Lymphocyte count and A-DROP score in COVID-19 patients: A retrospective observational study
2022-07-02ChandrakantWaikarVinayakGourLalPranaySevrasHingwe
Chandrakant Waikar, Vinayak Gour, Lal Pranay, Sevras Hingwe✉
Departments of 1Anaesthesiology and 2Pathology, ABV Medical College, Vidisha, India
ABSTRACT
KEYWORDS: COVID-19; Pandemic; Lymphopenia; Pneumonia
1. Introduction
Coronavirus disease 2019 (COVID-19) is a public health emergency across the world[1]. In India, there are 182 143 cases and 5 164 deaths recorded till May 2020. While most patients are either asymptomatic or have a mild influenza-like illness, some infected patients develop various manifestation as pneumonia,acute respiratory distress syndrome, multi-organ dysfunction, and even lethal outcome[2,3]. Judicious use of resources is essential in this pandemic and therefore early identification of severe disease by initial assessment will permit the allocation of resources effectively. Lymphopenia is associated with severe COVID-19,and severe COVID-19 patients were found to have a significantly lower lymphocyte count[4,5]. The scoring systems used for risk stratification include CURB-65 (confusion, urea, respiratory rate,systolic blood pressure, age), PSI (Pneumonia Severity Index),SMART-COP (systolic blood pressure, multilobar chest X-ray,involvement, albumin, respiratory rate, tachycardia, confusion,oxygen low, arterial pH), National Early Warning Score 2(NEWS2) and Quick Sequential Organ Failure Assessment Score B (qSOFA score). In COVID-19 patients, A-DROP score predicts efficiently the death of hospitalized patients compared to CURB-65, PSI, SMART-COP, NEWS2, and qSOFA scores and is used as a reliable tool for risk stratification[5]. The Japanese Respiratory Society proposed a 6-point scale (0-5) to assess the clinical severity of community-acquired pneumonia[6,7]. The A-DROP scoring system uses the following parameters: (1) Age (male≥70 years,female≥75 years); (2) Dehydration (blood urea nitrogen≥210 mg/L); (3) Respiratory failure (SPO2≤90% or PaO2≤60 mmHg); (4)Orientation disturbance (confusion); (5) Low blood pressure (systolic blood pressure≤90 mmHg). Each point gives 0 or 1 point and the cumulated score suggests the severity of the disease. The prognostic value of lymphopenia alone is limited. In this respect, its additive value to the existing severity score is unknown. The objective of the study was to find out the correlation between lymphocyte count and A-DROP score in COVID-19 patients and their role in predicting poor outcomes.
2. Patients and methods
2.1. Study design
This retrospective observational single-center study was conducted in a tertiary care hospital in Vidisha district, India. Reverse transcription-polymerase chain reaction positive patients were included in this study who were admitted to ICU and the COVID Care Centre from August 2020 to October 2020.
2.2. Ethical approval
Ethical approval was taken from the Institutional Ethics Committee of ABV Medical College (Ref. No. 21(a)/IEC/ABVGMC/Vidisha/2020).
2.3. Inclusion and exclusion criteria
Patients above the age of 18 years with positive RTPCR results admitted to ICU and COVID Care Centre (as per national guidelines released by Indian Council of Medical Research) were included in this study.
Patients aged <18 years, pregnant patients and lactating patients,patients with previously diagnosed with any malignancy, noninfectious pulmonary interstitial lung disease, and current tuberculosis on treatment, psychiatric disorder, or mental retardation affecting mental status examination, antibiotic therapy before the present admission were excluded from this study.
2.4. Data collection
All data related to the study were collected from patients’ records available in the hospital during the study period from August 2020 to October 2020. Demographic profile, clinical characteristics,medical history, A-DROP score, complete blood counts including lymphocyte counts (on admission), the severity of the disease course,and duration of hospitalization were collected from hospital records and reviewed by an independent doctor. Data on IL-6 and neutrophil to lymphocyte ratio were not collected as data regarding these were limited to very few patients in the records.
