风险评估模型预测人工肝治疗肝衰竭患者发生静脉血栓栓塞症的价值分析
2023-04-29陆素芳黄睿赵红利王丹丹丁玉珍周红
陆素芳 黄睿 赵红利 王丹丹 丁玉珍 周红

摘要:目的 探讨风险评估模型对人工肝治疗肝衰竭患者静脉血栓栓塞症(VTE)发生风险的预测价值。方法 回顾性选取2018年3月—2021年12月于南京大学医学院附属鼓楼医院行人工肝治疗的肝衰竭患者184例,其中并发VTE组患者41例,未并发VTE患者(对照组)143例。比较两组患者临床资料,并采用Caprini风险评估模型对两组患者进行评分及风险分级。计量资料两组间比较采用t检验;计数资料两组间比较采用χ2检验;等級资料两组间比较采用Mann-Whitney U秩和检验。采用Logistic回归分析人工肝治疗肝衰竭患者发生VTE的独立危险因素。采用受试者工作特征曲线(ROC曲线)分析Caprini量表评分、多因素预测模型及二者联合对VTE的预测价值。结果 并发VTE组患者Caprini量表评分为(4.39±1.10)分,明显高于对照组(3.12±1.04)分(t=6.805, P<0.001)。两组患者Caprini量表危险度分级存在明显差异(Z=-4.872, P<0.001),并发VTE的患者中,高危、极高危组占比更高。单因素分析结果显示,并发VTE组与对照组患者在年龄(t=6.400,P<0.001)、置管方式(χ2=14.413,P<0.001)、人工肝治疗次数(Z=-4.720,P<0.001)、活动情况(Z=-6.282,P<0.001)、合并感染(χ2=33.071,P<0.001)、D-二聚体(t=8.746,P<0.001)、28 d死亡率(χ2=5.524,P=0.022)比较差异均有统计学意义。多因素分析结果显示,人工肝治疗次数(X1)(OR=0.251, 95%CI: 0.111~0.566, P=0.001)、活动情况(X2)(OR=0.122, 95%CI: 0.056~0.264, P<0.001)、D-二聚体(X3)(OR=2.921, 95%CI: 1.114~7.662, P=0.029)为影响肝衰竭人工肝治疗患者VTE发生的独立危险因素。个体预测概率方程为P=1/[1+e-(7.425-1.384X1-2.103X2+1.072X3)]。ROC曲线分析结果显示,Caprini评分曲线下面积为0.802(95%CI: 0.721~0.882, P<0.001),多因素模型曲线下面积为0.768(95%CI: 0.685~0.851, P<0.001),二者联合运用曲线下面积为0.957(95%CI: 0.930~0.984, P<0.001)。结论 Caprini风险评估模型对人工肝治疗肝衰竭患者VTE发生风险具有较高的预测效能,联合多因素预测模型后可更为显著地提高对VTE的预测价值。
关键词:肝功能衰竭; 静脉血栓栓塞; 肝, 人工; 危险因素; 模型, 统计学
基金项目:国家自然科学基金青年基金项目(81702011); 南京大学现代医院管理与发展研究所课题项目&南京鼓楼医院医学发展医疗救助基金(NDYG2021016)
Value of a risk assessment model in predicting venous thromboembolism in patients with liver failure after artificial liver support therapy
LU Sufang, HUANG Rui, ZHAO Hongli, WANG Dandan, DING Yuzhen, ZHOU Hong. (Department of Infectious Diseases, Affiliated Drum Tower Hospital of Nanjing University Medical School, Nanjing 210008, China)
Corresponding author:
LU Sufang, sufanglu0708@126.com (ORCID:0000-0001-5471-2511)
Abstract:
