Clinical efficacy observation of acupoint threadembedding in treating obese patients with food addiction
2021-06-22JiLingling吉玲玲OuyangBasi欧阳八四ShenJie沈洁LuoYing罗莹JiangYawen蒋亚文AiBingwei艾炳蔚
Ji Ling-ling (吉玲玲), Ouyang Ba-si (欧阳八四), Shen Jie (沈洁), Luo Ying (罗莹), Jiang Ya-wen (蒋亚文),Ai Bing-wei (艾炳蔚)
1 Suzhou TCM Hospital Affiliated to Nanjing University of Chinese Medicine, Suzhou 215000, China
2 Suzhou Academy of Wumen Chinese Medicine, Suzhou 215000, China
3 Nanjing University of Chinese Medicine, Nanjing 210000, China
4 Jiangsu Province Hospital of Chinese Medicine, Nanjing 210000, China
Abstract Objective: To observe the effects of acupoint thread-embedding therapy and low-carbohydrate diet therapy on obese patients with food addiction.
Keywords: Acupoint Therapy; Embedding Therapy; Obesity; Food Addiction; Yale Food Addiction Scale; Randomized Controlled Trial
As a main factor affecting people’s health, obesity has become the most concerned public health issue worldwide. Given normal blood pressure, blood glucose and cholesterol levels, the risk of developing coronary heart disease increases by 26.0% and 28.0%, respectively,in overweight and obese people compared with those estimated as normal body mass (BM)[1]. The dangers are self-evident. Up to 2012, 2/3 of the American population were obese or overweight[2]. By 2015, the incidence of obesity had hit 11.9% in China and the overweight rate had reached 30.1%[3]. With the change in people’s diet pattern, the increased consumption of prepared starch,sugar and high fat foods is considered highly linked with the high incidence of obesity[4]. It has been wellrecognized that overeating is the root causing this obese epidemic. In addition, most of the obese patients reportedly present with food addiction[5-6], which is a significant cause of obesity in some cases[7]. This study observed the efficacy of acupoint thread-embedding in treating obesity coupled with food addiction by targeting food addiction. The report is given as follows.
1 Clinical Materials
1.1 Diagnostic criteria
1.1.1 Diagnostic criteria in Western medicine
According to the diagnostic criteria for obesity in Asian adults put forward by World Health Organization Working Group on Obesity in Western Pacific Region in 2000, obesity was diagnosed when body mass index(BMI) ≥28 kg/m2[8].
1.1.2 Diagnostic criteria in traditional Chinese medicine (TCM)
The criteria were tailored to diagnose obesity of damp-heat in stomach and intestine pattern in TCM based on theGuiding Principles for Clinical Study of New Chinese Medicines[9]. A fat body, indulged in foods rich in fat and sugar, excessive and insatiable appetite, heavy body and limbs, feeling tired and sleeping a lot, with a dry mouth but not eager for drinks, constipated or diarrheal, red tongue body covered by white or yellow greasy coating, slippery pulse.
1.1.3 Diagnostic criteria for food addiction
Food addiction was diagnosed by referring the modified Yale food addiction scale version 2.0 (YFAS 2.0)[10], when 2 or more items from the diagnostic criteria and one of the last two clinical severity items were met.
1.2 Inclusion criteria
The diagnostic criteria in both TCM and Western medicine were met; food addiction was diagnosed; aged between 18 and 50 years old; not in any weight loss program in the recent 6 months; joined voluntarily and had the informed consent form signed.
1.3 Exclusion criteria
Allergic to polyglycolic acid (PGA) suture line; coupled with other metabolic diseases; with severe heart, liver,lung or kidney complications; women during pregnancy or lactation.
1.4 Grouping method
This study followed a completely randomized design and the sample size was 65 cases. The researchers obtained the random allocation results according to the random number table and put them into envelopes. The envelopes were then sealed and coded. When a subject was enrolled, the envelope with the number matching the patient’s sequence was opened and the subject would be allocated into the corresponding group.
1.5 Statistical methods
The SPSS version 18.0 statistical software was used in this study. Measurement data were expressed as mean ±standard deviation (±s); paired samplest-test was adopted for intra-group comparisons and independent samplest-test for between-group comparisons; those not conforming to normal distribution or homogeneity of variance were processed by rank sum test. For repeated measurement data, one-way analysis of variance was used if Huynh-Feldt was satisfied while multivariate analysis of variance was employed if not.Chi-square test was implied for enumeration data.Statistical significance was confirmed whenP<0.05.
