Diabetes knowledge and self-care practices among people living with type 2 diabetes mellitus in a diabetes clinic in Southwestern Nigeria
2023-01-07TimothyTitilayoFAMAKINWAOyeninhunAbimbolaOLUWATOSINJoelOlayiwolaFARONBIFunmilolaAdenikeFAREMIAdeyemiOGUNLEYEChinmaStellaADERETIMatthewIdowuOLATUBI
Timothy Titilayo FAMAKINWA,Oyeninhun Abimbola OLUWATOSIN,Joel Olayiwola FARONBI,Funmilola Adenike FAREMI,Adeyemi OGUNLEYE,Chinma Stella ADERETI,Matthew Idowu OLATUBI
1Department of Nursing Science,Obafemi Awolowo University,Ile-Ife,Osun State,Nigeria;2Department of Nursing,University of Ibadan,Ibadan,Oyo State,Nigeria;3Department of Chemical Pathology,University of Medical Sciences Teaching Hospital,Ondo,Ondo State,Nigeria;4Department of Nursing Science,Bowen University,Iwo,Osun State,Nigeria
ABSTRACT Objective:The objective of this study is to assess the knowledge and self-care practices of people living with type 2 diabetes mellitus (T2DM).Materials and Methods:The study was conducted in a clinic in Southwestern Nigeria.It adopted a cross-sectional design.The sample consists of 107 people living with T2DM.Data were collected using Diabetes Knowledge Questionnaire and Revised Self-care Inventory Scale.Results:The mean diabetes knowledge of the participants was 16.2 ± 3.0 and 70.1% had inadequate knowledge of T2DM.The mean diabetes self-care practice score among the participants was 49.9 ± 4.9,and 89.7% reported poor diabetes self-care practice.There is no significant difference in the knowledge of diabetes between male (16.42 ± 3.42) and female (16.12 ± 2.8) participants (t=0.45; P =0.65),and no significant difference in self-care practice of male (49.23 ± 4.51) and female (50.06 ± 5.07) participants (t=0.75, P =0.46).In addition,there is no correlation between age and knowledge of diabetes (r =-0.18, P =0.07) and self-care practices (r=0.08, P =0.38) of participants.No significant relationship was found between knowledge of diabetes and diabetes selfcare practices (χ2=1.605,P=0.448)Conclusion:Knowledge of diabetes and self-care practices of people living with T2DM in this study were poor.Effort should be directed at improving their diabetes knowledge and self-care practices.
Keywords: Adherence,clinic,knowledge,self-care practices,type 2 diabetes mellitus,type 2 diabetes
INTRODUCTION
Diabetes mellitus is a chronic noncommunicable metabolic disorder that is of great concern to world health leaders due to its fast-growing prevalence worldwide.Globally an estimated 425 million adults between 20 and 79 years of age were living with diabetes in 2017,and by 2045,this may increase to 629 million.[1]In 2021,Nigeria has a diabetes prevalence of 3.6%among adults aged 20-79 years.[2]The increasing morbidity and mortality associated with diabetes lead to physical disabilities and social and economic losses with adverse consequences on the individual,family,and society.Minimizing these consequences largely depends on adequate management of type 2 diabetes mellitus (T2DM) to achieve glycemic control.
The management of T2DM requires lifestyle modification through self-care practices.Similarly,adherence to self-care practices depends on the patients’ knowledge and understanding of T2DM and its diabetes management.[3]Patients’ inadequate knowledge about T2DM control targets and self-care practices had been documented to be associated with poor glycemic control.[3,4]Furthermore,good knowledge of T2DM is known to be associated with better management outcomes in terms of decreases in glycated hemoglobin values and adherence to T2DM self-care behaviors.[5,6]
However,poor glycemic control among people living with T2DM remains a challenge.[7-9]The American Diabetes Association in 2016,reported that an estimated 30%-49% of diabetic patients do not have adequate control of blood sugar,blood pressure,or blood cholesterol and that only 14% have adequate control of these three factors.[10]In Nigeria,scholars had also documented poor glycemic control among people living with T2DM.[7]
Poor T2DM-related knowledge had been documented among people living with T2DM in India,[11]Ethiopia,[3]and Nigeria.[12]Furthermore,Bayemet al.[13]documented that the majority of people living with T2DM in Nigeria had issues with diabetes self-care practices.Oparaet al.[14]further found out in a study among people living with T2DM in Enugu and Nigeria that adherence to diabetes self-care practices was very poor.It had also been documented in some settings that the state of glycemic control can be improved if patients’ knowledge of diabetes and self-care behaviors improved.[5,13,15]
A significant relationship had been found to exist between T2DM knowledge and self-care practice among people living with T2DM in Malta,[16]India,[17]Malaysia,[18]and Ethiopia.[15]However,little is known about the relationship between T2DM-related knowledge and self-care among people living with T2DM in Southwestern Nigeria.Therefore,the purpose of this study was to assess the knowledge of diabetes management and self-care practices among people living with T2DM and determine the relationship between respondents’knowledge and reported self-care practices.