Objective To investigate the value of a risk assessment model in predicting venous thromboembolism (VTE) in patients with liver failure after artificial liver support therapy. Methods A retrospective analysis was performed for the clinical data of 124 patients with liver failure who received artificial liver support therapy in Affiliated Drum Tower Hospital of Nanjing University Medical School from March 2019 to December 2021, among whom there were 41 patients with VTE (observation group) and 143 patients without VTE (control group). Related clinical data were compared between the two groups, and the Caprini risk assessment model was used for scoring and risk classification of the patients in both groups. The t-test was used for comparison of continuous data between two groups; the chi-square test was used for comparison of categorical data between two groups; the Mann-Whitney U rank sum test was used for comparison of ranked data between two groups. The logistic regression analysis was used to investigate the independent risk factors for VTE in patients with liver failure after artificial liver support therapy. The receiver operating characteristic (ROC) curve was used to investigate the value of Caprini score and the multivariate predictive model used alone or in combination in predicting VTE. Results The observation group had a significantly higher Caprini score than the control group (4.39±1.10 vs 3.12±1.04, t=6.805, P<0.001). There was a significant difference between the two groups in risk classification based on Caprini scale (P<0.05), and the patients with high risk or extremely high risk accounted for a higher proportion among the patients with VTE. The univariate analysis showed that there were significant differences between the two groups in age (t=6.400, P<0.001), catheterization method (χ2=14.413, P<0.001), number of times of artificial liver support therapy (Z=-4.720, P<0.001), activity (Z=-6.282, P<0.001), infection (χ2=33.071, P<0.001), D-dimer (t=8.746, P<0.001), 28-day mortality rate (χ2=5.524, P=0.022). The multivariate analysis showed that number of