior cruciate ligament.J Sport Rehabil.2001;10:165-172.