MATERIALS AND METHODS
Study design
The study adopted a cross-sectional design.
Setting
Data were collected from March to June 2019 in the diabetes clinic of State Specialist Hospital,Ondo,Ondo State.The hospital provides both in-patients and out-patients health services to individuals with diverse care needs including people living with T2DM.The diabetes clinic essentially provides follow-up care in the areas of medication,glucose monitoring,and patient education.Physicians,nurses,and nutritionists/dieticians work in the clinic which attends to the clients on Tuesday of every week.
Study population and sampling strategy
The study population consists of 107 patients with T2DM attending the diabetes clinic.The sample size was determined using Kirk and Sterne (2003) formula.[19]The power of the study was 0.983 with the level of significance set at 95%.Simple random sampling technique using the ballot system was employed to recruit participants for the study.Only people that had been diagnosed with T2DM for at least 2 years were recruited for the study.
Data collection
Information about participants’ knowledge was obtained with a validated Diabetes Knowledge Questionnaire (DKQ).[20]The DKQ is a 24-item scale that evaluates diabetes knowledge in the areas of cause,diagnosis,glucose monitoring,diet,complications,and exercise.DKQ has a reliability value of alpha 0.74.Response variables in the DKQ were Yes,No,and I don’t know.Diabetes-related knowledge was evaluated as a percentage of correct answers and the mean score was calculated.Scores above the mean score were categorized as good knowledge,whereas scores below the mean (16.2)were categorized as fair and poor knowledge,respectively.The DKQ has documented Cronbach’s alpha coefficients (α)score of 0.78.In the pilot study,it has a score of 7.0.
Adherence to self-care practices was evaluated with revised Self-Care Inventory scale (SCI-R).[21]SCI-R is a self-report 15-item Likert-type scale with “Never=1,” “Rarely=2,”“Sometimes=3,” “Usually=4,” and “Always=5.” The scale allows for the possibility of varying treatment and also evaluates the individual’s perception.For analysis,the response variables on diabetes SCI-R were assigned numerical values of 1,2,3,4,and 5,respectively,thus the score ranged from 15 to 75.Participants’ performance was categorized as good practice (70% and above),fair practice (50%-69%),and poor practice (below 50%).The SCI-R scale has a documented α score of 0.87[21]and 0.82 in the pilot study.
The data were collected by two of the authors who are well-grounded in survey data collection.The questionnaire was administered to the prospective participants during their clinic appointments.The questionnaire was retrieved after satisfactory completion.Totally 120 questionnaires were administered but only 107 were retrieved and satisfactorily filled giving a response rate of 89.17%.Data were collected over 3 months.
Statistical analysis
Data analysis was done with SPSS version 20 manufactured by IBM Corporation,Armonk,New York,the USA[22]using descriptive (frequency counts and percentages) and inferential statistics (Correlation coefficient,Chi-square test,and Student’st-test).Student’st-test was used to ascertain differences in the knowledge of diabetes and self-care practices of male and female participants in the study while the correlation coefficient was used to establish relationship between the age of the participants and between knowledge of diabetes and self-care practices.Chi-square was used to test the relationship between knowledge of diabetes and self-care practices among the participants.
Ethical considerations
Approval was obtained from the Research Ethics Committee of Ondo State Ministry of Health (AD.4693/315) on January 15,2019.In addition,written consent was obtained from the participants.The instruments were given to the participants who could read and write while those who could not,were assisted by the research assistants who read and interpreted the items on the instruments to each client and their responses were documented accordingly.