times of artificial liver support therapy (X1) (odds ratio [OR]=0.251, 95% confidence interval [CI]: 0.111-0.566, P=0.001), activity (X2) (OR=0.122, 95%CI: 0.056-0.264, P<0.001), D-dimer (X3) (OR=2.921, 95%CI: 1.114-7.662, P=0.029) were independent risk factors for VTE in patients with liver failure after artificial liver support therapy. The equation for individual predicted probability was P=1/[1+e-(7.425-1.384X1-2.103X2+1.072X3)]. The ROC curve analysis showed that Caprini score had an area under the ROC curve of 0.802 (95%CI: 0.721-0.882, P<0.001), and the multivariate model had an area under the ROC curve of 0.768 (95%CI: 0.685-0.851, P<0.001), while the combination of Caprini score and the multivariate model had an area under the ROC curve of 0.957 (95%CI: 0.930-0.984, P<0.001). Conclusion The Caprini risk assessment model has a high predictive efficiency for the risk of VTE in patients with liver failure after artificial liver support therapy, and its combination with the multivariate predictive model can significantly improve the prediction of VTE.
Key words:
Liver Failure; Venous Thromboembolism; Liver, Artificial; Risk Factors; Models, Statistical
Research funding:
National Natural Science Foundation of China (81702011); Research Project of Modern Hospital Management and Development Institute of Nanjing University and Medical Development and Medical Assistance Fund of Nanjing Drum Tower Hospital (NDYG2021016)
静脉血栓栓塞症(venous thromboembolism,VTE)是指在静脉管腔内血液出现不正常的凝结,导致静脉血管完全或不完全阻塞,从而引发静脉回流障碍的一种血液循环系统疾病[1]。VTE的主要表现包括下肢神静脉血栓和肺栓塞,是医院住院重症患者常见并发症之一,严重威胁患者的生存预后[2]。肝衰竭是一种临床常见的严重肝病症候群,病死率极高[3],人工肝支持系统是目前最为有效的治疗手段之一,但是由于人工肝支持系统需要行深静脉插管,插管留置时间较长,且肝衰竭患者由于基础疾病的凝血功能障碍,常发生感染、出血以及VTE等多种并发症[4]。因此,及时应用科学有效的风险评估工具,对人工肝支持治疗肝衰竭患者危险因素进行风险评估并实施有效的预防措施,对预防VTE的发生以及改善患者临床预后具有重要价值[5]。本研究旨在探讨分析风险评估模型对接受人工肝治疗的肝衰竭患者发生VTE的预测价值。
1 资料与方法