2.5. Operative definition (criteria for admission in ICU and COVID Care Centre)
(1) Mild COVID-19 refers to without evidence of breathlessness or hypoxia (normal saturation);
(2) Moderate COVID-19 refers to pneumonia with no signs of severe disease i.e., adolescent or adult without the presence of clinical features of dyspnea and or hypoxia, fever, cough, including SpO2<94% (range 90%-94%) on room air, the respiratory rate more or equal to 24 per minute;
(3) Severe COVID-19 refers to severe pneumonia i.e., Adolescent or adult with clinical signs of pneumonia plus one of the following:Respiratory rate>30 breaths/min, severe respiratory distress,SpO2<90% on room air;
(4) Lymphopenia refers to lymphocyte counts≤1 000 cells/μL (the cut-off point is considered in our study);
(5) The definition of severe disease and the unfavorable outcome was based on clinical symptoms, i.e., patients having severe dyspnea,extremely low oxygen saturation, respiratory distress, or requiring endotracheal intubation, mechanical ventilation and death.
2.6. Statistical analysis
With a typeⅠerror of 0.05 and a power of 80%, we calculated a sample size of 194, so we recruited 220 patients to avoid attrition and dropouts.
IBM SPSS statistics software, version 25.0 was used for statistical analysis. Shapiro-Wilk test and visual inspection of box plot were used to determine normal distribution of continuous variable.Continuous variables were presented as the mean±SD for normally distributed data. Categorical variables were described as counts(%). The area under the receiver operating curve (ROC) for the prediction of endotracheal intubation was used for lymphocyte count and A-DROP score. Pearson’s correlation coefficients were used to determine the relationship between two variables. The correlation was considered significant at P<0.05.
3. Results
We recruited 220 COVID-19 patients who were admitted to the tertiary care center ICU from August 2020 to October 2020.In the total of 220 patients, 134 were male, and 86 were female[mean age (48.98±16.98) years, 95% CI: 46.72-51.23]. Thirty-seven of recruited patients had lymphopenia upon admission.Patients who admitted in ICU have hypertension (n=49), chronic obstructive pulmonary disease (n=43), congestive cardiac failure(n=30), diabetes mellitus (n=26), cerebrovascular disease (n=3),chronic renal disease (n=2), liver diseases (n=3) (Table 1).Clinical parameter for A-DROP score included age≥70 years(male=37),≥75 years (female=18), dehydration (n=45), SpO2≤90%(n=41), orientation/confusion (n=22), systolic blood pressure 90 mmHg (n=16). Besides, 114 patients had an A-DROP score of 0,56 patients of 1, 26 patients of 2, 17 patients of 3, 5 patients of 4, and 2 patients of 5 (Table 2). Noninvasive ventilation and high flow nasal oxygen were used in 23 and 29 patients respectively.Invasive ventilation (endotracheal intubation) was required in 28 patients. The average duration of ICU stay was (10.29±3.31) d.

Table 1. Baseline and outcome measures of COVID-19 patients.

Table 2. A-DROP scores and lymphocyte counts.
The correlation of lymphocyte count and A-DROP score showed in Figure 1. Lymphocyte count in COVID-19 patients correlated negatively with the A-DROP score (r=-0.673, P<0.05).Both A-DROP score and lymphopenia were able to predict an increased chance of intubation (Figure 2). The area under the ROC curve was 0.892 (95% CI: 080-0.98, P<0.001) for the lymphocyte count, and the area under the ROC curve was 0.93(95% CI: 0.84-1.00, P<0.001) for lymphocyte count-A-DROP.Area under receiver operating characteristic curve of lymphocyte count and that of combined lymphocyte count-A-DROP score was comparable for the prediction of endotracheal intubation.

Figure 1. Correlation of lymphocyte counts and A-DROP scores.
