Facilities for Centralized Isolation and Quarantine for the Observation and Treatment of Patients with COVID-19
2021-12-25XinlingWngJioWngJinShenJohnJiLijunPnHngLiuKngfengZhoLiLiBoYingLinFnLiuboZhngLinWngXiomingShi
Xinling Wng, Jio Wng, Jin Shen, John S. Ji, Lijun Pn, Hng Liu, Kngfeng Zho, Li Li,Bo Ying, Lin Fn, Liubo Zhng, Lin Wng, Xioming Shi,d,*
a China CDC Key Laboratory of Environment and Population Health, National Institute of Environmental Health, Chinese Center for Disease Control and Prevention, Beijing 100021,China
b Environmental Research Center, Duke Kunshan University, Kunshan 215316, China
c Nicholas School of the Environment, Duke University, Durham, NC 27708, USA
d Center for Global Health, School of Public Health, Nanjing Medical University, Nanjing 211166, China
Keywords:Centralized isolation Risk control Infectious patients Close contacts Coronavirus disease
ABSTRACT The coronavirus disease 2019 (COVID-19) pandemic increased the burden on many healthcare systems and in the process, exposed the need for medical resources and physical space. While few studies discussed the efficient utilization of medical resources and physical space so far.Therefore,this study aimed to summarize experiences related to facilities used for centralized isolation for medical observation and treatment during the COVID-19 pandemic in China and to provide suggestions to further improve the management of confirmed cases, suspected cases, and close contacts. In China, three types of facilities for centralized isolation (Fangcang shelter hospitals, refitted non-designated hospitals, and quarantine hotels) underwent retrofitting for the treatment and isolation of confirmed and suspected cases. These facilities mitigated the immediate high demand for space.Moreover,in order to minimize infection risks in these facilities, regulators and governmental agencies implemented new designs, management measures, and precautionary measures to minimize infection risk. Other countries and regions could refer to China’s experience in optimally allocating social resources in response to the COVID-19 pandemic.As a conclusion, government should allocate social resources and construct centralized isolation and quarantine facilities for an emergency response, health authorities should issue regulations for centralized isolation facilities and pay strict attention to the daily management of these facilities,a multidisciplinary administration team is required to support the daily operation of a centralized isolation facility,in-depth studies and international collaboration on the centralized isolation policy are encouraged.
1. Introduction
The current coronavirus disease 2019 (COVID-19) has rapidly spread across more than 200 countries[1].Severe acute respiratory syndrome coronavirus 2(SARS-CoV-2)can not only spread via respiratory droplets [2] but also persist on surfaces (including metal,glass,and plastic surfaces)for days,increasing the infection risk in confined places [3]. Since the World Health Organization (WHO)officially declared COVID-19 to be a pandemic, more than 128 million confirmed cases have been reported globally, with approximately 2.8 million deaths as of March 31,2021[1].In many nations, the COVID-19 pandemic was characterized by an exponential increase in confirmed cases, especially during the pandemic’s early phase [4,5]. Studies have reported that the case fatality rate(CFR)was 15%during the early stage of COVID-19 epidemic in Wuhan, China, in a small cohort of hospitalized patients and subsequently decreased to 1.4%,with an increase in confirmed cases in Wuhan [5,6]. However, poor survival rates were seen in elderly patients and those with respiratory diseases [5,7]. The medical staff estimated that approximately 60% of all infections originated from people considered to have mild symptoms or be asymptomatic [8]. According to a report from the WHO–China Joint Mission on COVID-19, 80% of the 55 924 COVID-19 patients in China exhibited mild-to-moderate syndromes [9]. However,there was neither an effective drug nor a vaccine available at that time, and thus, isolation became one of the essential preventive measures to curb COVID-19 transmission [10]. It is imperative to prevent the transmission of SARS-CoV-2 to healthy people via the isolation of confirmed and suspected cases and quarantining of their close contacts [11]. However, an unprecedented number of mild-to-moderate COVID-19 patients and close contacts were detected in a short period due to the rapid spread of COVID-19,exerting a continuous pressure on existing medical resources. In places such as Wuhan,Lombardy,and New York,all negative pressure wards became occupied due to a large number of mild-tomoderate COVID-19 patients, causing the increase in the CFR of severe cases [1,12,13]. In addition, general single medical rooms and individual isolation spaces were urgently needed for the isolation and screening of suspected cases and close contacts,respectively.