1.1 研究对象 回顾性选取2018年3月—2021年12月于本院接受人工肝治疗的肝衰竭患者。纳入标准:(1)符合《肝衰竭诊治指南(2012年版)》[6]中关于肝衰竭的诊断标准;(2)患者均接受人工肝治疗;(3)VTE患者采用静脉彩超/静脉造影进行确诊;(4)患者临床资料完整;(5)年龄≥18岁。排除标准:(1)临床资料不完整者;(2)合并严重活动性出血或弥散性血管内凝血患者;(3)合并循环功能衰竭患者;(4)在人工肝治疗期间发生血浆、鱼精蛋白、肝素等血制品或药物高度过敏患者;(5)妊娠期患者。根据是否并發VTE将所有患者分为并发VTE组和对照组。
1.2 研究方法
1.2.1 临床资料 收集患者一般资料,包括年龄、文化程度、BMI、空腹血糖、吸烟情况、置管方式、置管有无使用肝素、促凝治疗、人工肝治疗次数、肝衰竭病因、合并感染、肝性脑病、TBil、ALT、D-二聚体、纤维蛋白原、28 d病死率。
1.2.2 血栓风险评估 采用2013版Caprini评分对本研究纳入患者进行评分。根据Caprini风险模型,将每项风险因素对VTE的影响进行加权赋值,按照总分将患者分为4个风险层级。低危组(0~1分):血栓发生风险<10%;中危组(2分):血栓发生风险10%~20%;高危组(3~4分):血栓发生风险20%~40%;极高危组(≥5分):血栓发生风险40%~80%。
1.3 统计学方法 采用SPSS 25.0进行统计学数据分析。计量资料以x±s表示,两组间比较采用t检验;计数资料两组间比较采用χ2检验;等级资料两组间比较采用Mann-Whitney U秩和检验。采用Logistic回归分析人工肝治疗肝衰竭患者发生VTE的独立危险因素。采用受试者工作特征曲线(ROC曲线)分析Caprini量表评分、多因素预测模型及二者联合对VTE的预测价值。P<0.05为差异具有统计学意义。
2 结果
2.1 一般资料 共纳入接受人工肝治疗的肝衰竭患者184例,其中并发VTE组患者41例,未并发VTE的对照组患者143例。
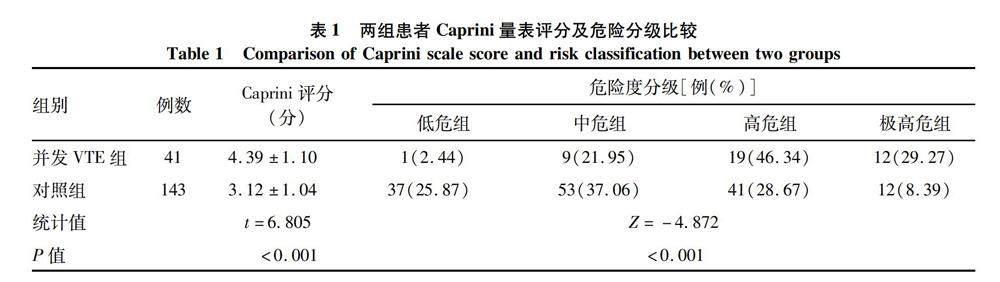
2.2 两组患者Caprini量表评分及危险分级比较 并发VTE组患者Caprini量表评分为(4.39±1.10)分,明显高于对照组[(3.12±1.04)分](t=6.805, P<0.001)。两组患者Caprini量表危险度分级存在明显差异(Z=-4.872, P<0.001),并发VTE的患者中,高危、极高危组占比更高(表1)。
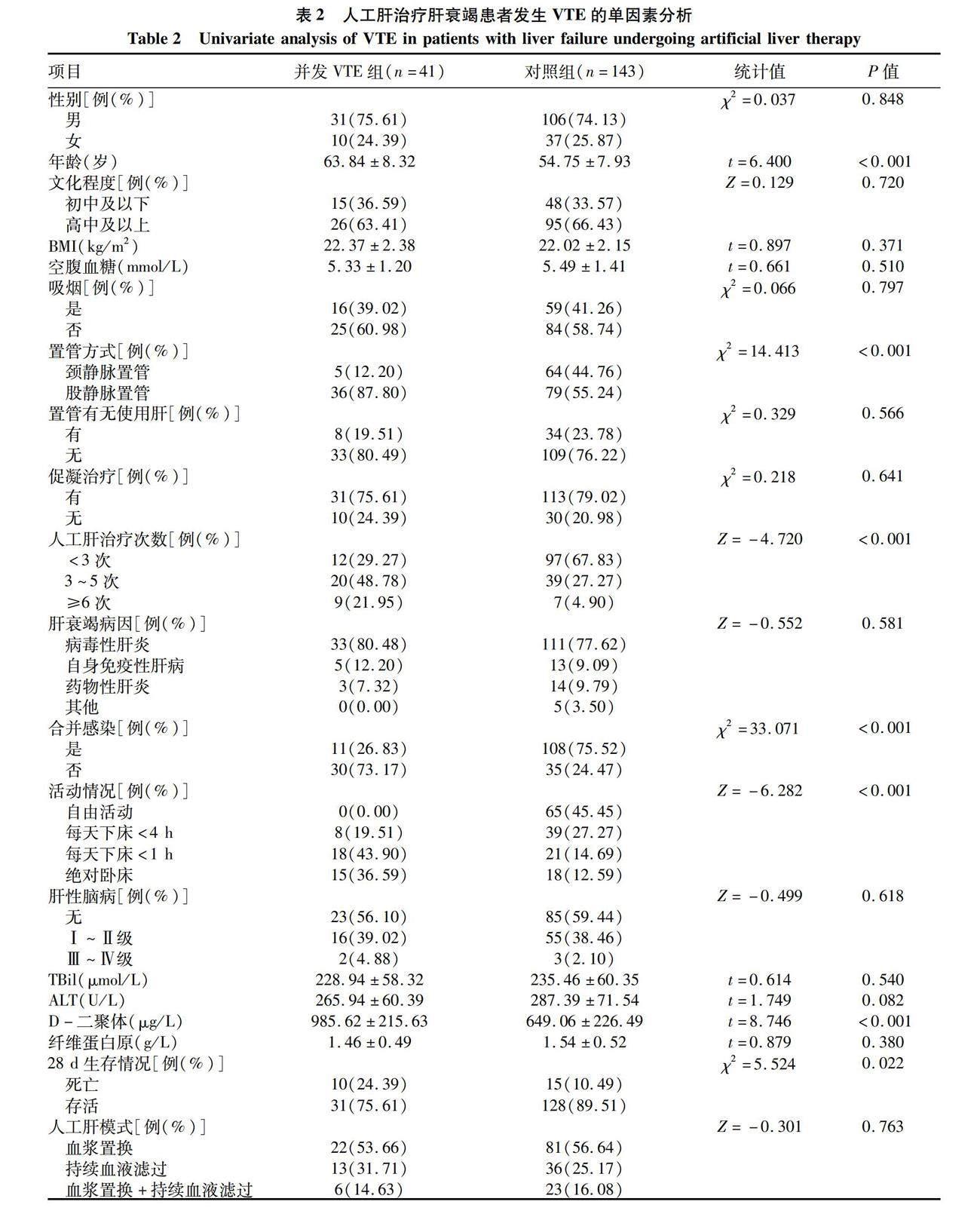
2.3 人工肝治疗肝衰竭患者发生VTE的单因素分析单因素分析结果显示,并发VTE组与对照组患者在年龄(t=6.400,P<0.001)、置管方式(χ2=14.413,P<0.001)、人工肝治疗次数(Z=-4.720,P<0.001)、活动情况(Z=-6.282,P<0.001)、合并感染(χ2=33.071,P<0.001)、D-二聚体(t=8.746,P<0.001)、28 d病死率(χ2=5.524,P=0.022)比较差异均有统计学意义(表2)。
2.4 人工肝治疗肝衰竭患者发生VTE的多因素分析多因素分析结果显示,人工肝治疗次数(X1)(OR=0.251, 95%CI: 0.111~0.566, P=0.001)、活动情况(X2)(OR=0.122, 95%CI: 0.056~0.264, P<0.001)、D-二聚体(X3)(OR=2.921, 95%CI: 1.114~7.662, P=0.029)为影响肝衰竭人工肝治疗患者VTE发生的独立危险因素(表3)。由回归结果获得logit(P)=7.425-1.384X1-2.103X2+1.072X3,个体预测概率方程为P=1/[1+e-(7.425-1.384X1-2.103X2+1.072X3)]。
2.5 Caprini量表评分、多因素预测模型及二者联合对VTE的预测价值 ROC曲线分析结果显示,Caprini评分曲线下面积为0.802(95%CI: 0.721~0.882, P<0.001),多因素模型曲线下面积为0.768(95%CI: 0.685~0.851, P<0.001),二者联合运用曲线下面积为0.957(95%CI: 0.930~0.984, P<0.001)(图1)。
3 讨论
人工肝支持系统是治疗肝衰竭的重要治疗方式,其治疗机制是基于肝细胞强大的再生能力,通过机械、理化以及生物性体外装置,帮助清除肝衰竭患者机体内各种有害物质,同时补充机体必需物质,进而改善机体内环境[7-8]。采用人工肝支持系统可暂时替代衰竭肝脏的部分功能,从而为肝细胞再生以及肝脏功能的恢复创造有利的条件[9-10]。