RESULTS
Table 1 presents the sociodemographic characteristics of the participants.All 107 participants duly completed and returned the questionnaire,representing a 100% response rate.Forty-two point one percent (42.1%) of the participants were within the age range of 60 and 69 years.The mean age of the participants in the study was observed to be 65.1 ± 9.4 years.The majority (75.7%) of the patients that participated in the study were females,53.3% had no formal education,whereas 82.2% were employed.
Only 29.9% of the participants had good knowledge of diabetes,and 45.8% and 24.3% had fair and poor knowledge of diabetes,respectively [Table 2].Better knowledge was demonstrated in the area of diabetes diagnosis (80.5%),diet management (83.2%),and clinical manifestations/complications (89.1%).The mean diabetes knowledge of the participants was 16.2 ± 3.0.No significant difference in the knowledge of diabetes between male (16.4 ± 3.4) and female (16.1 ± 2.8) participants with T2DM,(t=0.45;P=0.65).Furthermore,no correlation exists between the age of the participants and their knowledge of diabetes (r=-0.18,P=0.07).
Self-care practices among the participants in this study showed that only few (10.3%) reported good diabetes self-care practices while the majority (89.7%) have fair diabetes self-care practices.The mean diabetes self-care practice score among the participants in the study was 49.9 ± 4.9.Furthermore,there is no significant difference in diabetes self-care practice of male (49.2 ± 4.5) and female (50.1 ± 5.1)participants in the study (t=0.75,P=0.46).There is no significant correlation between the age of the people living with T2DM that participated in this study and their diabetes self-care practices (r=0.08,P=0.38).
As regards the relationship between the participants’knowledge and reported self-care practices,findings from the Chi-square test showed no significant relationship between knowledge of diabetes and diabetes self-care practices [Table 2].
DISCUSSION
Adequate knowledge of diabetes and effective self-care practices are key factors in achieving glycemic controlin people living with T2DM.[3,23-25]The patients take daily decisions about their care,make choices concerning self-care behaviors,and ultimately take control of their care to promote well-being and prevent complications.In this study,results showed that 24.3% of the participants’ demonstrated overall poor knowledge of diabetes and diabetes self-care.This implies that a good number of people living with T2DM that participated in this study were not knowledgeable about diabetes and diabetes self-care.This is similar to poor knowledge of diabetes documented among people attending outpatient diabetes clinics in Ethiopia,[3]India,[11]Nigeria,[12]and Zimbabwe.