1.6 General data
A total of 65 patients were recruited in this trial, all from the Acupuncture-moxibustion Department and Multidisciplinary Department for Physical Appearance Adjustment of Suzhou TCM Hospital Affiliated to Nanjing University of Chinese Medicine between June 2017 and June 2019. Prior to enrollment, the participants were informed of the objective, methods and precautions of this study and signed the informed consent form. This trial had been approved by the Ethics Committee of Suzhou TCM Hospital Affiliated to Nanjing University of Chinese Medicine (Approval No. 2017-028).
No dropouts in the thread-embedding group and all the 33 cases completed the study, with ages between 19 and 48 years old and disease duration ranging between 1 year and 30 years. Of the 32 cases in the diet group, 4 cases dropped out and 28 cases finished the study, with ages between 19 and 49 years old and disease duration varied between 1 year and 30 years. The baseline data were statistically consistent between the two groups (allP>0.05), suggesting the comparability (Table 1).
2 Treatment Methods
2.1 Thread-embedding group
Thread-embedding: The acupoints were selected based on the principle of pattern differentiation,referring the acupoint prescription in acupuncture treatment of obesity of dampness-heat in stomach and intestine.

Table 1. Comparison of general data
Acupoints: Prescription 1 included Tianshu (ST 25),Daheng (SP 15), Zhongwan (CV 12), Shangwan (CV 13),Pishu (BL 20), Xinshu (BL 15), Fenglong (ST 40), Zusanli(ST 36), Yinlingquan (SP 9), Shangjuxu (ST 37) and Sanyinjiao (SP 6); prescription 2 included Tianshu (ST 25),Daheng (SP 15), Zhongwan (CV 12), Shangwan (CV 13),Daimai (GB 26), Ganshu (BL 18), Weishu (BL 21), Neiting(ST 44), Yinlingquan (SP 9), Fenglong (ST 40) and Zusanli(ST 36). The two prescriptions were used alternately.
Operation: Self-made thread-embedding kit [1 kidney tray, size No. 7 disposable syringe needle, 1 pair of forceps and PGA suture line (specification: 3-0, 1.5 cm,Suzhou Medical Appliance Factory, China)], sterile gloves and 20 band-aids. The PGA suture line was placed into the size No. 7 disposable syringe needle first. After standard sterilization for the acupoints with iodine, the needle was swiftly punctured into acupoint and slowly removed the needle when needling qi was obtained by lifting-thrusting and twirling manipulations. The PGA suture line was left inside the acupoint after the needle was withdrawn, and then the needle hole was covered by a piece of band-aid. The patients were asked to tear off the band-aids 24 h later on their own. The threadembedding treatment was conducted every 2 weeks,with 2 sessions as 1 course of treatment. The relevant indicators were detected after 3 treatment courses(about 12 weeks) and at the 6-month follow-up. The patients were also educated on health and diet during treatment and follow-up.
2.2 Diet group
Patients in the diet group were educated on healthy diet. The total calorie demand was calculated for each patient according to their figure, height and activity level[11]. Total daily intake (kcal) = Ideal BM (kg) × Energy demand (kcal)/kg. Note: 1 kcal = 4.19 kJ. Ideal BM (kg) =Height (cm) - 100 (male) or 105 (female). Based on the activity intensity, the daily energy supply for obese patients was defined as: bed resting, 15 kcal/kg; mild activity, 20-25 kcal/kg; moderate activity, 30 kcal/kg;intense activity 35 kcal/kg. The individual energy demand was transformed into the number of food servings, which was equal to total daily calorie demand/90 kcal. For example, an obese male who was 170 cm tall and weighed 90 kg performing moderate activity would demand a total daily calorie of 70×30=2 100 kcal, and his number of food servings would be 2 100÷90=23.3. For him, each serving of food contained grains and potatoes 25 g, vegetables 500 g,fruits 200 g, beans 25 g, dairy food 160 g, meats and eggs 50 g, nuts 15 g and fats 10 g. Carbohydrates are mostly found in cereals and potatoes and a low-carbohydrate diet contains 30% of carbohydrates according to the criteria from both China and abroad[10]. In this study, we limited the intake of carbohydrates at dinner and distributed the required amount to breakfast and lunch instead. Every week, we contacted the patients via phone or WeChat to learn about and supervise their diet pattern and offered guidance accordingly to ensure the reasonable intake of calorie and also avoid hypoglycemia.The relevant parameters were measured 12 weeks later,as well as at the 6-month follow-up. During follow-up,the patients were still given health education and followed a healthy diet pattern.