VTE是一种临床常见并发症,但是由于患者缺乏特性的临床症状,临床漏诊率较高,治疗效果不理想,复发率较高且患者临床预后差[11]。由于肝衰竭患者肝脏合成凝血因子减少、脾功能亢进以及纤溶功能亢进,导致机体血小板减少,因此肝衰竭患者一般被认为处于低凝状态[12-13]。降低VTE发生率的关键在于对VTE的早期识别,并及时给予有效的干预[14]。因此,亟需一种准确、简便、有效的工具用于评估人工肝治疗肝衰竭VTE发生风险,对于改善患者临床预后具有重要价值。
Caprini量表评分被应用于多种疾病领域,且被认为其具有良好的信效度[15-16]。美国胸科协会指南[16]建议使用Caprini量表对患者进行血栓评估以及风险分级,并针对不同的风险分层采取相应的预防措施。本研究采用Caprini风险评估模型进行评估分析,探讨其对人工肝治疗肝衰竭患者VTE预测价值。研究结果显示,并发VTE组患者Caprini量表评分显著高于对照组,且并发VTE的患者中,高危、极高危组占比更高。
Logistic回归分析结果显示,人工肝治疗次数、活动情况、D-二聚体是人工肝治疗肝衰竭患者发生VTE的独立危险因素,进入预测模型。年龄、置管方式、合并感染和28 d病死率两组间比较虽有统计学差异,但并未进入回归模型,考虑可能是由于相关样本量所限。本研究中,Caprini评分、多因素模型及二者联合对人工肝治疗肝衰竭患者发生VTE的预测价值与既往研究[17-18]结果相近。研究表明,Caprini风险评估模型对人工肝治疗肝衰竭患者VTE发生风险具有较高的预测效能,联合多因素预测模型后可更为显著地提高对VTE的预测价值。
伦理学声明:本研究方案于2018年2月10日经由南京大学医学院附属鼓楼医院伦理委员会审批,批号:2018022。
利益冲突声明:本研究不存在研究者、伦理委员会成员、受试者监护人以及与公开研究成果有关的利益冲突。
作者贡献声明:陆素芳、黄睿负责课题设计,资料分析,撰写论文;赵紅利、王丹丹参与收集数据,修改论文;丁玉珍、周红负责拟定写作思路,指导撰写文章并最后定稿。
参考文献:
[1]RAPP CM, SHIELDS EJ, WIATER BP, et al. Venous thromboembolism after shoulder arthoplasty and arthroscopy[J]. J Am Acad Orthop Surg, 2019, 27(8): 265-274. DOI: 10.5435/JAAOS-D-17-00763.
[2]WANG Q, DING J, YANG R. The venous thromboembolism prophylaxis in patients receiving thoracic surgery: A systematic review[J]. Asia Pac J Clin Oncol, 2021, 17(5): e142-e152. DOI: 10.1111/ajco.13386.
[3]SI N, LIU F, LIU L, et al. Effect of platelet level and platelet parameters on the prognosis of patients with acute-on-chronic liver failure[J]. J Clin Hepatol, 2022, 38(2): 381-386. DOI: 10.3969/j.issn.1001-5256.2022.02.023.
司诺, 刘芳, 刘磊, 等. PLT水平及PLT参数对慢加急性肝衰竭患者预后的影响[J]. 临床肝胆病杂志, 2022, 38(2): 381-386. DOI: 10.3969/j.issn.1001-5256.2022.02.023.
[4]ZHOU L, CHEN Y. Model selection and curative effect judgment criteria for artificial liver in the treatment of liver failure[J]. Chin J Hepatol, 2022, 30(2): 127-130. DOI: 10.3760/cma.j.cn501113-20220108-00008.
周莉, 陈煜. 人工肝治疗肝衰竭模式选择及其疗效判断标准[J]. 中华肝脏病杂志, 2022, 30(2): 127-130. DOI: 10.3760/cma.j.cn501113-20220108-00008.
