Autosomal recessive 333 base pair interleukin 10 receptor alpha subunit deletion in very early-onset inflammatory bowel disease
2021-12-06JiaJiaLvWenSuXiaoYanChenYiYuXuXuChunDiXuXingDengJieBinHuangXinQiongWangYuanXiao
Jia-Jia Lv, Wen Su, Xiao-Yan Chen, Yi Yu, Xu Xu, Chun-Di Xu, Xing Deng, Jie-Bin Huang, Xin-Qiong Wang,Yuan Xiao
Abstract
Key Words: Interleukin 10 receptor alpha subunit mutation; Very early-onset inflammatory bowel disease; Whole-genome sequencing; Immunodeficiency; Crohn’s disease; Wholeexon sequencing
INTRODUCTION
Inflammatory bowel disease (IBD) in children < 6 years of age is known as very earlyonset IBD (VEO-IBD)[1 ] and represents a specific disease course with a distinct phenotype that can be more severe and refractory than classic IBD[2 -3 ]. Recent studies suggested that patients with VEO-IBD, particularly those with symptoms such as perianal disease soon after birth, suffer from failed treatment, indicating a monogenic type of disease[4 -6 ].
By utilizing next-generation sequencing (NGS), many genetic disorders associated with epithelial defects or immunodeficiencies have been found in patients[7 -9 ].Notably, interleukin 10 receptor alpha subunit (IL10 RA) dysfunction is the most common cause of the disease in East Asians, particularly in the Chinese, Japanese, and Korean populations[10 -12 ].
According to our previous retrospective study, increased serum ferritin levels in VEO-IBD patients are indicative of monogenic disease, and very high serum levels of IL-10 suggest that patients with VEO-IBD are more likely to have IL10RAmutations[13 ].
We report four cases clinically diagnosed with VEO-Crohn's disease with high serum IL-10 levels, indicating IL10RAdysfunction. However, neither results of targeted gene panel sequencing (TGPS) nor those of whole-exome sequencing (WES)in the probands were conclusive. Whole-genome sequencing (WGS) was performed in two patients, and a novel 333 -bp deletion in IL10RAwas identified. The results of trio-WES for the other two patients were subsequently reanalyzed, and the same novel 333 -bp deletion was found.
MATERIALS AND METHODS
Patients
Four patients with VEO-IBD, including two boys and two girls, were enrolled in our study. The medical history and clinical characteristics of the patients are summarized in Table 1 . All patients were of Chinese Han ethnicity and were born to parents who were non-consanguineous, presented disease at the age of less than 1 year (range: 11 d to 8 mo), and experienced severe diarrhea with fistulas in the perianal region; blood samples were collected from three healthy volunteers.
Written informed consent was obtained from the parents of the four patients who participated in the study. This study was approved by the Institutional Review Board of Ruijin Hospital, Shanghai Jiao Tong University School of Medicine (No. 2019 -15 ).
养殖生产实践证明,青虾与小龙虾混养是可行的。在饲养期间要注意以下的问题:①要合理控制青虾与小龙虾的放养密度,密度过大时小龙虾可能摄食青虾,青虾也可以摄食小龙虾。②混养池塘水体的溶解氧应当保持在5.0mg/L以上,最低也不能低于3.0mg/L。③要保证充足的饲料供应,以防青虾与小龙虾之间,或青虾内部间,或小龙虾内部间相互残杀。④青虾与小龙虾一旦达到商品规格,即捕捞出售。
Whole-genome sequencing
Sample preparation and WGS were carried out by Beijing Berry Genomics Co., Ltd.(Beijing, China). The quality of the isolated genomic DNA was verified using the following two methods: (1 ) DNA degradation and contamination were monitored by electrophoresis on 1 % agarose gels; and (2 ) DNA concentration was measured using the Qubit DNA Assay Kit and Qubit 2 .0 Fluorometer (Life Technologies, Carlsbad, CA,United States).
A total of 1 μg DNA per sample was used as the input material for DNA library preparation. The DNA sequencing library was generated using the CLEANNGS DNA kit following the manufacturer’s recommendations, and indexing codes were added to each sample. Briefly, genomic DNA samples were enzymatically disrupted to a size of 350 bp. The DNA fragments were then end-polished, a-tailed, and ligated with a fulllength adapter for Illumina sequencing, followed by further polymerase chain reaction(PCR) amplification. After the PCR products were purified (AMPure XP system,Beckman, Brea, CA, United States), libraries were analyzed to determine theirsize distribution using an Agilent 2100 Bioanalyzer (Santa Clara, CA, United States) and quantified by qPCR.
