原位肝移植术后胆道并发症发生的影响因素分析
2023-04-29朱明强杨大帅裴俊鹏熊祥云苏洋丁佑铭
朱明强 杨大帅 裴俊鹏 熊祥云 苏洋 丁佑铭
摘要:
目的 分析原位肝移植術后胆道并发症相关的血清学指标、手术指标,探究其影响因素及预测指标。方法 回顾性收集武汉大学人民医院2016年1月—2022年6月101例行原位肝移植患者的临床资料。根据患者术后6个月是否出现胆道并发症,分为胆道并发症组(BC组,n=21)和非胆道并发症组(非BC组,n=80)。计量资料两组间比较采用成组t检验或 Mann- Whitney U检验,计数资料两组间比较使用χ2检验。单因素与多因素分析采用Logistic回归分析,并以受试者工作特征曲线(ROC曲线) 评估联合指标的预测效能。结果 101例患者中21例(20.8%)发生胆道并发症。Logistc多因素分析结果显示,MELD评分(OR=0.134,95%CI:0.031~0.590,P=0.008)、全身炎症反应指数(SⅡ)/Alb(OR=1.415,95%CI:1.181~1.696,P=0.001)、输入血浆量(OR=1.001,95%CI:1.000~1.002,P=0.032)是肝移植患者术后发生胆道并发症的独立影响因素。MELD 评分、SⅡ/Alb、输入血浆量、MELD+SⅡ/Alb、MELD+SⅡ/Alb+输入血浆量预测肝移植术后胆道并发症的ROC曲线下面积(AUC)分别为 0.712、0.870、0.712、0.900、0.918。结论 SⅡ/Alb、输入血浆量及MELD评分是肝移植术后胆道并发症发生的影响因素,三者联合具有较好的预测价值和临床指导意义。
关键词:肝移植; 手术后并发症; 系统免疫炎症指数; MELD评分
基金项目:国家重点研发计划 (2022YFC2407304)
Analysis of influencing factors on biliary complications after orthotopic liver transplantation
ZHU Mingqiang, YANG Dashuai, PEI Junpeng, XIONG Xiangyun, SU Yang, DING Youming. (Department of Hepatobiliary Surgery, Renmin Hospital of Wuhan University, Wuhan 430060, China)
Corresponding author:
DING Youming, dingym62@163.com (ORCID:0000-0001-6695-3275)
Abstract:
Objective To analyze the serological markers and surgical indicators associated with biliary complications after orthotopic liver transplantation, explore their influencing factors and predictive indicators. Methods A retrospective analysis was performed for the clinical data of 101 patients who underwent orthotopic liver transplantation in Renmin Hospital of Wuhan University from January 2016 to June 2022, according to the presence or absence of biliary complication (BC) at 6 months after surgery, they were divided into BC group with 21 patients and non-BC group with 80 patients. The t-test or the Mann-Whitney U test was used for comparison of continuous data between groups, and the chi-square test was used for comparison of categorical data between groups. Univariate and multivariate Logistic regression analyses were performed, and the receiver operating characteristic (ROC) curve was used to evaluate the predictive performance of combined indicators. Results Among the 101 patients, 21 (20.8%) experienced BC. The multivariate Logistic regression analysis showed that MELD score(odds ratio [OR]=0.134, 95% confidence interval [CI]: 0.031-0.590, P=0.008), SⅡ/Alb (OR=1.415, 95%CI: 1.181-1.696, P=0.001), and plasma transfusion volume (OR=1.001, 95%CI: 1.000-1.002, P=0.032) were independent risk factors for the development of BC in patients after liver transplantation. MELD score, SⅡ/Alb, plasma transfusion volume, MELD+SⅡ/Alb, and MELD+SⅡ/Alb+plasma transfusion volume had an area under the ROC curve of 0.712, 0.870, 0.712, 0.900, and 0.918, respectively, in predicting BC after liver transplantation. ConclusionSⅡ/Alb, plasma transfusion volume and MELD score are independent risk fators for BC after liver transplantation. The combination of three indicators has good predictive value and clinical guiding significance for BC after liver transplantation.