[5]WANG L, XU WX, ZHU Z, et al. Influence of artificial liver support system therapy on platelet in treatment of hepatitis B virus-related acute-on-chronic liver failure[J]. J Clin Hepatol, 2022, 38(5): 1053-1058. DOI: 10.3969/j.issn.1001-5256.2022.05.015.
王璐, 许文雄, 朱姝, 等. 人工肝治疗HBV相关慢加急性肝衰竭的血小板计数变化及其影响因素[J]. 临床肝胆病杂志, 2022, 38(5): 1053-1058. DOI: 10.3969/j.issn.1001-5256.2022.05.015.
[6]Liver failure and artificial liver group of infectious diseases branch of Chinese Medical Association, severe liver disease and artificial liver group of Hepatology branch of Chinese Medical Association. Diagnostic and treatment guidelines for liver failure (2012 version)[J]. Chin J Clin Infect Dis, 2012, 5(6): 321-327. DOI: 10.3760/cma.j.issn.1674-2397.2012.06.001.
中华医学会感染病学分会肝衰竭与人工肝学组, 中华医学会肝病学分会重型肝病与人工肝学组. 肝衰竭诊治指南(2012年版)[J]. 中华临床感染病杂志, 2012, 5(6): 321-327. DOI: 10.3760/cma.j.issn.1674-2397.2012.06.001.
[7]WU B, DU LY, MA YJ, et al. Effects of different combinations of artificial liver support system on efficacy and inflammatory indexes of patients with hepatitis B virus-related acute-on-chronic liver failure in early and middle stages[J/CD]. Chin J Liver Dis (Electronic Version), 2021, 13(1): 32-38. DOI: 10.3969/j.issn.1674-7380.2021.01.006.
吳蓓, 杜凌遥, 马元吉, 等. 不同组合人工肝支持系统治疗乙型肝炎病毒相关早、中期慢加急性肝衰竭患者的疗效及对炎症指标的影响[J/CD]. 中国肝脏病杂志(电子版), 2021, 13(1): 32-38. DOI: 10.3969/j.issn.1674-7380.2021.01.006.
[8]NANCHAL R, SUBRAMANIAN R, KARVELLAS CJ, et al. Guidelines for the management of adult acute and acute-on-chronic liver failure in the ICU: Cardiovascular, endocrine, hematologic, pulmonary, and renal considerations[J]. Crit Care Med, 2020, 48(3): e173-e191. DOI: 10.1097/CCM.0000000000004192.
[9]MAP YQ, ZHOU XS, WANG X, et al. Study on the correlation between antithrombin Ⅲ activity and short-term prognosis of acute-on-chronic liver failure patients treated with artificial liver support system[J]. Chin Hepatol, 2021, 26(7): 770-775. DOI: 10.3969/j.issn.1008-1704.2021. 07.016.
毛燕群, 周学士, 王霞, 等. 抗凝血酶Ⅲ活性与慢加急性肝衰竭患者人工肝治疗结局的相关性[J]. 肝脏, 2021, 26(7): 770-775. DOI: 10.3969/j.issn.1008-1704.2021. 07.016.
[10]PENG H, XU FF, WAN XQ, et al. Clinical efficacy of artificial liver plasma exchange in treatment of patients with severe hepatitis and influencing factors for prognosis[J]. Clin Misdiagn Misther, 2021, 34(5): 90-95. DOI: 10.3969/j.issn.1002-3429.2021.05.018.
彭欢, 许菲菲, 万小秋, 等. 人工肝血浆置换治疗重型肝炎效果及其预后影响因素分析[J]. 临床误诊误治, 2021, 34(5): 90-95. DOI: 10.3969/j.issn.1002-3429.2021.05.018.
[11]WANG DG, TAN CL, WANG HY, et al. Predictive value of thromboelastogram for postoperative venous thromboembolism in breast cancer patients[J]. Chin J Curr Adv Gen Surg, 2022, 25(1): 23-26, 48. DOI: 10.3969/j.issn.1009-9905.2022.01.005.
王德光, 谭春玲, 王洪燕, 等. 血栓弹力图对乳腺癌术后静脉血栓栓塞症的预测价值[J]. 中国现代普通外科进展, 2022, 25(1): 23-26, 48. DOI: 10.3969/j.issn.1009-9905.2022.01.005.