Clustering of the index-coded samples was performed on a cBot Cluster Generation System using the NovaSeq 5000 /6000 S4 Reagent Kit (Illumina, San Diego, CA, United States) according to the manufacturer’s instructions. After cluster generation, the DNA libraries were sequenced on an Illumina NovaSeq 6000 platform, and 150 -bp pairedend reads were generated.
The pathogenicity of all mutations was further evaluated according to the American College of Medical Genetics and Genomics guidelines.
Isolation and stimulation of peripheral blood mononuclear cells
Peripheral blood mononuclear cells (PBMCs) were isolated according to a previous study, with minor modifications[14 ]. Briefly, blood was drawn from patient D and healthy controls by standard venipuncture in our pediatric ward and collected into a tube containing ethylenediamine tetraacetic acid. Blood (4 mL) was diluted 1 :1 with sterile RPMI 1640 medium (Hyclone, Logan, UT, United States) at room temperature(RT) and carefully dropped into a 15 -mL tube (Corning, Inc., Corning, NY, United States) containing 4 mL Ficoll-Paque Plus (GE Healthcare, Little Chalfont, United Kingdom). Notably, diluted blood was present on the surface of the Ficoll gradient.The 15 -mL tube was centrifuged at 800 × g at RT for 20 min (brake off), after which the buffy coat was carefully aspirated and transferred to another sterile 15 -mL tube. After washing the cells with 5 mL RPMI 1640 medium three times by centrifugation at 400 ×g for 15 min at RT, most of the supernatant, as much as possible, was pipetted off.
Cells were aspirated with complete RPMI 1640 (10 % fetal bovine serum and 1 %penicillin-streptomycin) and cultured in 6 -well plates at a density of 2 × 106 cells/well.Four groups of PBMCs from patients or healthy controls were established as follows:Unstimulated phosphate buffered saline (PBS), lipopolysaccharide (LPS) (100 ng/mL),LPS (100 ng/mL) + IL-10 (20 ng/mL), and IL-10 (20 ng/mL)[15 ]. Cells were cultured in the indicated milieu for 12 h at 37 °C. Proteins in PBS-, LPS-, and IL-10 -stimulated PBMCs were collected in radioimmunoprecipitation assay buffer containing protease and phosphatase inhibitors for western blot analysis. The supernatants of the PBS-,LPS-, and LPS + IL-10 -stimulated PBMCs were collected to determine tumor necrosis factor-α (TNF-α) level.
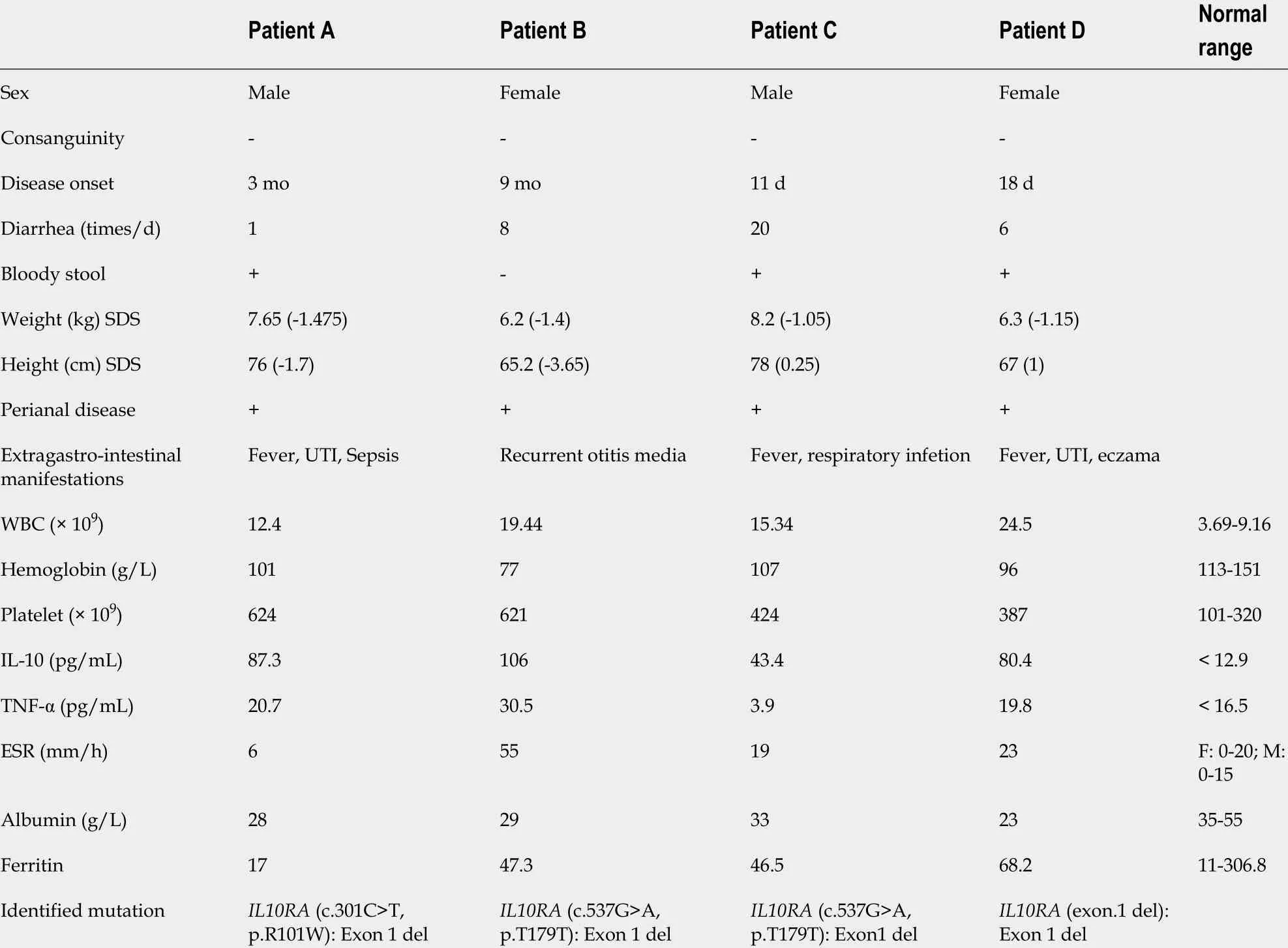