Key words:Liver Transplantation; Postoperative Complications; Systemic Immune-Inflammation Index; MELD Score
Research funding:
National Key Research and Development Program(2022YFC2407304)
肝移植是终末期肝病最终的治疗手段,能有效地延长患者生存时间,术后5年的存活率可达80%[1-2]。胆道并发症是围手术期常见的并发症之一,发生率为5%~40%,是影响移植肝存活时间、受者生存质量的重要因素[3-4]。肝移植术后胆道并发症包括吻合口及非吻合口狭窄、胆漏、胆管结石和胆泥形成、Oddi 括约肌功能障碍、胆道出血等[5-6]。提升肝移植手术技巧、优化免疫抑制方案、改善围手术期管理水平,包括术前受者准备、术后并发症防治管理等是改善患者预后的重要因素[7]。本研究回顾性分析101例原位肝移植患者的临床资料,研究术后胆道并发症的发生情况及联合指标的诊断预测效能,用于临床对并发症的积极预防和肝移植患者围手术期的治疗。
1 资料与方法
1.1 研究对象 回顾性收集2016年1月—2022年6月本院肝胆外科行经典原位肝移植患者101例,其中男86例,女15例,年龄15~74岁,平均(50.2±10.4)岁。术后均采取他克莫司联合吗替麦考酚酯抗术后排斥。原发病包括:肝癌和/或肝硬化76例、急性肝衰竭8例、酒精性肝硬化8例、自身免疫性肝硬化3例、原发性胆汁性肝硬化3例、多囊肝2例、先天性胆道闭锁1例。全部肝脏来源于自愿无偿捐献者。根据患者术后6个月是否出现胆道并发症,分为胆道并发症组(BC组,n=21)和非胆道并发症组(非BC组,n=80)。
1.2 纳入与排除标准 肝移植术后胆道并发症80%在6个月内发生[8]。纳入标准:(1)肝移植术后6个月内出现胆道并发症;(2)临床病历资料完整;(3)行首次原位肝移植。排除标准:(1)肝移植术后1周内死亡的患者; (2)临床病历资料不完整。(3)行联合器官移植。
1.3 诊断标准 由于胆道并发症临床表现多样,肝移植术后胆道并发症的诊断尚无统一标准。肝移植术后胆道并发症的诊断主要根据临床症状 (发热、腹痛、黄疸等),引流液的性质,实验室检查,影像学检查等[9]。胆道并发症包括吻合口及非吻合口狭窄、胆漏、胆道感染、胆道出血、胆管结石和胆泥形成等[10]。胆管狭窄表现为梗阻性黄疸伴肝功能异常,磁共振胰胆管成像(MRCP)/内镜逆行胰胆管造影(ERCP)提示吻合口成角畸形伴胆管扩张者或是肝内外胆管呈串珠样改变;胆漏表现为发热、腹痛、腹膜炎,肝功能可无明显异常;引流管或诊断性腹穿刺见黄绿色胆汁样液体;术中胆道造影或探查见胆漏;胆道感染表现为发热、黄疸、腹痛,胆汁细菌培养为阳性;胆道出血表现为上消化道周期性出血,引流管持续引流出血性液体,经内镜检查排除其他部位出血;胆管结石表现为腹痛、黄疸伴有肝功能异常,B超提示胆管内高回声影,CT/MRCP 提示胆管内高密度占位,ERCP/经皮经肝胆管造影示胆管呈节段性充盈缺损且术中取石网篮取出结石。