In this context, routine medical observation and treatment might not be possible during the pandemic due to their extensive burden on the medical system, especially in developing countries.To maximize healthcare service capacity during the pandemic,public health agencies need to establish a flexible management strategy for different patient groups. Centralized isolation means gathering people in one place and cutting off contact with outsiders. In our knowledge, this is the first systematic illustration of centralized isolation and quarantine for the observation and treatment of patients with COVID-19 in China from the perspectives of policy and public health. Therefore, this study aimed to summarize experiences related to facilities used for centralized isolation for medical observation and treatment during the COVID-19 pandemic in China and to provide suggestions to further improve the management of confirmed cases,suspected cases,and close contacts.
2. Centralized isolation strategy for controlling the COVID-19 infection risk
Effective centralized isolation is a reasonable countermeasure to slow down or stop COVID-19 transmission[14].The ideal places for isolation include hospitals and separate medical institutes. As early as the mid-1800s, infectious disease hospitals were utilized to isolate patients to interrupt disease transmission[15].In recent decades, the Chinese government has constructed and retrofitted centralized isolation facilities to respond to outbreaks of infectious diseases.For example,Chinese government built the Xiaotangshan Hospital for the temporary isolation and treatment of patients during the SARS epidemic in 2003 [16]; simple places for isolation,including empty schools, have been refitted for patients during the hepatitis A epidemic in Shanghai, China [17]. These practices imply that centralized isolation would be conducive to maintaining a functioning healthcare system using existing medical resources and ensuring timely and effective treatment for severe COVID-19 patients with a low CFR. In Wuhan, during the early stage of the COVID-19 pandemic, the isolation and treatment of patients with mild-to-moderate symptoms was a time-sensitive issue.The study by Chen et al. [18] showed that although social distancing for a finite time period could slow down transmission to some extent,it could not be expected to be sufficient for epidemic control without centralized isolation measures.Therefore,to overcome the severe shortage of available medical resources, several types of facilities were constructed or retrofitted, including Fangcang shelter hospitals, non-designated hospitals, and quarantine hotels, for the centralized isolation and quarantine of confirmed cases, suspected cases,and close contacts[19].It should be noted that Fangcang shelter hospitals are not temporary field hospitals but are places rapidly converted from existing public facilities to hospitals;they are used to simultaneously isolate and care for patients with mild-to-moderate COVID-19 [20]. The basic requirements related to environmental sanitation included a regular supply of drinking water and food, adequate number of temporary restrooms and bathrooms, and daily cleaning. The facilities used for centralized isolation were considered in terms of minimizing the infection risk to the surroundings and nearby residents.
3. Practices in facilities used for centralized isolation and quarantine during the COVID-19 pandemic
3.1. General design and implementation of the isolation and quarantine strategy
The rapid surge in the number of COVID-19 cases in Wuhan caused a rapid heavy burden on the capacity of centralized isolation.Resettlement buildings were used for the centralized isolation of many infectious cases and those who came into close contact with patients in emergency-room conditions. Since mild cases are reported to be the most infectious and it is difficult to determine the discharge date, the implementation of facility-based isolation plays an essential role in admitting all confirmed cases to hospitals and treating all patients in hospitals, which significantly improves the treatment rate [20–23]. The Wuhan Sports Center Stadium Fangcang Shelter Hospital started to admit patients and treat mild-to-moderate cases starting on February 12, 2020. The first group of eight patients recovered from the disease six days after admission. As of February 28, 2020, 479 cases had been admitted, with 49 cases discharged and 9 transferred. No deaths in patients and no infection in healthcare workers were reported.Only 37 days later, all Fangcang shelter hospitals in Wuhan were closed owing to complete reversal of the pandemic trend, which indicates the effectiveness of centralized isolation and quarantine in curbing the COVID-19 pandemic in China (Table 1).