3 Observation of Therapeutic Efficacy
3.1 Outcome measures
3.1.1 BM and BMI
Height and BM were measured before and after treatment and at the 6-month follow-up on an empty stomach using a weight scale and tape measure. BMI was calculated accordingly.
3.1.2 Waist circumference (WC), hip circumference(HC) and waist-to-hip ratio (WHR)
WC and HC were measured before and after treatment and at the 6-month follow-up. WHR was calculated accordingly. When measured, the patient should stand straight, have the abdomen relaxed, hand down, feet together, and breathe naturally, instead of keeping the stomach in and holding the breath. WC was taken horizontally by 1 cm above the belly button and HC was measured at the level of the greatest protrusion of the bottom. WHR=WC/HC.
3.1.3 Body fat rate (BFR) and basal metabolic rate(BMR)
BFR and BMR were estimated before and after treatment and at the 6-month follow-up. To measure BFR, the patient was asked to stand straight with the feet shoulder-width apart and clutched the Omron body fat meter [HBF-306, Omron (Dalian) Co., Ltd., China] where the data of patient’s gender, height and BM were already entered. BMR was calculated using the basal energy expenditure/BM.
3.1.4 YFAS 2.0[10]
Food addiction intensity was estimated before and after treatment and at the 6-month follow-up using YFAS 2.0. At a resting state, the patient answered ‘yes’ or ‘no’to the 11 diagnostic questions and 2 questions judging the disease severity, 1 point for ‘yes’ and 0 point for ‘no’.The highest score would be 11+2 while the lowest would be 0 + 0. A state of food addiction was confirmed when the score ≥2+1, the higher the score, the more serious the condition.
3.1.5 Efficacy evaluation criteria
This was made by referringDiagnosis and Efficacy Evaluation Criteria for Simple Obesity[12].
Clinical recovery: BMI <27 kg/m2, together with BFR<20% in males and BFR <30% in females.
Markedly effective: BMI decreased by ≥4 kg/m2and BFR decreased by >5%.
Effective: BMI decreased by ≥2 kg/m2but <4 kg/m2and BFR decreased by 3%-5%.
Invalid: BMI decreased by <2 kg/m2and BFR decreased by <3%.
There is no universal standard for the estimation of treatment efficacy for food addiction. In this case, we took the score of YFAS 2.0 <2+1 points as the standard for clinical recovery of food addiction by referring the modified YFAS 2.0[10].
3.2 Results
3.2.1 Comparison of therapeutic efficacy
At the end of treatment, the total effective rate was higher in the diet group than in the thread-embedding group, but the difference was statistically insignificant(P>0.05), suggesting the efficacy was equivalent (Table 2).
At the 6-month follow-up, the total effective rate was notably higher in the thread-embedding group than in the diet group, and the difference was statistically significant (P<0.05), indicating that the threadembedding group produced more significant long-term efficacy than the diet group (Table 3).
3.2.2 Comparison of BM and BMI
BM and BMI declined significantly after treatment and at the follow-up in both groups (allP<0.01). There were no significant differences in the improvements of BM and BMI between the two groups at the end of treatment (P>0.05); at the 6-month follow-up, the improvements of BM and BMI were more significant in the thread-embedding group than in the diet group(bothP<0.05). Find the details in Table 4.