1.4 收集指标 (1)一般资料:性别、年龄、原发病、合并症等。(2)术前血液学指标: ALT、AST、TBil、Alb、PT、ALP、GGT、血清肌酐(SCr)、γ-谷氨酰转肽酶/血小板(GPR)、中性粒细胞与淋巴细胞比值(NLR)、全身炎症反应指数/白蛋白(systemic immune-inflammation index,SⅡ /Alb);(3)手术指标:手术时间、术中失血量、术中红细胞输入量、术中输血浆量、无肝期等;根据指南对患者进行ALBI评分、MELD评分、Child-Pugh 分级。计算公式:S Ⅱ=血小板×NLR。
1.5 统计学方法 采用 SPSS 26.0 统计软件进行数据分析。正态分布的计量资料以x±s表示,两组间比较采用成组t检验;非正态分布的计量资料以M(P25~P75)表示,两组间比较使用 Mann-Whitney U检验。计数资料两组间比较采用χ2检验。对单因素分析中差异有统计学意义的指标行Logistic多因素回归分析。用ROC曲线评估危险因素的联合对肝移植术后胆道并发症的预测价值。P<0.05为差异有统计学意义。
2 结果
2.1 肝移植术后胆道并发症发生情况 在101例肝移植受者中,发生术后胆道并发症的受者有21例,发生率为20.8%,其中胆管狭窄10例、胆漏5例、胆道感染3例、胆管结石/淤泥2例、胆道出血1例。
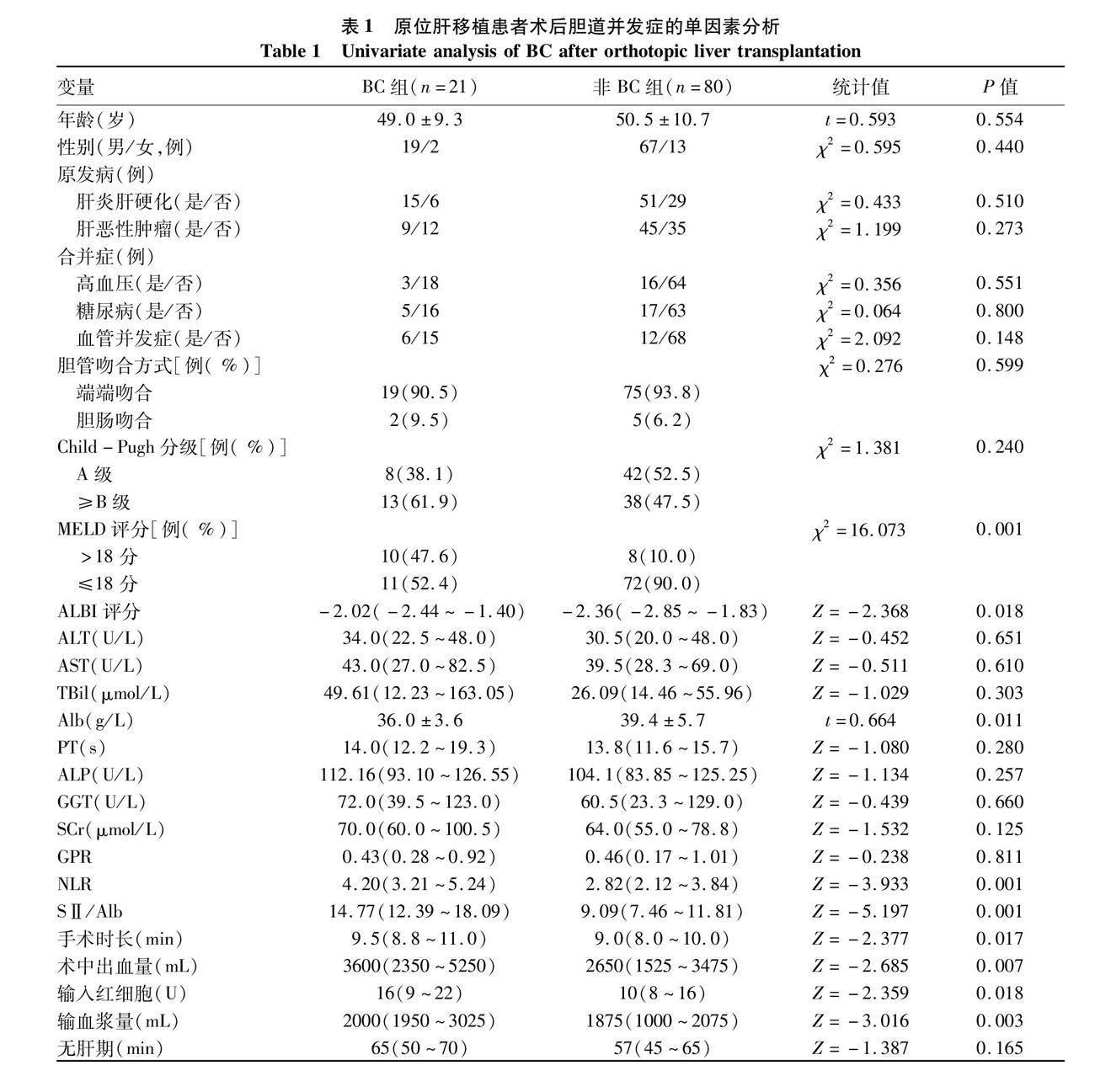
2.2 肝移植术后胆道并发症危险因素的单因素分析 BC组与非BC组受者的一般情况、血液学指标及手术相关指标见表1。单因素分析结果显示,MELD>18分、ALBI评分、Alb、NLR、SⅡ/Alb、手术时长、术中出血量、输入红细胞、输血浆量是原位肝移植术后发生胆管并发症的危险因素(P值均<0.05)。BC组与非BC组受者在年龄、性别、原发病、合并症、胆管吻合方式、ALT、AST、TBil、PT、ALP、GGT、 SCr、GPR、无肝期的差异均无统计学意义(P值均>0.05)。
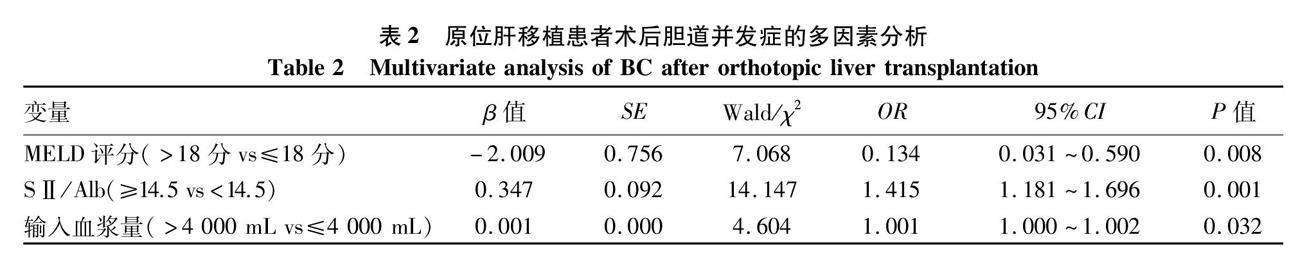
2.3 肝移植术后胆道并发症危险因素的多因素分析多因素 Logistic 回归分析结果显示:术前MELD评分、S Ⅱ /Alb、输入血浆量是肝移植术后胆道并发症的独立影响因素(P值均<0.05)(表2)。
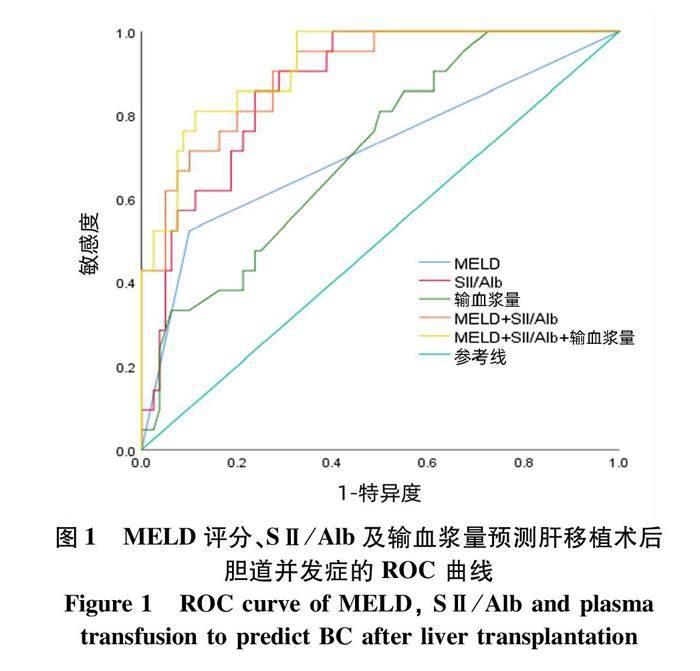