Table 1 Clinical and laboratory characteristics of patients
Western blot analysis
Western blotting was performed as described previously[16 ]. Polyvinylidene fluoride membranes were blotted with monoclonal antibodies against phos-signal transducer and activator of transcription 3 (STAT3 ) (Tyr705 ), phos-STAT3 (Ser727 ), STAT3 (Cell Signaling Technology, Danvers, MA, United States), and glyceraldehyde-3 -phosphate dehydrogenase (Servicebio, Wuhan, China). Horseradish peroxidase-conjugated antimouse and anti-rabbit (Cell Signaling Technology) secondary antibodies were detected using a chemiluinescent substrate (Millipore, Billerica, MA, United States). Images were captured using an automatic chemiluminescence image analysis system (Tanon,Shanghai, China).
Enzyme-linked immunosorbent assay
The supernatant of PBMCs after stimulation with PBS, LPS or LPS + IL-10 was collected. IL-10 and TNF-α levels were determined using sandwich ELISA kits(DAKEWE, Shenzhen, China) according to the manufacturer’s instructions.
Statistical analysis
Continuous variables are presented as the mean ± SEM, and the unpaired two-tailed Student’st-test or analysis of variance was used to compare the differences between groups as appropriate. Bonferroni correction was used for pairwise comparisons(GraphPad Prism v.5 .0 software; GraphPad, Inc., La Jolla, CA, United States). Statistical significance was set atP< 0 .05 .
RESULTS
Clinical characteristics of four patients with VEO-IBD
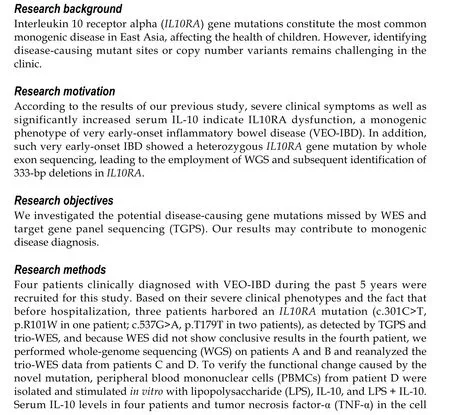
All four patients had severe diarrhea (> 6 times/d) and hematochezia during the first year of life. Patients C and D suffered from the disease during the newborn period. In addition to gastrointestinal symptoms, all cases exhibited extraintestinal manifestations, such as perianal abscesses, skin tags (Figure 1 A), rectoperineal fistula, failure to thrive, recurrent otitis, urinary tract or respiratory infection, folliculitis, and even sepsis (Table 1 ). Elevated numbers of peripheral white blood cells and platelets and decreased hemoglobin and albumin levels were found in each patient. Remarkably,immune-related investigations showed that all patients had high serum levels of IL-10 (Table 1 ). All patients underwent colonoscopy and intestinal biopsy under general anesthesia, revealing erosive lesions (Figure 1 B), and were diagnosed with Crohn’s disease.