All supplies were classified and managed in a centralized manner,and a worker was assigned to investigate the demand and supply status. Daily necessaries such as masks and slippers were provided to the patients on admission. The managing staff comprised well-trained healthcare responders with adequate knowledge regarding COVID-19, infection control, and protective measures.The occupant densities could be ranked from the highest to the lowest from Fangcang shelter hospitals to refitted nondesignated hospitals to quarantine hotels[24].Thus,the frequency of disinfection for the indoor environment could be adjusted according to need[25].Terminal disinfection of beds was restricted to specific rooms and carried out via spraying disinfection followed by ultraviolet disinfection.
3.2. Measures implemented within different facilities used for centralized isolation and quarantine
Since Fangcang shelter hospitals,non-designated hospitals,and quarantine hotels had different functions and conditions, the precaution measures for controlling infection risk varied accordingly.Some stadiums were retrofitted as facilities for centralized isolation,such as Fangcang shelter hospitals,for the isolation and treatment of confirmed patients with mild-to-moderate symptoms[19,26].Since all patients in Fangcang shelter hospitals were infectious,the indoor environment was contaminated with SARS-CoV-2.Thus, it was imperative to minimize the infection risks of doctors,nurses, and service personnel. To illustrate a case in point, some non-designated hospitals with simple infrastructure were retrofitted for the isolation and screening of suspected patients owing to limited capacity for polymerase chain reaction (PCR) diagnosis.Since suspected patients might be confirmed to have the disease,the prevention of inter-infection was emphasized by strictly limiting mobilization (suspected patients were requested to stay in separate rooms).Meanwhile,preparations were made with respect to simple medical treatment functions to cope with possible emergencies involving severe patients.In addition,simple modifications were made to some hotels that were not in proximity to other buildings for the quarantine of COVID-19 patients. In quarantine hotels,inter-infection was prevented by the use of separate rooms for quarantine or strict mobilization limitations.The design characteristics, management strategies, and precautionary measures in Fangcang shelter hospitals, refitted non-designated hospitals, and quarantine hotels are summarized in Table 2.
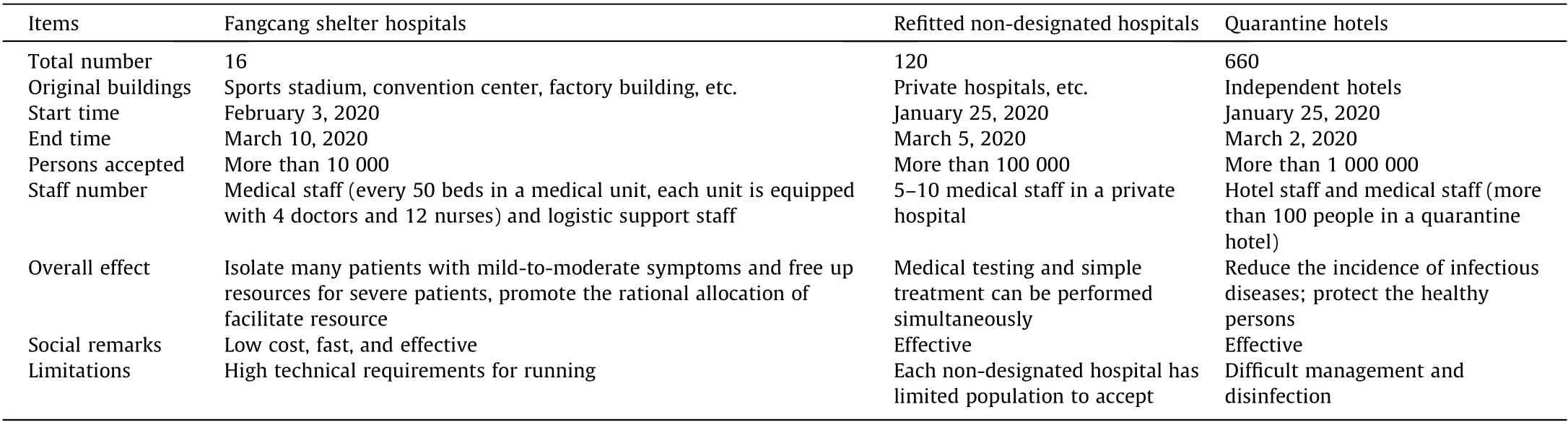
Table 1 Characteristics of Fangcang shelter hospitals, private hospitals, and quarantine hotels used to mitigate the COVID-19 pandemic in Wuhan.