Table 2. Comparison of therapeutic efficacy by the end of treatment (case)

Table 3. Comparison of long-term therapeutic efficacy at the 6-month follow-up (case)
Table 4. Comparison of BM and BMI at different time points (±s)
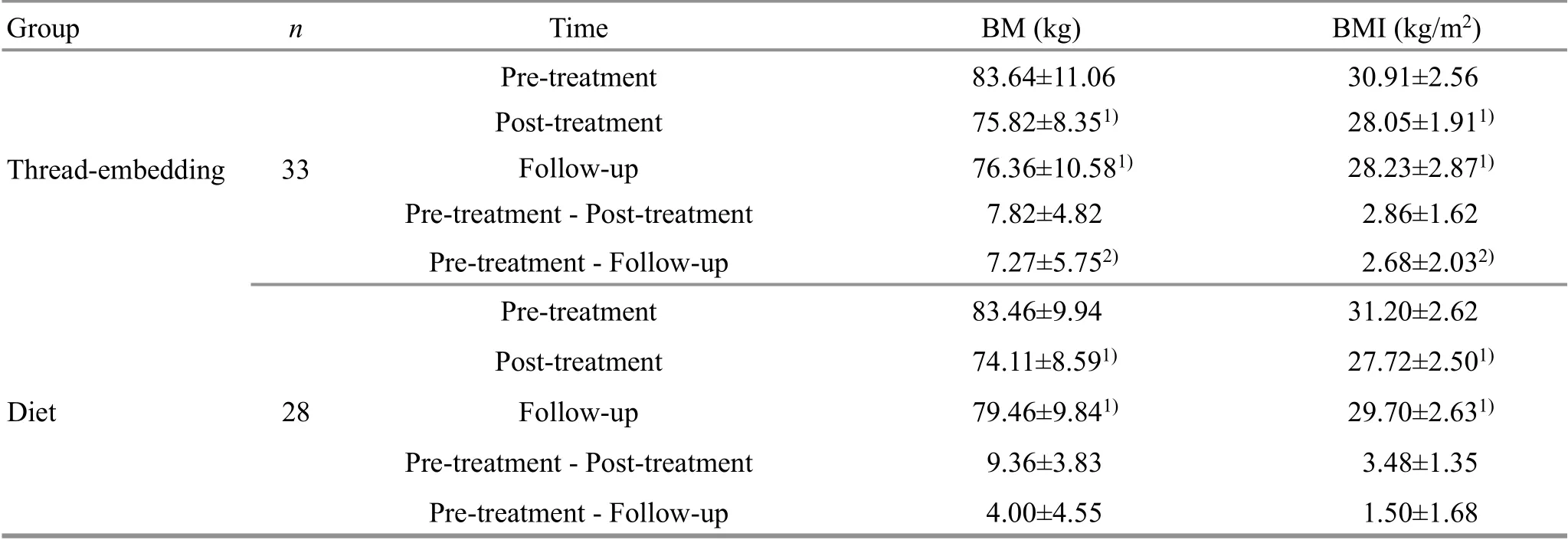
Table 4. Comparison of BM and BMI at different time points (±s)
Note: Compared with the same group before treatment, 1) P<0.01; compared with the diet group, 2) P<0.01
Group n Time BM (kg) BMI (kg/m2)Pre-treatment 83.64±11.06 30.91±2.56 Thread-embedding 33 Post-treatment 75.82±8.351) 28.05±1.911)Follow-up 76.36±10.581) 28.23±2.871)Pre-treatment - Post-treatment 7.82±4.82 2.86±1.62 Pre-treatment - Follow-up 7.27±5.752) 2.68±2.032)Pre-treatment 83.46±9.94 31.20±2.62 Diet 28 Post-treatment 74.11±8.591) 27.72±2.501)Follow-up 79.46±9.841) 29.70±2.631)Pre-treatment - Post-treatment 9.36±3.83 3.48±1.35 Pre-treatment - Follow-up 4.00±4.55 1.50±1.68
3.2.3 Comparison of WC, HC and WHR
WC, HC and WHR dropped significantly after treatment in both groups (allP<0.01), while the between-group differences were statistically insignificant (allP>0.05); at the follow-up, the improvements of WC and WHR were more significant in the thread-embedding group than in the diet group(bothP<0.05). See the details in Table 5.
3.2.4 Comparison of BFR and BMR
BFR decreased significantly in both groups after treatment (bothP<0.01), though the between-group difference was statistically insignificant (P>0.05); at the 6-month follow-up, there was a significant difference in the improvement of BFR between the two groups(P<0.05), (Table 6).
BMR increased after treatment in the threadembedding group (P<0.05), while the statistical significance disappeared at follow-up (P>0.05); BMR seemed to decrease after treatment and at follow-up in the diet group, but the intra-group differences were statistically insignificant (P>0.05). The improvements of BMR were more significant in the thread-embedding group than in the diet group after treatment and at follow-up (bothP<0.05), (Table 6).
3.2.5 Comparison of food addiction intensity
Based on YFAS 2.0, the recovery rate was markedly higher in the thread-embedding group than in the diet group after treatment and at follow-up (bothP<0.01),suggesting that acupoint thread-embedding can produce more significant efficacy than low-carbohydrate diet in improving food addiction (Table 7).