[26]In many developed nations,knowledge of diabetes among people living with T2DM is better than what was documented in this study.[27]However,another related study reported fair knowledge of diabetes among people living with T2DM in Ibadan,southwestern Nigeria.[28]The reason for this might be due to the fact that Ibadan is an urban city with better access to health care and health information compared to Ondo where this study was carried out.
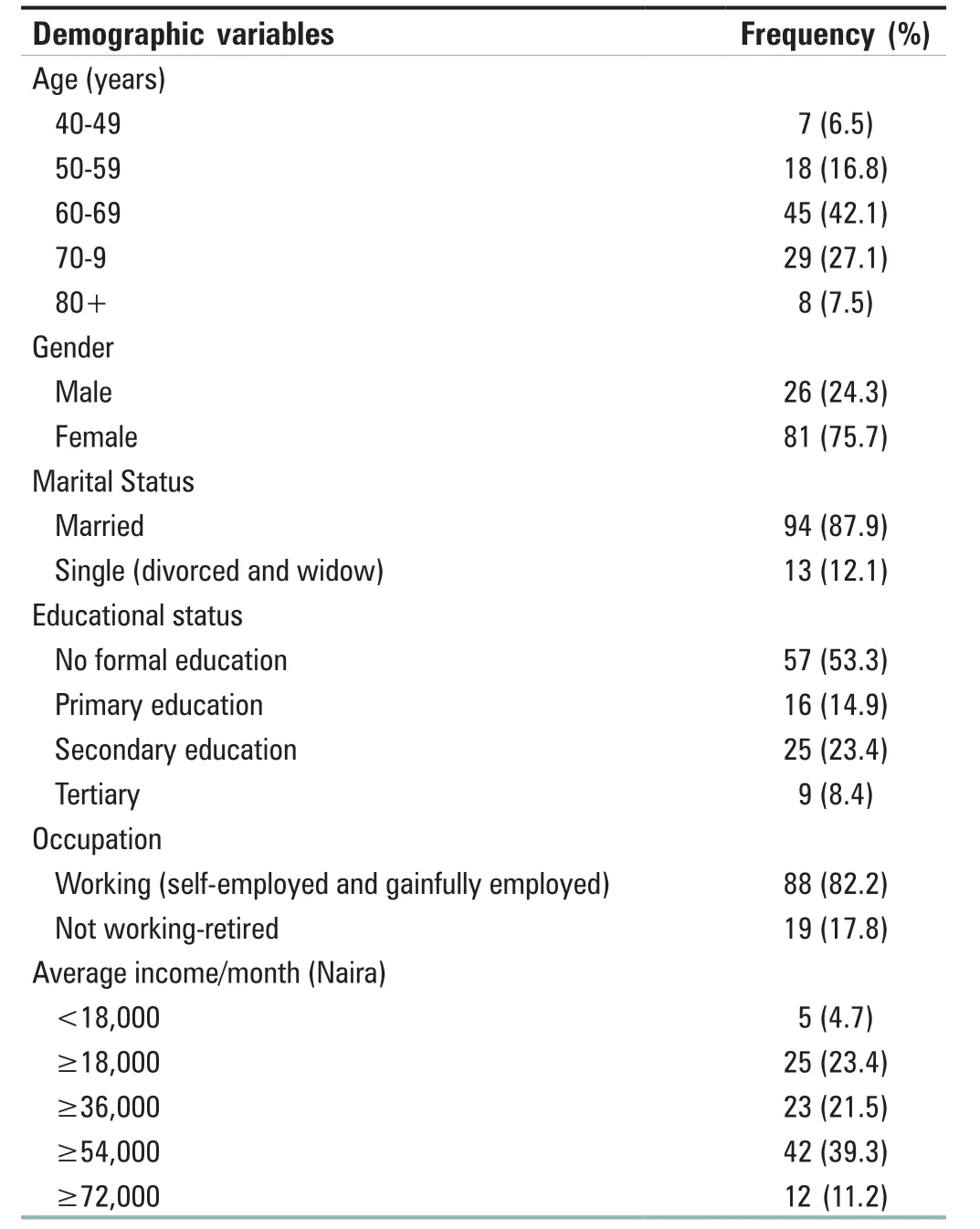
Table 1: Participants’ sociodemographic characteristics
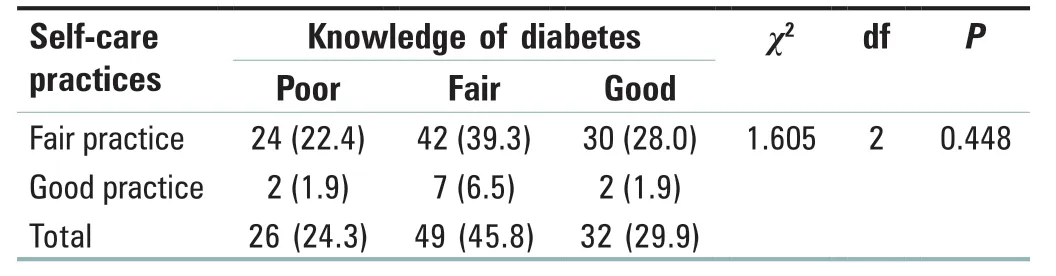
Table 2: Relationship between participants’ knowledge and reported self-care practice
While assessing the knowledge of people living with T2DM about different aspects of diabetes self-care,it was reported that only few of the participants in their study have good nutritional knowledge about diabetes.[29]Results of our study,however,showed good nutritional knowledge among patients that participated in the study.This is probably due to frequent education on the dietary management of diabetes that is provided in the clinic where our study was carried out.Also,this study documented good knowledge of clinical manifestations and complications of diabetes among the participants.This had also been documented among people living with T2DM in the Southeastern part of Nigeria.[30]
Participants’ knowledge on the diagnosis of diabetes was also found to be very high.The participants’ knowledge may be a result of adequate education provided by health-care providers to the patients.It is recommended that diabetes education should be made available to patients on diagnosis and on on-going basis.The findings about the overall knowledge of the participants about diabetes are similar to the findings of Dineshet al.except their findings about knowledge of complications of diabetes.[31]
Ubajakaet al.[32]documented a significant relationship between gender and knowledge of diabetes in a study among secondary school teachers in the eastern part of Nigeria.However,this study found that there is no significant difference in the diabetes knowledge of male and female patients living with T2DM that participated in this study.This might be probably due to the fact that our study was carried out among people living with T2DM while Ubajakaet al.’s study was carried out among the general population.Furthermore,the weak insignificant relationship was found between age and knowledge of diabetes among participants in this study.
