Depression, periodontitis, caries and missing teeth in the USA, NHANES 2009-2014
2021-01-12MuathAldosarMohammadHelmiErinneKennedyRiddhiBadamiaSatomiOdaniIsraelAgakuConstantineVardavas
Muath Aldosar i , Mohammad Helmi, Erinne N Kennedy, Riddhi Badamia, Satomi Odani, Israel Agaku, Constantine Vardavas,4
ABSTRACT
Purpose This study aimed to investigate the association between self- reported depressive symptoms and oral diseases in US adults, including periodontitis, caries, missing teeth and untreated dental caries.
Design This study was designed as a secondary data analysis of a cross- sectional survey. We conducted descriptive, multivariable logistic and Poisson regression analyses on weighted data.
Setting US National Health and Nutrition Examination Survey 2009—2014 data.
Participants Individuals aged ≥30 years who completed a periodontal examination and depression screening (n=9799).
Results 21.6% (28.9 million) of adults aged ≥30 years reported depressive symptoms, with a higher prevalence among females, current smokers and participants with lower income and education status. More than half of the adults with moderate depressive symptoms had periodontal diseases, and more than one- third had teeth with untreated dental caries. After adjusting for sociodemographics, behavioural factors, having diabetes and psychotherapeutic medication use, depressive symptoms were associated with poorer oral health. Severe depressive symptoms were associated with higher odds of mild periodontitis (2.20; 99% CI 1.03 to 4.66). For those with mild depressive symptoms, the mean number of missing teeth was 1.20 (99% CI 1.06 to 1.37) times the average of non- symptomatic individuals; and 1.38 times (99% CI 1.15 to 1.66) among individuals with moderate depressive symptoms.
Conclusions Depressive symptoms were associated with mild periodontitis and a greater number of missing teeth, while having teeth with untreated dental caries was attributed to sociodemographic factors. Awareness of oral health status among patients with depressive symptoms can inform both dental and mental health providers to develop tailored treatment and help patients achieve overall wellness.
lNTRODUCTlON
Depression is a diagnosable and treatable health condition distinct from experiences that occur normally from time to time such as feelings of fear, sadness or stress. Based on certain symptoms, depressive disorders are categorised into major depressive disorders, persistent depressive disorders and specified or unspecified depressive disorders.1Symp—toms of depression can include increased risk for social isolation, feelings of hope—lessness, restlessness, difficulty performing any activity, aches or pains and substance abuse.2—5In severe cases, depression is associ—ated with increased risk of suicidal ideation, suicide attempts and death.6As depressive symptoms are heterogeneous, not everyone who is depressed exhibits the same symp—toms; hence, depression might manifest in different symptoms depending on an individ—ual’s age, ethnicity, lifestyle and other socio—demographic conditions.
WHO reported that, globally, more than 300 million people (4.4% of the world popu—lation) were living with depression in 2015, an increase of almost 18% from 2005.7According to the National Institute of Health, depression is the most common mental health disorder in the USA.8Using the Patient Health Questionnaire—9 (PHQ—9) to diagnose depression, the National Health and Nutri—tion Examination Survey (NHANES) cycle in 2018 showed 8.1% of adults aged 20 or older had depression in USA.5Depression was most prevalent among non— Hispanic whites (9.2%) and almost twice as prevalent among women (10.4%) than men (5.5%).5
Several studies have reported depressive symptoms to be associated with poorer health and physical illness such as coronary heart disease, obesity and sleep depri—vation.9—11The association of depressive disorders with poor oral health has also been reported in the dental literature. Similar to the impact of oral disease, the conse—quences of depression affect the overall well— being of the individual, not just their mental health.12Nationally, data show a relationship between poor oral health and depressive symptoms, independent of inflammatory path—ways associated with increased C reactive protein and/or obesity.13A positive association has been demonstrated between poor oral health (ie, untreated tooth decay and tooth loss) and depressive disorders. However, the studies used in this 2016 systematic review used small sample sizes and often presented self— reported oral diseases.14In 2018, a systematic review and meta— analysis consistently reported tooth decay, tooth loss and edentulism associ—ated with depression.15
Our study addresses the gaps presented in the currently available literature by including objective, clinical dental examination data instead of solely self— reported oral diseases. Using the most recent NHANES data, we evaluate the associations among different sever—ities of depressive symptoms with clinically assessed oral diseases and missing teeth in non— institutionalised US adults.