2.4 各指标对肝移植术后胆道并发症预测价值 MELD 评分、SⅡ/Alb、输入血浆量、MELD + SⅡ/Alb、MELD+SⅡ/Alb+输入血浆量的ROC曲线下面积(AUC)分别是0.712、0.870、0.712、0.900、0.918(图1,表3)。结果提示SⅡ/Alb、输入血浆量联合MELD评分对肝移植术后胆道并發症有良好的预测价值。
3 討论
肝移植是终末期慢性肝病最有效的治疗方式,但如果术后并发症的控制不理想,有可能导致移植肝功能障碍,严重影响受者的生活质量和远期生存。肝移植围手术期并发症包括术后感染、急性免疫排斥反应、胆道并发症、血管并发症、代谢并发症等。肝移植术后胆道并发症的高发病率是影响受者生存的重要原因,本研究的肝移植术后胆道并发症发病率为20.8%,与既往研究的结果类似[11-12]。本组数据分析显示胆道狭窄、胆漏和胆道感染是常见的肝移植术后胆道并发症类型。肝移植术后胆道并发症与供体营养状态、血管解剖结构、手术方案设计、术中缺血再灌注损伤、受者血流动力学状态和移植后免疫反应等有关。既往研究[13-14]发现MELD评分是肝移植术后胆道并发症的危险因素。对于MELD评分>18分的肝移植患者,其生活质量及长期生存差[15-17]。在本研究中,MELD评分>18分是肝移植术后胆道并发症的独立危险因素。S Ⅱ /Alb作为一种新型预后指标广泛应用于多种疾病模型中[18-20]。全身免疫炎症指数是肝移植术后胆道并发症的重要危险因素,能更好地预测肿瘤患者的生存率[21-22]。本研究发现肝
移植术后BC组SⅡ/Alb升高, SⅡ/Alb是肝移植术后胆道并发症的独立危险因素。与非BC组相比,BC组术中出血量和输入血浆量增加,可能与术中结扎止血不彻底、受者肝功能不全和移植肝恢复不良等因素有关。
本中心研究结果提示术中输入血浆量是肝移植术后胆道并发症的独立危险因素。胆道血供主要来自胃十二指肠动脉和右肝动脉的小分支,术中手术分离会危及胆道血运,胆道缺血会导致胆管狭窄甚至坏死,增加术后胆道并发症的风险。因此,应避免受体或供体的胆总管过分游离或烧灼,保证微弱的血供。另外,缩短供体胆管、减少多次吻合或不良吻合位置或吻合口张力过大也是极为重要的。肝移植手术时间、术中出血量与术后胆道并发症的关系目前仍尚存争议[23-24]。NLR可作为一种系统免疫标志物,其预后价值在肝癌、胃癌等多种肿瘤中都有研究[25]。受者术前NLR升高是肝移植术后受者生存率的独立预测因素[26-27]。本研究发现NLR是肝移植术后胆道并发症潜在危险因素。另外,胆道并发症的发生不受胆道重建方式的影响(包括胆管端-端吻合与胆管空肠 Roux-en-Y吻合)。年龄、合并血管并发症对肝移植术后胆道并发症的影响存在争议,本研究发现年龄、合并血管并发症与术后胆道并发症的发生无统计学相关性,与先前发表的研究相似[28-29]。本研究也存在一定的局限性,本中心肝移植数量有限,属于单中心临床回顾性研究,需大样本、多中心、前瞻性研究进行验证。