Identification of a novel compound heterozygous mutation in IL1 0 RA
Before admission, all patients underwent TGPS or trio-WES. Two heterozygous pathogenic variants ofIL10 RA were detected in three patients (patient A: c.301 C>T,p.R101 W; patients B and C: c.537 G>A, p.T179 T) (Figure 1 C and Supplementary Figures 1 and 2 ). Mutation of c.537 G>A occurred at the exon-intron boundary of exon 4 , which is a variant hotspot and disrupts RNA splicing (Figure 2 A). No pathogenic or likely pathogenic variants were found in patient D.
AsIL10RAmutation causes infantile IBD in an autosomal recessive manner and serum levels of IL-10 were very high in the four infantile patients with IBD, which is a valuable clinical indicator for identifying infantile IBD as a monogenic disease as we demonstrated previously[13 ], we suspected that mutations had been overlooked in WES owing to the techniques’ limitations. After performing WGS in patients A and B,the breakpoints of the novel deletion were identified by manual review and correction.The deletion was located at chr11 :117857030 upstream of exon 1 and chr11 :117857362 in intron 1 , which contains the 5 ′-untranslated region (UTR), all of exon 1 , and part of intron 1 in IL10 RA (Figure 1 D and Figure 2 B). PCR revealed a paternally-inherited 333 -bp deletion in addition to the point mutations mentioned above (Figure 1 E). The deletion and point mutations were inherited from both parents and eventually constituted compound heterozygotes in patients B (Figure 1 F) and A (Supplementary Figure 1 ).
After identifying the 333 -bp deletion in the gene in patients A and B, we reanalyzed the trio-WES data for patients C and D, specifically in the region from 117857030 and 117857362 on chromosome 11 and detected the same deletion. Patient C was a compound heterozygous carrier for c.537 G>A, p.T179 T (maternal), and the 333 -bp deletion (paternal) (Supplementary Figure 2 ), and patient D was homozygous for the 333 -bp deletion.
Histological and functional analysis of patient DIL1 0 RA deletion
Histological findings in a specimen from the colon obtained during colonoscopy revealed oval-shaped intramural abscesses in the submucosa (Figure 3 A). Figure 3 B shows a higher magnification of inset 1 in Figure 3 A, depicting intramural microabscesses.
To determine whether the novel 333 -bp deletion in IL10 RA caused IL-10 R dysfunction and subsequently inhibited TNF-α production, supernatants of cultured PBMCs were collected and used to determine TNF-α levels. In healthy controls, LPS stimulation caused a remarkable increase in TNF-α production, whereas addition of IL-10 significantly decreased its abundance. Although LPS led to increased TNF-α production in patient D, this phenomenon was not reversed by the addition of IL-10 ,as observed in the healthy controls (Figure 3 C).
To clarify the exact mechanisms involved, PBMCs were isolated from patient D because the patient was homozygous for theIL10RAdeletion. PBMCs were stimulated with LPS in the presence or absence of IL-10 . The results of western blot analysis showed that in PBMCs from healthy controls, both LPS and IL-10 stimulation caused an increase in the phosphorylation of STAT3 at Tyr705 but not at Ser727 (Figure 3 D).In PBMCs from patient D, LPS stimulation also induced increased phosphorylation of STAT3 at Tyr705 but not at Ser727 . However, IL-10 stimulation failed to significantly increase phosphorylation of STAT3 at Tyr705 in PBMCs of patient D compared with that in PBS-stimulated PBMCs. No significant differences in STAT3 phosphorylation at Ser727 were observed among the PBS-, LPS-, and IL-10 -stimulated PBMCs from patient D (Figure 3 D).