It is vital to find a suitable site for building a Fangcang shelter hospital based on technical requirements similar to those for an infectious disease hospital. Inside the Fangcang shelter hospital,the contaminated zones included the places where patients were treated, such as wards, treatment rooms, waste rooms, and discharge rooms. The clean zones included dressing rooms, catering rooms, duty rooms, and storerooms [26]. Semi-contaminated zones referred to spaces between clean zones and contaminated zones,which could be potentially contaminated by patients’blood or body fluids; these zones included the medical staffs’ offices,treatment rooms, nurses’ stations, medical equipment rooms,other treatment rooms, and inner corridors. Two distinct passages were designed for healthy medical staff and infectious patients[19].Fangcang shelter hospitals in use were required to have three key characteristics:rapid construction,massive scale,and low cost.They were also required to have six essential functions: isolation,triage, basic medical care, frequent monitoring, rapid referral,and essential living and social engagement.These were considered to be powerful components of responses to the COVID-19 pandemic in Wuhan[19].Some non-designated hospitals and separate health centers with basic medical facilities were refitted for the emergency isolation and screening of suspected patients. These refitted hospitals for centralized isolation provided some essential functions such as frequent medical testing,separate isolation,basic medical care, rapid referral, and essential living conditions. In order to minimize the infection risk of medical staff because of frequent contact with cases,health status of medical staff in Fangcang shelter hospitals and refitted non-designated hospitals were monitored on a daily basis. The staff used personal protection equipment of a similar grade as that used in hospital settings.Goggles were soaked in disinfectant with an available chlorine content of 1000 mg∙L–1for one hour; then, they were washed and dried and disinfected again using ultraviolet light.
However,the medical treatment supply was not strongly necessary for quarantine hotels.In China,nearly 1 million close contacts were isolated in quarantine hotels [27,28]. It was imperative to ensure safety with respect to the indoor environment in these quarantine hotels by means of room ventilation and disinfection.Multi-room air conditioning systems were shut down to avoid possible inter-infections between different isolation spaces.The objective in such facilities for centralized isolation was the minimization of infection risk. The body temperature of people was recorded on entry. The close contacts and service personnel in quarantine hotels were monitored many times per day. Reverse transcription-polymerase chain reaction (RT-PCR) testing and screening were arranged for close contacts with body temperatures higher than 37.3°C.The local health department helped service personnel in these places to acquire skills related to risk control via education and professional training [29].