MATERlALS AND METHODS
Study design and population
We used pooled NHANES data from 2009 to 2014. NHANES is a cross— sectional, nationally representative survey of the non— institutionalised US population that collects data via self— reported questionnaires, labora—tory assessments and clinical exams.16Participants in the analytical sample were at least 30 years old and had completed an NHANES oral examination and a nine— item screening and diagnostic tool for depression called the PHQ—9.16The PHQ—9 is designed to measure depres—sive symptoms within a 2— week period before the survey that align with the American Psychiatric Association’s diagnostic criteria for depressive disorders.17—19While a diagnosis of depression typically does not rely solely on a single questionnaire, cut— off scores for the diagnosis of severe depression have been developed and validated using the PHQ—9.20
The total sample size included 9799 participants in the three pooled cycles with periodontal examination data from 2009 to 2014 as well as 7011 participants in the two pooled cycles with clinical data recording dental caries and missing teeth from 2011 to 2014. The unweighted response rate of the examined sample was 77% from 2009 to 2010, 69.5% from 2011 to 2012, and 68.5% from 2013 to 2014. Written informed consent was obtained from all participants.
Clinical assessment of oral diseases
Calibrated dental examiners performed all clinical exam—inations of periodontal and dental status for NHANES participants. Using the definitions from the Centers for Disease Control and Prevention and the American Academy of Periodontics /, periodontal status was catego—rised into three groups: severe, moderate and mild. Peri—odontitis was deemed severe if there were two or more interproximal sites with ≥6 mm of loss of attachment (not on the same tooth) and one or more interproximal sites with probing depths of ≥5 mm. Moderate periodon—titis was defined as two or more interproximal sites with ≥4 mm of loss of attachment (not on the same tooth) or two or more interproximal sites with probing depths of ≥5 mm (not on the same tooth). Mild periodontitis was defined as either two or more interproximal sites with ≥3 mm of loss of attachment and two or more interprox—imal sites with ≥4 mm of probing depths (not on the same tooth) or one or more interproximal sites with probing depths of ≥5 mm.
The presence of any periodontitis at all was also recorded as an aggregate measure.21Additionally, we assessed the prevalence of participants with untreated dental caries, the number of teeth with untreated dental caries and the number of missing teeth.
Definition of depression and confounding factors
The severity of depressive symptoms was measured using the PHQ—9, a nine— item screening instrument that measures the frequency of self— reported depression— related symptoms over the 2 weeks preceding the ques—tionnaire. Based on the frequency of the symptoms, participants responded to each question by ranking symptom frequency: 0 for ‘not at all,’ 1 for ‘several days,’ 2 for ‘more than half the days’ and 3 for ‘nearly every day.’ The PHQ—9 classifies the severity of depressive symp—toms based on the total score. A total score in the range of 0—4 classifies depressive symptoms as minimal; 5—9 clas—sifies depressive symptoms as mild; 10—14, moderate and 15—27, severe.1718
Other independent variables we included in the anal—ysis were: age (30—34, 35—49, 50—64, 65+), sex (male or female), family income ratio to the federal poverty level (<100%, 100%—199%, 200%—499%, 500%+), education level (less than high school, completed high school/GED and education beyond high school), race/ethnicity (non— Hispanic white, non— Hispanic black, non— Hispanic other and Hispanic), smoking status (never, former or current smoker), current heavy alcohol consumption (≥2.5 drinks/day for men, ≥1.5 drinks/day for women), use of psychotherapeutic medications (taking antidepressant and/or antipsychotic medication, not taking psychother—apeutic medications) and report of diagnosed diabetes mellitus (diabetic, non— diabetic).