[12]ZHANG L, HE JX, FAN XS, et al. Prognostic value of antithrombin Ⅲ activity combined with CLIF-C OFs score in patients with HBV related chronic plus acute liver failure[J]. Chin J Difficult Comp Cases, 2022, 21(1): 36-40, 45. DOI: 10.3969/j.issn.1671-6450. 2022.01.007.
张蕾, 贺建勋, 范雪松, 等. 抗凝血酶Ⅲ活性联合CLIF-C OFs评分对HBV相关慢加急性肝衰竭患者预后的评估价值[J]. 疑难病杂志, 2022, 21(1): 36-40, 45. DOI: 10.3969/j.issn.1671-6450. 2022.01.007.
[13]YANG P, XIAO LR, YANG N, et al. The evaluation value of procalcitonin and prothrombin activity in the prognosis of liver failure complicated by infection[J]. Chin J Nosocomiol, 2022, 32(4): 531-534. DOI: 10.11816/cn.ni.2022-210509.
楊平, 肖乐尧, 杨娜, 等. 降钙素原和凝血酶原活动度在肝衰竭合并感染预后中的评估价值[J]. 中华医院感染学杂志, 2022, 32(4): 531-534. DOI: 10.11816/cn.ni.2022-210509.
[14]WU XJ, ZHAO WL, SU ZZ, et al. Application value of antithrombin Ⅲ in evaluating the disease progression and 28-day mortality of patients with HBV-associated acute-on-chronic liver failure[J]. Chin J Clin Lab Sci, 2020, 38(6): 458-463. DOI: 10.13602/j.cnki.jcls.2020.06.18.
吴晓娟, 赵文玲, 苏真珍, 等. 抗凝血酶Ⅲ评价HBV感染相关慢加急性肝衰竭患者疾病进展和28天死亡率的应用价值[J]. 临床检验杂志, 2020, 38(6): 458-463. DOI: 10.13602/j.cnki.jcls.2020.06.18.
[15]LIN Y, ZENG Z, LIN R, et al. The Caprini thrombosis risk model predicts the risk of peripherally inserted central catheter-related upper extremity venous thrombosis in patients with cancer[J]. J Vasc Surg Venous Lymphat Disord, 2021, 9(5): 1151-1158. DOI: 10.1016/j.jvsv.2020.12.075.
[16]ZHOU J, WANG QY, QIN CL. Analysis of risk factors for venous thromboembolism after operation of primary liver cancer and application of Caprini risk prediction model[J]. Mod Oncol, 2022, 30(12): 2214-2218. DOI: 10.3969/j.issn.1672-4992. 2022. 12.021.
周建, 王庆元, 秦长岭. 原发性肝癌术后发生静脉血栓栓塞症的危险因素及Caprini风险预测模型的应用[J]. 现代肿瘤医学, 2022, 30(12): 2214-2218. DOI: 10.3969/j.issn.1672-4992.2022. 12.021.
[17]MENG R, MA CY. Practice and effect of Caprini risk assessment model in prevention of deep venous thrombosis in ICU patients[J]. Chin J Thromb Hemost, 2017, 23(6): 1054-1056. DOI: 10.3969/j.issn.1009-6213.2017.06.057.
孟蕊, 马春园. Caprini风险评估模型在预防ICU患者深静脉血栓中的实践效果[J]. 血栓与止血学, 2017, 23(6): 1054-1056. DOI: 10.3969/j.issn.1009-6213.2017.06.057.
[18]QIAO Y, GUO P, WANG L. Validityan alysis of Caprini thrombosis assessment scale in assessing the risk of venous thromboembolism in liver failure patients treated with artificial liver[J]. Acta Acad Med Bengbu, 2020, 45(1): 120-123. DOI: 10.13898/j.cnki.issn.1000-2200.2020.01.031.
乔艳, 郭普, 王丽. Caprini血栓风险评估量表预测人工肝治疗肝衰竭病人静脉血栓栓塞症风险有效性分析[J]. 蚌埠医学院学报, 2020, 45(1): 120-123. DOI: 10.13898/j.cnki.issn.1000-2200.2020.01.031.
收稿日期:
2022-08-01;录用日期:2022-10-11
本文编辑:邢翔宇