4. Discussion
Experiences in China revealed that centralized isolation could economically mitigate the COVID-19 pandemic by ensuring effective and timely isolation; treatment; and quarantine of confirmed cases,suspected cases,and close contacts.A differentiated prevention and control strategy was proposed, and the local government was responsible for formulating prevention and control measures according to the actual pandemic and socio-economic situations.In January 2020, the number of COVID-19 cases rose rapidly in Wuhan,China,causing a strain on medical institutions.Many confirmed and suspected cases could not be admitted and treated in time. Fig. 1 shows the temporal variation in the daily numbers of new confirmed cases from January 24 to March 16, 2020, in Wuhan.On February 2,the Wuhan COVID-19 Prevention and Control Headquarters announced that close contacts of patients with fever and patients with fever and pneumonia symptoms in Wuhan should be sent to facilities for centralized isolation for medical observation, treatment, and preventive measures. On February 5,the first Fangcang shelter hospital was put into service,and the last one was closed on March 10.Chen et al.[30]investigated the relationship between temperature and COVID-19 transmissibility in 117 countries and found that when keeping other environmental indicators equal, lower temperature increases the transmissibility of the virus, indicating higher demand of centralized isolation which efficiently curbs the virus transmission.Our finding is in line with those of their study that centralized isolation and quarantine is more important in winters [30]. Fangcang shelter hospitals provided better medical facilities for the treatment of patients with mild-to-moderate symptoms who showed progression to severe COVID-19,which was crucial for decreasing the CFR.The screening and isolation of suspected cases and quarantine of close contacts as early as possible could be used to avoid cluster infection amongfamily members and subsequent transmission in the community.Fig. 1 shows that only two days after announcing close contacts of patients with fever and patients with fever and pneumonia symptoms in Wuhan should be sent to facilities for centralized isolation for medical observation, treatment, and preventive measures, the rapid increase in cases since January 24 was ameliorated, and the number of new confirmed cases began to drop with occasional fluctuations. The statistical caliber was adjusted on February 12, which indicates that after this date,clinically diagnosed cases without PCR confirmation were also reported as confirmed cases. To better demonstrate the variation in the trend of confirmed cases, the data on February 12 (13 436 cases)were not shown in the graph.However,the absolute number of confirmed cases could not be directly compared before and after adjustment of the statistical caliber. The variation trends both demonstrated an overall decrease. Thus, it is reasonable to infer that centralized isolation and quarantine in these places was conducive to interrupting the rapid spread of COVID-19 owing to optimal allocation of resources in local areas. Moreover, facility-based isolation of mild cases was a cost-effective approach because it could efficiently curb the pandemic and minimize economic burden[31]. However,it should be pointed out that centralized isolation and quarantine policy was only one of the factors contributing to the change in the curve. Other factors might include change of meteorological and environmental factors, intervening measures,improvement of public compliance to precautions, and so on.

Table 2 Design characteristics, management strategies, and precautionary measures in Fangcang shelter hospitals, refitted non-designated hospitals, and quarantine hotels.
However, the centralized isolation and quarantine policy also has disadvantages. The limitations of centralized isolation include separation from family members, restriction of activities, high medical requirements,and psychological problems associated with isolation (such as anxiety and depression). Thus, to avoid possible limitations, further improvements are needed in the management of these centralized isolation and quarantine facilities, such as the provision of psychological counseling.Moreover,decentralized isolation and quarantine, such as stay-at-home-orders and at-home quarantining,might also serve as an alternative measure.Although the isolation of confirmed and suspected cases at home might result in family clusters and instances of second-generation community transmission [32,33], decentralized isolation and quarantine can be an alternative for suspected patients with mild symptoms, close contacts, people entering the region from medium- and high-risk areas, and people who need to be isolated in specific circumstances as required by the local health department. Therefore, while emphasizing measures for centralized isolation and quarantine, it is also necessary to pay attention to the decentralized isolation and quarantine policy. Moreover,religious beliefs and local cultural traditions should be respected in the routine management of centralized isolation and quaratine facilities (setting up prayer rooms and multiple choices for food).Mobility assistance and special needs should also be considered for individuals with disabilities.As to the minimization of infection risk in centralized isolation and quarantine facilities, further studies are needed to improve function and precautionary measures. Unfortunately, the data about the number of confirmed cases in the centralized isolation and quarantine places could not be obtained due to limited data access,which becomes a limitation of this study.However,with the improvement of data accessibility,once the national and international data become available, indepth quantitative studies on the role of centralized isolation policy in the prevention and control of COVID-19 could be carried out.