Table 5. Comparison of WC, HC and WHR at different time points (±s)

Table 5. Comparison of WC, HC and WHR at different time points (±s)
Note: Compared with the same group before treatment, 1) P<0.01; compared with the diet group, 2) P<0.01
Group n Time WC (cm) HC (cm) WHR Thread-embedding 33 Pre-treatment 91.61±5.31 100.24±6.91 0.92±0.52 Post-treatment 82.87±5.621) 94.97±6.721) 0.87±0.451)Follow-up 83.64±7.071) 95.64±8.151) 0.88±0.47 Pre-treatment - Post-treatment 8.73±3.54 5.27±2.72 0.04±0.03 Pre-treatment - Follow-up 7.97±5.672) 4.61±3.25 0.04±0.042)Pre-treatment 91.43±4.46 100.25±6.18 0.91±0.48 Diet 28 Post-treatment 83.93±5.331) 94.43±5.951) 0.89±0.651)Follow-up 87.79±6.10 97.07±6.94 0.91±0.60 Pre-treatment - Post-treatment 7.50±3.17 5.14±2.40 0.03±0.02 Pre-treatment - Follow-up 3.64±4.55 3.18±2.65 0.01±0.03
Table 6. Comparison of BFR and BMR at different time points (±s)

Table 6. Comparison of BFR and BMR at different time points (±s)
Note: Compared with the same group before treatment, 1) P<0.01, 2) P<0.05; compared with the diet group, 3) P<0.05
Group n Time BFR (%) BMR (kJ/kg)Thread-embedding 33 Pre-treatment 37.05±2.05 16.34±2.22 Post-treatment 36.12±1.871) 17.03±2.252)Follow-up 36.23±1.901) 16.79±2.58 Pre-treatment - Post-treatment 0.92±0.68 -0.69±1.303)Pre-treatment - Follow-up 0.82±0.723) -0.44±2.083)Pre-treatment 37.24±1.97 16.18±1.92 Diet 28 Post-treatment 36.36±1.991) 16.14±2.43 Follow-up 36.79±2.032) 15.81±1.68 Pre-treatment - Post-treatment 0.88±0.51 0.36±1.37 Pre-treatment - Follow-up 0.45±0.49 0.37±1.04

Table 7. Comparison of food addiction at different time points (case)
4 Discussion
The record of obesity can be traced back to as early as the era ofHuang Di Nei Jing(Yellow Emperor’s Classic of Internal Medicine), involving its causes, pathogenesis,treatment principles, treatment methods and many other aspects. According toSu Wen(Essential Questions),obesity is caused by abnormal diet. Modern Chinese medicine scientists believe that the pathogenesis is mostly dampness-heat accumulated in the stomach and intestines[13].Through research, Yu C,et al[14]hold that the endogenous phlegm and dampness should be the basis of various types of obesity.
Food addiction is manifested by the behavioral individual’s inability to rationally control the amount and time of eating a certain food, and the tolerance of foods continues to increase in the process of overeating, and a series of withdrawal symptoms are developing during the withdrawal process, which aggravates the craving for food, leading to repeated overeating behavior. Some researchers have proposed that in the neural response mode, food addiction is similar to alcohol and nicotine addiction, but the specific similar reaction points are not clear[15-16], which is also a difficult task in the treatment of obesity. Although the term of food addiction has been accepted by more and more researchers, food is a basic life-sustaining substance, which is essentially different from mental addictive substances. Therefore, many scholars believe that there must be another specific neurobiological mechanism[17].
The incidence of food addiction among obese people is 24.9%. A 2015 study in Australia showed that 70.0% of patients with type 2 diabetes met the diagnosis of food addiction, and the patients with type 2 diabetes who met the diagnosis of food addiction had an elevated BMI[6].Johnson PM,et al[18]found that feeding rats with tasty high-energy food can trigger addictive behaviors and directly lead to obesity in the rats. This was reportedly due to the decreased dopamine signal in the striatum of the reward center in the rat brain, similar to the effect of exposure to addictive drugs. More and more researchers started to pay attention to the relationship between obesity and food addiction, and tried to explain the correlation between the two from multiple angles such as nerve and immunity, seeking the best way to solve the problem of food-dependent obesity.
Thread-embedding integrates traditional acupuncture and modern medical theories and wins a pivotal position in the treatment of obesity with a solid clinical foundation. Its mechanism of action is more complicated.Chen LS,et al[19]found that thread-embedding therapy may stimulate the innate immune response pattern of topical tissue and enhance the phagocytosis and clearance ability of the immune system, thereby intervening the chronic inflammatory response of adipose tissue in obese patients and reducing the BM.
Low-carbohydrate diet is currently a quite popular nutritional treatment mode[20]. A low-carbohydrate diet has a significant effect on weight control in a short period of time. Its mode of action is mainly to promote body fat metabolism by keeping the body in a state of lack of available carbohydrates, so as to achieve the purpose of weight control.