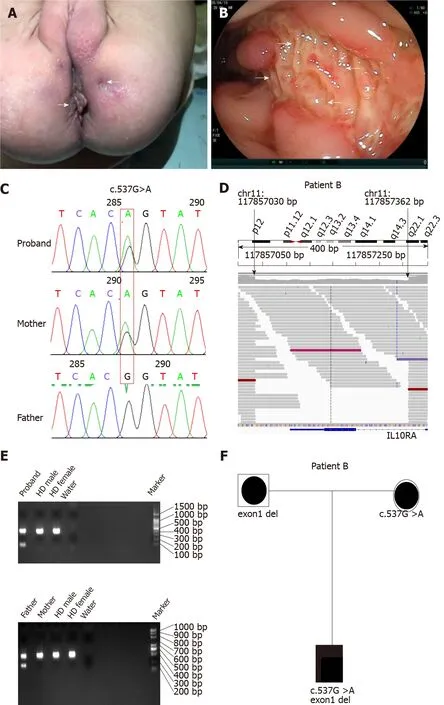
Figure 1 Identification of a novel 333 -bp deletion spanning interleukin 10 receptor alpha subunit exon1 . A: Perianal skin tag; B: Endoscopic image of ulcerations; C: Sanger DNA sequencing verified a compound heterozygous variant (c.537 G>A) inherited from the mother in patient B; D: Whole-genome sequencing (WGS) data showing sequencing read pairs at breakpoints chr:117857030 and chr:117857362 of interleukin 10 receptor alpha subunit (IL10 RA); E:Polymerase chain reaction validated the heterozygous deletion of 333 bp spanning exon1 inherited from the father; F: WGS revealed compound heterozygous variants of IL1 0 RA in patient B with very early-onset inflammatory bowel disease. bp: Base pair; HD: Healthy donor.
DISCUSSION
VEO-IBD is challenging to diagnose and treat because the patients are critically ill and exhibit numerous potential mono-genic defects. Approximately 56 Mendelian genetic defects that can lead to IBD-like colitis have been identified, some of which show almost 100 % penetrance, such as defects in IL-10 , IL10 RA, IL10 RB, FoxP3 , and XIAP[1 ].NGS has led to breakthroughs in the diagnosis of genetic diseases, including monogenic VEO-IBD. According to a recent single-center study performed by Crowleyet al[17 ], 7 .8 % of VEO-IBD (141 patients) and 13 .8 % of infantile-onset IBD (29 patients)cases had rare variations associated with monogenic genes. This prevalence was lower than that reported in Chinese or European studies, which was approximately 31 .9 %-45 .2 %[12 ,18 ]. In our center, we found that 60 .3 % of patients with infant-onset IBD had monogenic disease, with mutations inIL10RAidentified as the most common defect[13 ].
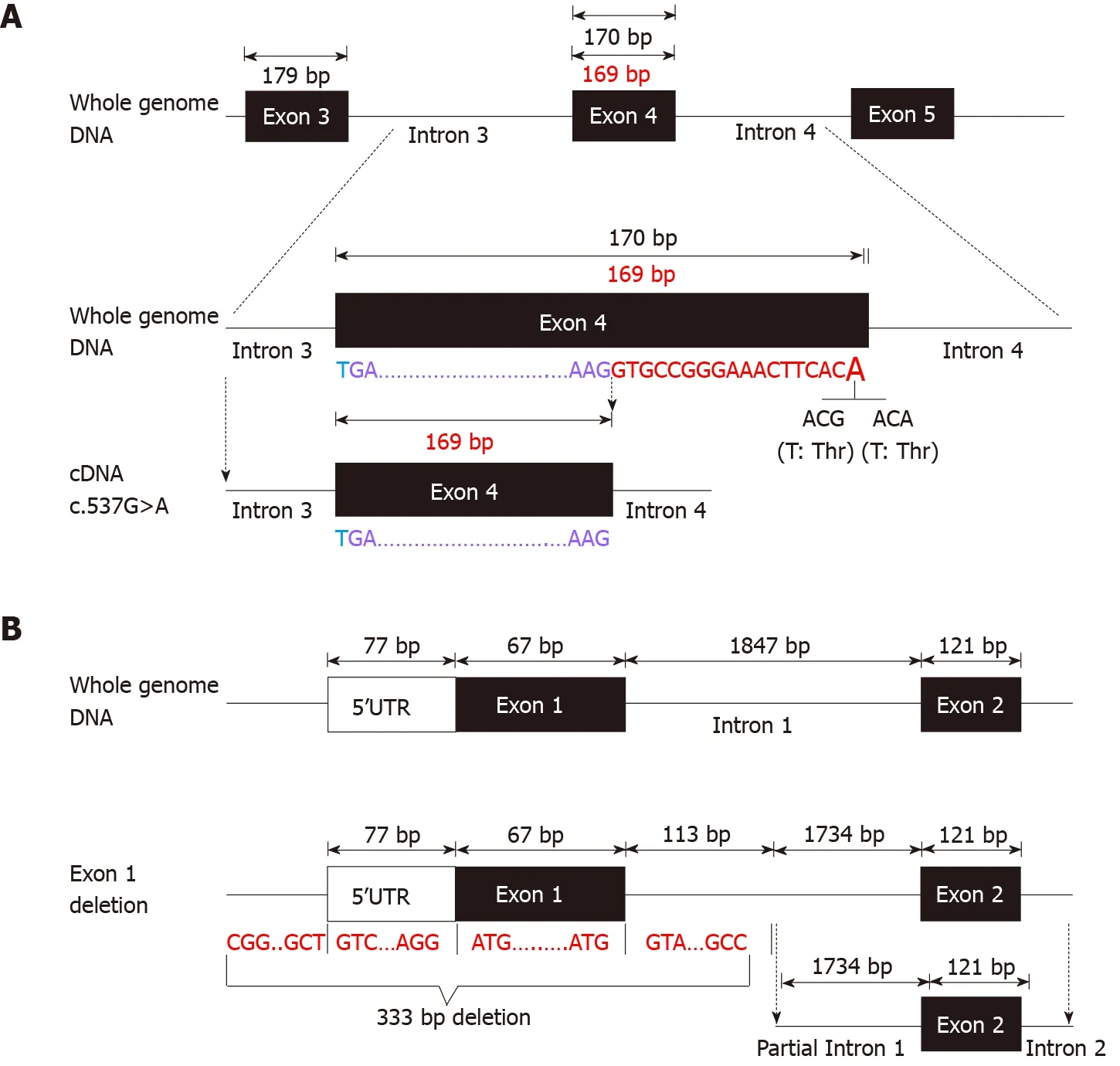
Figure 2 Schematic diagram of disrupted RNA splicing and 333 -bp deletion in interleukin 10 receptor alpha subunit. A: Schematic diagram of disrupted splicing caused by c.537 G>A in interleukin 10 receptor alpha subunit (IL10 RA) between the boundary of exon4 and intron4 ; B: Schematic diagram of IL1 0 RA 333 -bp deletion. bp: Base pair.
We evaluated four patients who had Crohn’s disease from early infancy and exhibited failure to thrive, severe perianal disease, and resistance to medication. These characteristics indicate the presence of underlying genetic conditions[7 ]. Although the patients underwent NGS in a local hospital, neither TGPS nor WES revealed conclusive results. However, all patients showed very high serum IL-10 