综上所述,MELD、SⅡ/Alb和输入血浆量是肝移植患者术后发生胆道并发症的独立危险因素。SⅡ/Alb、输入血浆量联合MELD评分对肝移植术后胆道并发症具有较好的预测价值和临床指导意义。
利益冲突声明:本文不存在任何利益冲突。
作者贡献声明:朱明强负责课题设计,资料分析,撰写论文;杨大帅参与数据分析;裴俊鹏、熊祥云参与收集数据;苏洋参与修改论文;丁佑铭负责拟定写作思路,指导撰写文章并最后定稿。
参考文献:
[1]
SAMUEL D, COILLY A. Management of patients with liver diseases on the waiting list for transplantation: A major impact to the success of liver transplantation[J]. BMC Med, 2018, 16(1): 113. DOI: 10.1186/s12916-018-1110-y.
[2]BERTACCO A, BARBIERI S, GUASTALLA G, et al. Risk factors for mortality in liver transplant patients[J]. Transplant Proc, 2019, 51 (1): 179-183. DOI: 10.1016/j.transproceed.2018.06.025
[3]AKAMATSU N, SUGAWARA Y, HASHIMOTO D. Biliary reconstruction, its complications and management of biliary complications after adult liver transplantation: A systematic review of the incidence, risk factors and outcome[J]. Transpl Int, 2011, 24(4): 379-392. DOI: 10.1111/j.1432-2277.2010.01202.x.
[4]FORDE JJ, BHAMIDIMARRI KR. Management of biliary complications in liver transplant recipients[J]. Clin Liver Dis, 2022, 26(1): 81-99. DOI: 10.1016/j.cld.2021.08.008.