In this study, with syndrome differentiation as the basic principle, together with Professor Ai Bing-wei's clinical experience, Tianshu (ST 25) and Daheng (SP 15)were selected for dredging intestines, descending the turbid and reducing the fat; Yinlingquan (SP 9) and Fenglong (ST 40) for releasing dampness and resolving phlegm; Zhongwan (CV 12) and Shangwan (CV 13) for harmonizing the stomach and invigorating the spleen to eliminate dampness; Zusanli (ST 36) and Shangjuxu(ST 37) for activating stomach qi and regulating the function of stomach and intestines; Sanyinjiao (SP 6) and Daimai (GB 26) for invigorating the spleen and stomach,and removing dampness and phlegm; Neiting (ST 44) for clearing and reducing the fire in the stomach and purges the turbid qi. Xinshu (BL 15), Pishu (BL 20) and Ganshu(BL 18) were used as adjunct points to reconcile qi and blood and calm the heart and mind, so as to mitigate the withdrawal syndrome after food addiction.
This study included obese patients of dampness-heat in stomach and intestine pattern. The results showed that: in terms of overall efficacy, the low-carbohydrate diet and acupoint thread-embedding worked equivalently at the end of the treatment course, but after 6 months of follow-up, the thread-embedding group showed a better result than the diet group; in terms of BM and BMI, at the end of the treatment, the diet group improved more than the thread-embedding group, but the difference between the two groups was not statistically significant, and at the 6-month follow-up, the thread-embedding group showed significant advantage compared with the diet group; in terms of WC, HC and WHR, the two groups had similar efficacy at the end of treatment, but at follow-up, the thread-embedding group was significantly better than the diet group except for HC; in terms of BFR, the two performed equivalently by the end of treatment, while the thread-embedding group was estimated better than the diet group at follow-up; regarding BMR, it increased both after treatment and at follow-up in the thread-embedding group but decreased in the diet group, indicating that the thread-embedding group was superior to the diet group in improving BMR; the food addiction state also changed more significantly in the thread-embedding group than in the diet group.
The results of this study suggested that acupoint thread-embedding showed significant advantage in long-term efficacy, while low-carbohydrate diet resulted in a higher rate of relapse. Thread-embedding therapy may achieve its goal of weight loss by increasing the patient's BMR and suppressing their craving for food.This also reminds us that the key to weight reduction in obese patients with food addiction should be the control of patients' food desire, targeting the ‘addiction’. Diet control alone can achieve weight loss for a certain time,but it cannot solve the patient's food addiction problem,or even further aggravates the patient's craving for food.It has no advantage regarding the patient's long-term weight control. This somewhat also answers the question of ‘rebound’ in obese patients after losing weight. Since thread-embedding therapy can improve the obese state as well as food addiction, producing definite efficacy, so it is generally more conducive to weight loss in this patient group, and thus can be promoted in clinical practice.
Due to limited funding, the sample size was not large enough in this study, and the research cycle was rather short, which may cause a certain bias to the results.Besides, scales for evaluating the quality of life and mental state were not introduced in this study. In the future, we will perform a long-term observation amongst the participants to get the full picture of their changes from various aspects for more systemically understanding the long-term efficacy of threadembedding therapy for patients with food addiction.
Conflict of Interest
There is no potential conflict of interest in this article.
Acknowledgments
This work was supported by Project of Jiangsu Provincial Administration of Traditional Chinese Medicine(江苏省中医药管理局, No. YB2017005).
Statement of Informed Consent
This trial had been approved by the Ethics Committee of Suzhou TCM Hospital Affiliated to Nanjing University of Chinese Medicine (Approval No. 2017-028). Informed consent was obtained from all individual participants.
Received: 20 March 2020/Accepted: 10 July 2020
猜你喜欢
杂志排行

Journal of Acupuncture and Tuina Science的其它文章
- Assessment of the safety and efficacy of acupuncture in erectile dysfunction treatment
- Clinical observation of heat-sensitive moxibustion for acute ischemic stroke
- Efficacy observation of Zhi Shen Tiao Sui acupuncture method for depression after ischemic stroke
- Clinical observation on acupoint pressure plus longsnake moxibustion for upper-limb spastic hemiplegia after cerebral infarction
- Effect of mild moxibustion on cancer-related fatigue,serum ghrelin and adiponectin in patients undergoing chemotherapy after colorectal cancer surgery
- Effects of acupuncture plus spinal manipulations on physical functioning and biochemical indicators in patients with ankylosing spondylitis