levels, and three patients had a disease-causing heterozygous mutation inIL10RA. According to our previous research, serum IL-10 levels > 33 .05 pg/mL in patients with VEO-IBD strongly indicates the presence of IL10 RA dysfunction[13 ]. Thus, we predicted that additionalIL10RAmutations were missed during TGPS or WES. We did not detect the 333 -bp deletion in IL10RAin two patients until WGS was performed. We then analyzed the same deletion in the other two patients by reanalyzing the trio-WES data.Finally, all patients were precisely diagnosed with VEO-IBD owing to compound heterozygous mutations inIL10RAin three patients and homozygous deletion involvingIL10RAin one patient.
NGS, including TGPS and WES, is a powerful tool for identifying Mendelian genetic diseases in patients with VEO-IBD. The position paper on VEO-IBD by NASPGHAN/ESPGHAN suggests that NGS combined with the patient clinical history represents a vital component of the diagnostic approach[1 ]. A previous multicenter study showed that molecular diagnosis was achieved in 32 % of patients with VEO-IBD when NGS was employed[18 ]. However, clinical NGS applications have limitations such as short read lengths, relatively high error rates, and incomplete coverage. Non-coding, yet potentially functional regions, and approximately 5 % of exons are poorly covered in WES[19 ]. It is difficult to detect variants involving extensive deletions/insertions or short tandem repeats[20 ]. Charbit-Henrion et al[18 ]reported three WES-negative cases harboring large deletions inLRBAandNCF1.Compared to WES, WGS can detect all single-nucleotide variants, small indels, large indels, and copy number variants. In our cases, the 333 -bp IL10RAdeletion contained a 5 ′-UTR, exon 1 , and part of intron 1 . This large deletion was easy to overlook when WES was used because of its technical limitations and insufficient bioinformatics analysis. After detecting this deletion, we requested re-analysis of the WES data for patients C and D, specifically for the 333 -bp region spanning IL10 RA exon 1 . As expected, these two patients harbored the deletion. These results indicate that WES can detect the 333 -bp deletion, which was easily overlooked in bioinformatics analysis because of algorithm defects and insufficient experience. WGS compensates for the limitations of WES. Our results indicated that WGS should be performed in VEO-IBD cases with negative WES results, particularly in those with infantile-onset IBD and treatment failure.