No significant difference in the knowledge of diabetes between male (16.42 ± 3.42) and female (16.12 ± 2.8) participants with T2DM that participated in the study (t=0.45;P=0.65).Furthermore,no correlation exists between the age of the participants and their knowledge of diabetes (r=-0.18,P=0.07).However,Formosa and Muscat[16]found a positive correlation between the age of people living with T2DM and their knowledge of diabetes,which is not consistent with results of our study.
Findings from our study also showed that participants adhered poorly to blood glucose monitoring,which is similar to the findings of previous studies.[12,13,29]In a systematic review of adherence to diabetes self-care,adherence with blood glucose monitoring among people living with T2DM was reported to be between 17.0% and 77.45% depending on the setting where the study was carried out.[33]Mogreet al.’s review further showed that studies conducted in poor nations like our study,have poor adherence to blood glucose monitoring.[34]Therefore,poor adherence to blood glucose in our study might probably be due to the unavailability of glucometer for the personal use of many of the participants in this study.[12,13]
Although participants in this study have good knowledge of dietary management of diabetes,dietary-related practices in the management of diabetes were found to be poor.[13,30]This is at variance with moderate dietary self-care practices among people living with T2DM documented by Ketemaet al.[35]Nearly all the participants reported taking the correct doses of diabetes pills and 82 of them take their medications at the right time corroborating submissions of previous studies.[30,32]
Overall,participants reported adherence to self-care practices was fair.This is better than poor adherence to diabetes self-care practices reported among people living with T2DM in Enugu Nigeria,[14]and India.[36]A possible reason for the participants’ better adherence to medication is their reported belief that untreated or poorly controlled diabetes would cause an increase in blood sugar levels and possible complications.This is,however,in contrast with the findings by Dineshet al.,[31]where only 48% of their study participants take the recommended hypoglycemic agents and insulin daily.Results of our study showed that there is no relationship between gender,age,and self-care practices of people living with T2DM that participated in the study,contrary to findings of previous studies.[28,32]
The participants’ poor knowledge of diabetes and diabetes care reflected in their reported self-care practices which were fair.This shows the importance of diabetes patient education as an integral component of diabetes care to encourage effective self-care practices.On the relationship between participants’ knowledge of diabetes and self-care practices,findings showed no statistically significant relationship them.Patients with adequate knowledge of diabetes are more likely to better engage in self-care than those with poor knowledge.
Assessing practice from participants’ point of view is prone to bias.This study uses a standardized scale that had been used in previous studies to increase the correctness of the results.Similarly,this study was conducted in a single setting,multiple settings would have yielded broader findings and generalization.
CONCLUSION
The participants in this study demonstrated inadequate knowledge of diabetes and diabetes self-care and their reported performance in self-care activities was below average.To minimize T2DM complications,there is a need for improved diabetes patient education.Similarly,no difference in the knowledge of diabetes and diabetes self-care among male and female participants in this study.This will help patients to engage better in self-care behaviors and thus prevent complications while experiencing good quality of life.
Acknowledgment
The authors appreciate the support of the following people Mr.Ogunleye A,Mrs.O.Araoyinbo,Mrs.O.Ezekiel,Mrs.B.O Adegoke,Rev.Sister Oluwole,and the entire staff of Diabetes Clinic,State Specialist Hospital,Ondo City,Ondo State.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
杂志排行

Journal of Integrative Nursing的其它文章
- Evaluation of adolescent/youth-friendly sexual and reproductive health services: A 7-year systematic review from January 2016 to April 2022
- Symptom experience in patients with cancer-related fatigue: A systematic review and meta-synthesis
- Drivers of early marriage and teenage pregnancy in Kenya and Uganda during COVlD-19 lockdown period:A systematic review
- Dredging hand Yang meridians with deep tissue massage combined with neck movement in stiff-neck syndrome:A randomized controlled trial
- Quality of life and psychological impact among chronic disease patients during the COVlD-19 pandemic
- Job satisfaction and organizational commitment among nurses working on temporary versus permanent jobs at a tertiary care teaching hospital,Uttarakhand,lndia