4. Discussion
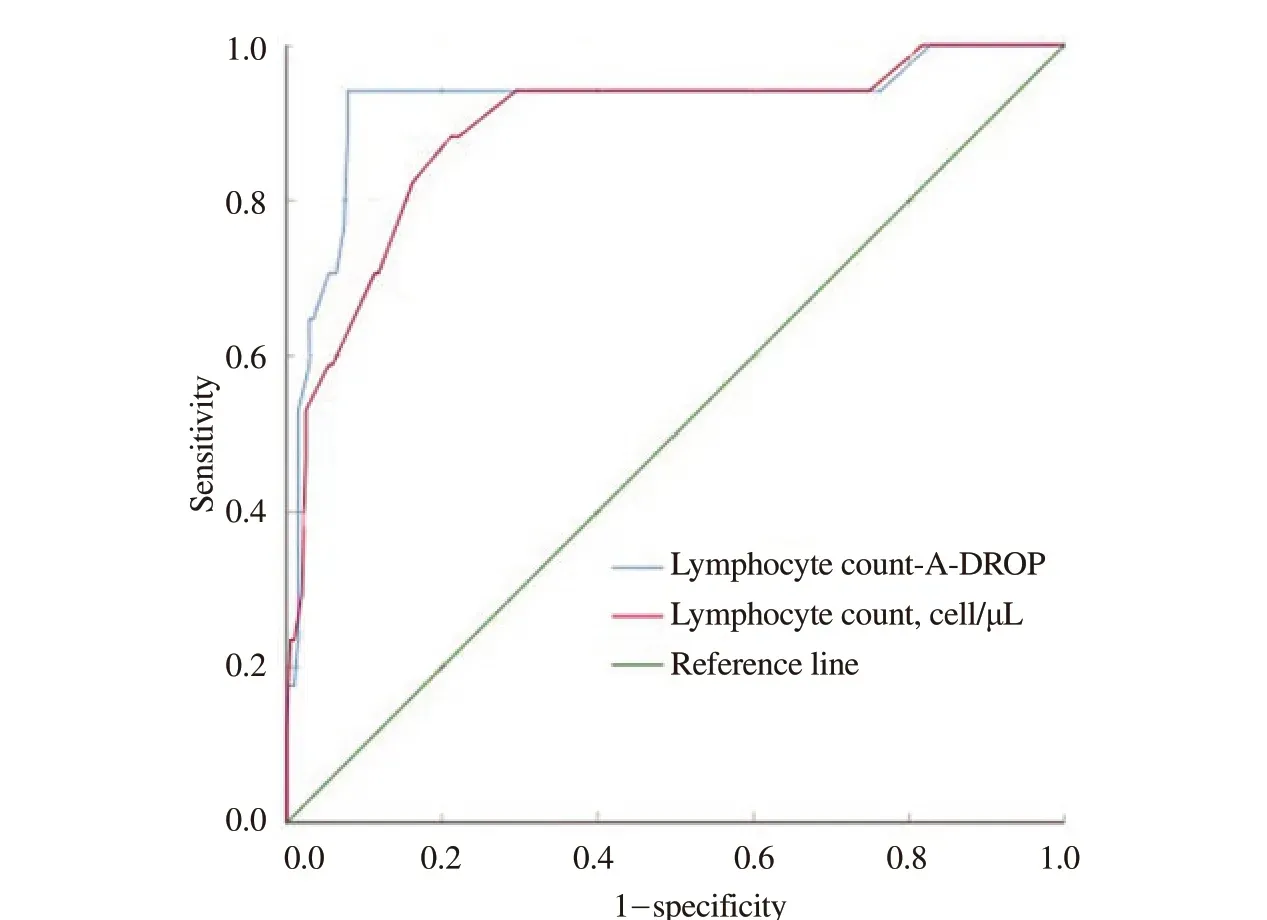
Figure 2. ROC curve of lymphocyte count and combined lymphocyte count-A-DROP score for endotracheal intubation.