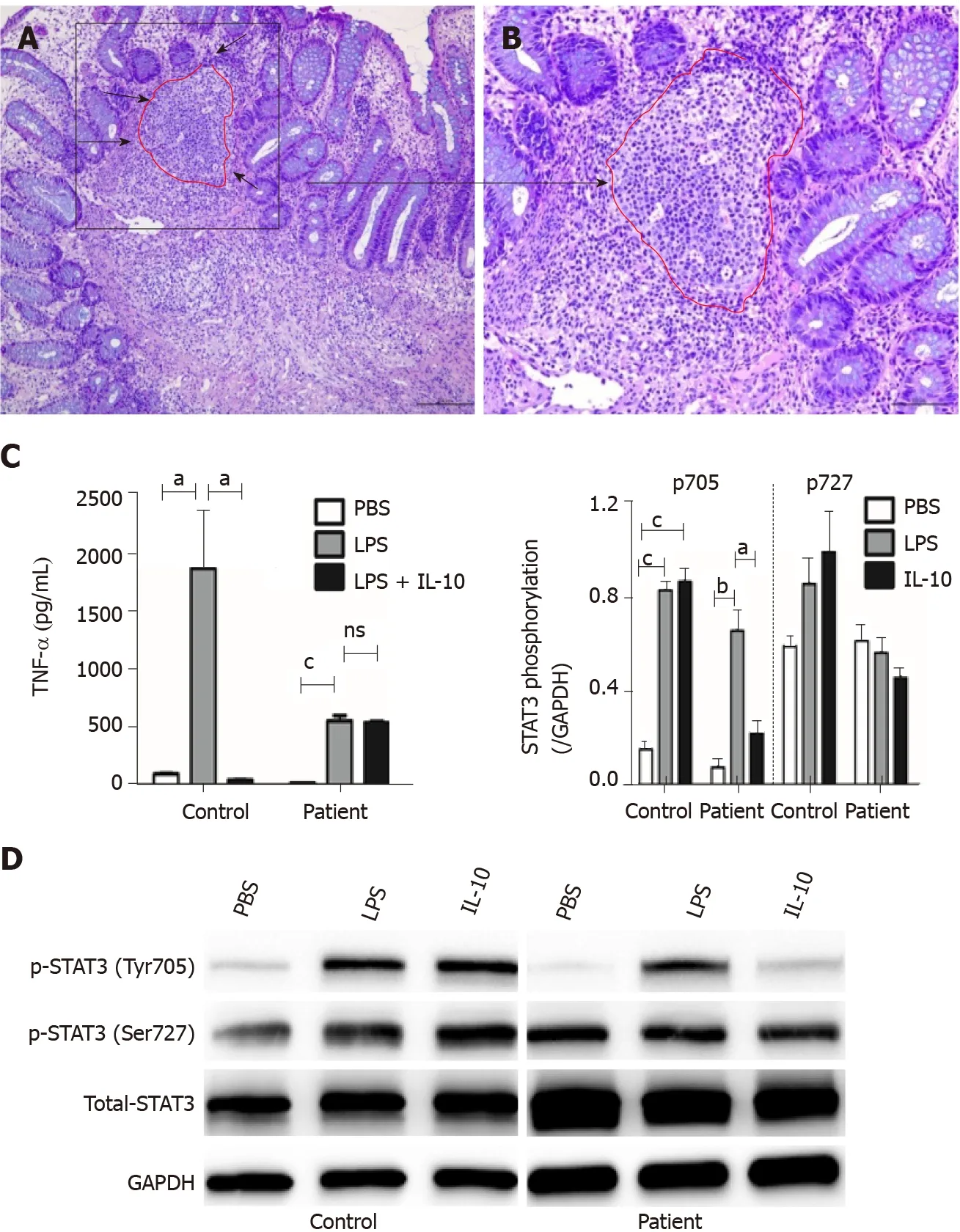
Figure 3 Histopathochemistry and functional results of homozygous interleukin 10 receptor alpha subunit mutation. A: Histological findings in a colonic specimen obtained during colonoscopy showing oval-shaped intramural abscesses; B: Higher magnification of inset A; C: Determination of TNF-α levels in the supernatant of cultured PBMCs from patient D after stimulation with PBS, LPS, or LPS + IL-10 in vitro; D: Western blot results of PBMCs isolated from patient D after stimulation with LPS or IL-10 . Phosphorylation of STAT3 at Tyr705 and Ser727 and total STAT3 protein were detected (n = 3 ). aP < 0 .05 , bP < 0 .01 , and cP <0 .001 were considered as statistically different.