[5]HU XW, LI T. Diagnosis and treatment of common biliary complications after orthotopic liver transplantation in adults[J]. Organ Transplant, 2022, 13(5): 569-576. DOI: 10.3969/j.issn.1674-7445.2022.05.004.
胡鑫文, 李亭. 成人原位肝移植术后常见胆道并发症的诊疗[J]. 器官移植, 2022, 13(5): 569-576. DOI: 10.3969/j.issn.1674-7445.2022.05.004.
[6]KOCHHAR G, PARUNGAO JM, HANOUNEH IA, et al. Biliary complications following liver transplantation[J]. World J Gastroenterol, 2013, 19(19): 2841-2846. DOI: 10.3748/wjg.v19.i19.2841.
[7]
TRAN LT, CARULLO PC, BANH DPT, et al. Pediatric liver transplantation: Then and now[J]. J Cardiothorac Vasc Anesth, 2020, 34(8): 2028-2035. DOI: 10.1053/j.jvca.2020.02.019.
[8]GREIF F, BRONSTHER OL, VAN THIEL DH, et al. The incidence, timing, and management of biliary tract complications after orthotopic liver transplantation[J]. Ann Surg, 1994, 219(1): 40-45. DOI: 10.1097/00000658-199401000-00007.
[9]TAI Q, HE XS, YANG JA, et al. The diagnosis and treatment of biliary complications in liver transplant patients[J]. Chin J Gen Surg, 2010, 25(12): 969-972. DOI: 10.3760/cma.j.issn.1007-631X.2010.12.010.
邰強, 何晓顺, 杨建安, 等. 肝移植术后胆道并发症的诊断与治疗[J]. 中华普通外科杂志, 2010, 25(12): 969-972. DOI: 10.3760/cma.j.issn.1007-631X.2010.12.010.
[10]FANG C, YAN S, ZHENG SS. Influencing factors, diagnosis and treatment of biliary complications after liver transplantation[J]. Chin J Gen Surg, 2014, 29(6): 486-488. DOI: 10.3760/cma.j.issn.1007-631X.2014.06.028.
方程, 严盛, 郑树森. 肝移植术后胆道并发症的影响因素及诊治进展[J]. 中华普通外科杂志, 2014, 29(6): 486-488. DOI: 10.3760/cma.j.issn.1007-631X.2014.06.028.
[11]KALTENBORN A, GUTCKE A, GWIASDA J, et al. Biliary complications following liver transplantation: Single-center experience over three decades and recent risk factors[J]. World J Hepatol, 2017, 9(3): 147-154. DOI: 10.4254/wjh.v9.i3.147.
[12]SARHAN MD, OSMAN AMA, MOHAMED MA, et al. Biliary complications in recipients of living-donor liver transplant: A single-center review of 120 patients[J]. Exp Clin Transplant, 2017, 15(6): 648-657. DOI: 10.6002/ect.2016.0210.
[13]WIEDERKEHR JC, IGREJA MR, NOGARA MS, et al. Analysis of survival after primary liver transplantation: Multivariate analysis of 155 cases in a single center[J]. Transplant Proc, 2010, 42(2): 511-512. DOI: 10.1016/j.transproceed.2010.01.014.
[14]GIRARD E, RISSE O, ABBA J, et al. Internal biliary stenting in liver transplantation[J]. Langenbecks Arch Surg, 2018, 403(4): 487-494. DOI: 10.1007/s00423-018-1669-y.
[15]YOON JU, BYEON GJ, PARK JY, et al. Bloodless living donor liver transplantation: Risk factors, outcomes, and diagnostic predictors[J]. Medicine, 2018, 97(50): e13581. DOI: 10.1097/MD.0000000000013581.
[16]JACOB M, COPLEY LP, LEWSEY JD, et al. Pretransplant MELD score and post liver transplantation survival in the UK and Ireland[J]. Liver Transpl, 2004, 10(7): 903-907. DOI: 10.1002/lt.20169.
[17]ODEN-BRUNSON H, MCDONALD MF, GODFREY E, et al. Is liver transplant justified at any MELD score?[J]. Transplantation, 2023, 107(3): 680-692. DOI: 10.1097/tp.0000000000004345.