In the present study, we analyzed the correlation between lymphopenia and A-DROP score in the severity of COVID-19 and found out that lymphopenia in COVID-19 patients correlated negatively with A-DROP score. Low lymphocyte counts (<1 000/μL) were found in various types of virus-infected diseases such as severe acute respiratory syndrome (SARS), Middle East Respiratory Syndrome, and respiratory syncytial viral. Human T lymphocytes are infected and destroyed by MERS-CoV and SARS-CoV, which leads to the destruction of lymphocytes by apoptosis and causes lymphopenia[8-10]. These are pathological similarities of COVID-19 to SARS and MERS. However,the clinical manifestation of COVID-19 may be more asymptomatic during the first phase of COVID-19 in India. The complete blood count with lymphocyte counts is most commonly used to determine the severity of inflammation. There are various scoring systems for the initial assessment of patients and their prognosis, and the A-DROP score is identified better than other scoring systems. The different scoring system has a disparity in the definition of elderly patients and the evaluation of the respiratory condition. These two characteristics directly correlate to poor outcomes in COVID-19 pneumonia. In the COVID-19 pandemic when resources are limited, it is prudent to use resources appropriately. Early determination of the severity of COVID-19 is essential to use resources appropriately. Lymphopenia along with the A-DROP score helps in determining severity and early intervention in COVID-19 pneumonia. Lymphopenia is seen in severe COVID-19 pneumonia and correlates with disease outcomes[11-13].We have selected the A-DROP score because of its simplicity and easy applicability in COVID-19 patients at the time of the initial assessment by clinical physicians and paraclinical physicians[7,14]. In SARS-CoV-2 infection, cytokine storms are caused by the secretion of a huge amount of proinflammatory cytokines, interleukins[15,16], and chemokine which have an important role in the occurrence of SARS-CoV-2 related complications e.g. acute respiratory distress syndrome[14,17,18], these are associated with COVID-19 severity. In previous studies, the A-DROP score showed better accuracy in in-hospital death prediction compared to other current widely used community-acquired pneumonia-specific tools. Patient’s age (male≥70 years, female≥75 years) and respiratory condition (SPO2≤90% or PaO2≤60 mm Hg) directly correlate to poor outcomes in COVID-19 pneumonia. Lymphopenia along with the A-DROP score helps in determining severity and early intervention in COVID-19 pneumonia.
There are some limitations of this study. First, it is a retrospective single center study, as the prospective study design was difficult in the COVID-19 pandemic. Second, the sample size is small for this study,so a large sample size is required for validating the conclusion. Third,we have analyzed lymphocyte count at the time of admission only,although low lymphocyte count during ICU stays also has an impact on the poor outcome.
To sum up, lymphopenia and A-DROP score on admission effectively correlate with the severity of COVID-19 pneumonia and unfavorable outcome.
Conflict of interest statement
The authors report no conflict of interest.
Funding
This study received no extramural funding.
Authors’ contributionsThe authors confirmed contributions to the paper as follows: study conception and design: S.H., C.W.; Data collection: L.P. and V.G.;Analysis and interpretation of results: S.H., C.W., V.G.; Draft manuscript preparation: S.H. All authors reviewed the results and approved the final version of the manuscript.
杂志排行

Journal of Acute Disease的其它文章
- Efficacy of gabapentin for low back pain at a tertiary hospital: A prospective observational study
- Leukemoid reaction in a patient with COVID-19 infection: A case report
- Sudden cardiac death in a case of Crohn's disease with COVID-19: A case report
- Efficacy of propofol versus ketamine in modified electroconvulsive therapy: A prospective randomized control trial
- Comparison of impact of adjuvant treatment of midazolam, fentanyl, and magnesium sulfate with intrathecal bupivacaine on block characteristics and postoperative analgesia in knee arthroplasty: A randomized clinical trial
- Knowledge, attitude, and practice of house officers towards COVID-19: A multicentered crosssectional study in Egypt