A comprehensive range of defects may be associated with VEO-IBD. It is difficult to differentiate every patient based on these defects and their underlying genetic disorders. A small number of patients show distinct phenotypes associated with specific functions, such as IL-10 /IL-10 R defects, IPEX, CGD, and XIAP[1 ]. IL10RAmutation-induced VEO-IBD shows specific characteristics such as refractory pancolitis, perianal defects, fistulas, and growth failure, which occur during the neonatal period. An assay that can detect the lack of IL-10 inhibition in LPS can confirm receptor mutations[1 ]. Nevertheless, this assay is complicated and not routinely available in most hospitals in China. In a retrospective study, we found that the assay was useful for diagnosing IL10 RA defects when the serum level of IL-10 was > 33 .05 pg/mL. The assay sensitivity was very close to 100 %, and the specificity was approximately 84 %[13 ]. Elevated serum levels of IL-10 in patients with VEO-IBD indicated that even such high level of IL-10 could not inhibit TNF-α release and alleviate inflammation. Thus, serum IL-10 level may be a substitute for determining IL-10 inhibition in LPS functional testing. Therefore, when classic symptoms and laboratory results indicate that patients may have IL-10 /IL-10 R dysfunction but WES is inconclusive,IL-10 /IL10 RA/IL-10RBmust be investigated and analyzed. It is recommended to use WGS or specific PCR to detect whether a large deletion involving these genes has occurred.
Interestingly, TNF-α production in LPS-stimulated PBMCs was not as robust in patient D as in control subjects; in our study, patient D was administered with anti-TNF-α antibody (Infliximab) before blood collection, which may have led to relatively low TNF-α production in the supernatant of LPS-stimulated PBMCs compared to that in healthy controls. Another possible reason is that increased TNF-α in the blood of patient D led to activation of the TNF-α receptor, resulting in JNK signaling-dependent inhibition of Bcl-2 expression, which acts as a major anti-apoptosis protein[21 ].The lack of a comprehensive functional test forIL10RAmutation is the major limitation of our study, although we conducted western blotting to determine the possible mechanism ofIL10 RA mutation-induced dysfunction of IL10 RA signaling. Further studies are needed to explore other potential differences in IL10 RA signaling.
CONCLUSION
Using WGS, we identified a novel 333 -bp deletion in IL10RAthat contributed to four cases of clinically diagnosed VEO-IBD with inconclusiveIL10RAmutations. Most importantly, we confirmed that typical clinical manifestations and increased serum levels of IL-10 strongly indicate the existence of IL-10 R dysfunction even when WES results are negative.
ARTICLE HIGHLIGHTS

Research results
Results of WGS revealed a novel 333 -bp deletion encompassing exon 1 of IL10RAin patients A and B, which was also found in patients C and D after reanalyzing their WES data. Patient D was homozygous for the 333 -bp deletion. All four patients showed elevated serum IL-10 levels. In vitro, IL-10 -stimulated PBMCs from patient D failed to induce STAT3 phosphorylation at Tyr705 and minimally suppressed TNF-α production induced by LPS. Phosphorylation at Ser727 in PBMCs was not affected by LPS or LPS + IL-10 in both healthy subjects and patient D.
Research conclusions
Genome-wide uniformity of coverage of WGS identified a novel 333 -bp deletion inIL10RAin four patients with VEO-IBD, whereas the results of initially performed WES were inconclusive. WGS, which was more informative than WES, is the most important comprehensive second-tier genomic test for monogenic diseases in the clinic.
Research perspectives
We will customize a multiplex ligation-dependent amplification probe of the 333 -bp deletion inIL10 RA to help diagnose IL10RAmutation-related monogenic diseases.
ACKNOWLEDGEMENTS
The authors would like to thank the members of the Department of Pediatrics and Pediatric Laboratory.
猜你喜欢
杂志排行

World Journal of Gastroenterology的其它文章
- Proton pump inhibitors and colorectal cancer: A systematic review
- Orexins: A promising target to digestive cancers, inflammation, obesity and metabolism dysfunctions
- Calycosin attenuates severe acute pancreatitis-associated acute lung injury by curtailing high mobility group box 1 - induced inflammation
- Prediction of genetic alterations from gastric cancer histopathology images using a fully automated deep learning approach
- Endoscopic management of difficult common bile duct stones: Where are we now? A comprehensive review
- Role of early transjugular intrahepatic portosystemic stent-shunt in acute variceal bleeding: An update of the evidence and future directions