Fig.1. Temporal variation in the daily number of new confirmed cases from January 24 to March 16,2020,in Wuhan,China.The red dashed line refers to the release of the 10th announcement from the Wuhan COVID-19 Prevention and Control Headquarters (February 2, 2020), and the black dot line refers to the date of adjustment of the statistical caliber (February 12, 2020).
5. Perspectives
At present, the COVID-19 pandemic is ongoing in many countries, and centralized isolation has become a valuable strategy for the isolation and treatment of infectious cases in some nations.To curb the global spread of COVID-19,we recommend the following actions.
First, all countries should collaborate and address the threat of the COVID-19 pandemic and develop appropriate preventive strategies for the effective isolation of infectious cases. Because of the diversity in economic growth, social development, and historical background, it would be valuable for international health organizations such as the WHO to discuss principles regarding the designing and legal aspects of such facilities; issue technical standards [1]; and encourage stakeholders, social organizations,and enterprises to participate in the prevention of COVID-19.
Second, it should be the government’s goal to allocate social resources and construct centralized isolation and quarantine facilities for an emergency response.Due to the diversity in hospitals and hotels in different countries,practical local construction or retrofitting plans should be taken into consideration.
Third,health authorities should issue regulations for centralized isolation and quarantine facilities and pay strict attention to the daily management of these facilities. Secondary infection must be prevented, and adequate sanitation should be guaranteed with environmental health surveillance and health risk evaluation.
Fourth, a multidisciplinary administration team is required to support the daily operation of a centralized isolation facility. The team should be composed of doctors, nurses, environmental hygiene staff, and support personnel. Some workers may not have training and experience regarding personal protection against infectious diseases.Thus,health education and specialized training should be conducted for all members.Moreover,it is also essential to improve the compliance to prevention and control strategy of people living in centralized isolation facilities in terms of reducing infection risk by emphasizing the importance and benefits of preventive measures.
Fifth, in-depth studies on the centralized isolation and quarantine policy are encouraged.It is necessary to accumulate comparative experience both across countries and across various means of achieving different isolation and quarantine strategies. An open data platform should be constructed for further in-depth quantitative studies on the role of centralized isolation and quarantine in the prevention and control of COVID-19. Moreover, costeffectiveness studies are needed to identify measures that are critical for successful isolation and quarantine at minimal economic and health costs.
Authors’ contribution
Xiaoming Shi, Xianliang Wang, and Jiao Wang had the idea for and designed the study. Xianliang Wang, Jiao Wang, Jin Shen, and Xiaoming Shi drafted the paper. All authors critically revised the manuscript and gave final approval for the version to be published. Hang Liu, Li Li, Bo Ying, and Lin Fan produced field materials. John S. Ji, Lijun Pan, Kangfeng Zhao, and Liubo Zhang discussed the experience. All authors agree to be accountable for all aspects of the work in ensuring that questions related to any part of the work are appropriately investigated and resolved.
Compliance with ethics guidelines
Xianliang Wang, Jiao Wang, Jin Shen, John S. Ji, Lijun Pan, Hang Liu, Kangfeng Zhao, Li Li, Bo Ying, Lin Fan, Liubo Zhang, Lin Wang,and Xiaoming Shi declare that they have no conflict of interest or financial conflicts to disclose.
杂志排行
Engineering的其它文章
- COVID-19 Vaccine Allocation: Modeling Health Outcomes and Equity Implications of Alternative Strategies
- Quantitative Investigation of Tomographic Effects in Abnormal Regions of Complex Structures
- Fast Marching Method for Microseismic Source Location in Cavern-Containing Rockmass: Performance Analysis and Engineering Application
- Non-Communicable Diseases During the COVID-19 Pandemic and Beyond
- Next Steps for Efficacy Evaluation in Clinical Trials of COVID-19 Vaccines
- Temporal Profiles of Antibody Responses, Cytokines, and Survival of COVID-19 Patients: A Retrospective Cohort