[18]LIU CC. Real-world study on SII/ALB ratio to predict the efficacy of immune checkpoint inhibitors in the treatment of malignant tumors[D]. Dalian: Dalian Medical University, 2021.
刘成成. SII/ALB比值预测免疫检查点抑制剂治疗恶性肿瘤疗效真实世界研究[D]. 大连: 大连医科大学, 2021.
[19]LI HW, WANG GC, ZHANG HH, et al. Prognostic role of the systemic immune-inflammation index in brain metastases from lung adenocarcinoma with different EGFR mutations[J]. Genes Immun, 2019, 20(6): 455-461. DOI: 10.1038/s41435-018-0050-z.
[20]AN R, QIN C, WU Q, et al. Predictive value of systemic immune inflammation index (SII)in the short-term prognosis of patients with dilated cardiomyopathy[J]. Clin J Med Offic, 2022, 50(11): 1129-1133. DOI: 10.16680/j.1671-3826.2022.11.07.
安然, 秦璨, 武瓊, 等. 全身免疫炎症指数对扩张型心肌病患者预后预测价值[J]. 临床军医杂志, 2022, 50(11): 1129-1133. DOI: 10.16680/j.1671-3826.2022.11.07.
[21]REN A, LI ZQ, CHENG PR, et al. Systemic immune-inflammation index is a prognostic predictor in patients with intrahepatic cholangiocarcinoma undergoing liver transplantation[J]. Mediators Inflamm, 2021, 2021: 6656996. DOI: 10.1155/2021/6656996.
[22]FU HY, ZHENG J, CAI JY, et al. Systemic immune-inflammation index (SII) is useful to predict survival outcomes in patients after liver transplantation for hepatocellular carcinoma within Hangzhou criteria[J]. Cell Physiol Biochem, 2018, 47(1): 293-301. DOI: 10.1159/000489807.
[23]LICHTENEGGER P, SCHIEFER J, GRAF A, et al. The association of pre-operative anaemia with survival after orthotopic liver transplantation[J]. Anaesthesia, 2020, 75(4): 472-478. DOI: 10.1111/anae.14918.
[24]JZ'WIK A, KARPETA E, NITA M, et al. Impact of blood loss and intraoperative blood transfusion during liver transplantation on the incidence of early biliary complications and mortality[J]. Transplant Proc, 2020, 52(8): 2477-2479. DOI: 10.1016/j.transproceed.2020.03.052.
[25]CHU HH, KIM JH, SHIM JH, et al. Neutrophil-to-lymphocyte ratio as a biomarker predicting overall survival after chemoembolization for intermediate-stage hepatocellular carcinoma[J]. Cancers (Basel), 2021, 13(11): 2830. DOI: 10.3390/cancers13112830.
[26]NYLEC M, DERBISZ K, CHRZSZCZ P, et al. Preoperative neutrophil-to-lymphocyte ratio as an independent predictor of 1-year graft loss and mortality after orthotopic LiverTransplantation[J]. Transplant Proc, 2020, 52(8): 2472-2476. DOI: 10.1016/j.transproceed.2020.03.036.
[27]KWON HM, MOON YJ, JUNG KW, et al. Neutrophil-to-lymphocyte ratio is a predictor of early graft dysfunction following living donor liver transplantation[J]. Liver Int, 2019, 39(8): 1545-1556. DOI: 10.1111/liv.14103.
[28]LU A, SOLANAS E, BAPTISTA P, et al. How important is donor age in liver transplantation?[J]. World J Gastroenterol, 2016, 22(21): 4966-4976. DOI: 10.3748/wjg.v22.i21.4966.
[29]ZHANG QB, SHEN CH, TAO YF, et al. Risk factor analysis and classified therapeutic strategies for biliary complications after liver transplantation from organ donation by citizens after death: A report of 48 cases at a single center[J]. Chin J Organ Transplant, 2020, 41(10): 623-628. DOI: 10.3760/cma.j.cn421203-20191115-00415.
張全保, 沈丛欢, 陶一峰, 等. 肝移植术后胆道并发症的危险因素分析及分类治疗策略[J]. 中华器官移植杂志, 2020, 41(10): 623-628. DOI: 10.3760/cma.j.cn421203-20191115-00415.
收稿日期:
2022-11-24;录用日期:2023-01-09
本文编辑:王莹