Statistical analysis
We obtained descriptive statistics to examine the prev—alence of depressive symptoms for each independent factor; then, we estimated the overall prevalence and severity of oral diseases among the four levels of depres—sive symptoms. With the corresponding 99% CI, we reported the prevalence of periodontitis, the presence of untreated dental caries, the average number of teeth with untreated dental caries, and the number of missing teeth. Weighted percentages were used to report nation—ally representative results. We also performed analyses on pooled data across cycles of NHANES and recalibrated the weights by dividing them by the number of cycles; then, we used these recalibrated weights to accurately extrapolate the population counts. For SE estimations, we used Taylor linearisation methods in the survey proce—dures with the provided masked variance pseudostratum and masked variance pseudoprimary sampling units .
We used logistic regression models for binary oral disease regarding mild to moderate to severe periodon—titis and the presence of untreated dental caries. Poisson regression models were used for the mean numbers of missing teeth and teeth with untreated dental caries to esti—mate crude and adjusted measures of association between depressive symptoms and study endpoints. To determine OR, we applied simple and multivariable logistic regres—sions to estimate the crude and adjusted OR of peri—odontal diseases and untreated dental caries, comparing the levels of the severity of depressive symptoms to individ—uals with no reported depressive symptoms. Additionally, we used Poisson regressions to estimate the mean ratio of missing teeth and teeth with untreated dental caries to the severity level of reported depressive symptoms, using individuals without depressive symptoms as a reference. We controlled for the independent confounding factors in all multivariable regression models for the adjusted estimates, the directed acyclic graph (online supple—mental figure 1) provides a visual model for our assump—tions. The results were deemed statistically significant at p<0.01, and all statistical analyses were performed using Stata/MP V.16.1 (StataCorp).
RESULTS
Among non— institutionalised US adults aged ≥30 years, 21.6% of them reported having at least mild depressive symptoms within the last 2 weeks on the PHQ—9 (table 1). The highest prevalence of depressive symptoms was among females, current smokers and heavy alcohol drinkers. Additionally, the data showed that the prev—alence of depressive symptoms was higher among indi—viduals with lower education level, lower income, those taking antipsychotherapeutic medications and patients with diabetes.
Among US adults aged ≥30 years, the prevalence of mild, moderate or severe periodontitis was 42.1% (99% CI 38.3% to 46.0%), and the prevalence of having at least one tooth with untreated dental caries was 21.5% (99% CI 18.5% to 24.5%) (table 2). The average number per participant of teeth with an untreated carious lesion was 0.6 (99% CI 0.5 to 0.8) and of missing teeth was 4.9 (99% CI 4.2 to 5.6). Table 2 also shows that participants with moderate depressive symptoms had the highest preva—lence of periodontal disease—nearly half (52.4%; 99% CI 44.9% to 60.0%)—as well as the highest prevalence of teeth with untreated dental caries (36.3%; 99% CI 26.1% to 46.5%). This group averaged 1.1 teeth with untreated dental caries (99% CI 0.7 to 1.5) and 8.1 (99% CI 6.2 to 10.1) missing teeth.
Table 3 shows that periodontitis was more prevalent in participants reporting moderate and severe depressive symptoms than in participants reporting no depressive symptoms. After adjusting for potential confounding factors, the association between depressive symptoms and periodontitis disappeared, except among individuals with severe depressive symptoms who had 2.20 times the odds of mild periodontitis (99% CI 1.03 to 4.66) than individ—uals without depressive symptoms.
The mean number of teeth with untreated dental caries was higher in individuals who reported moderate (crude mean ratio=1.87; 99% CI 1.25 to 2.80) and severe (crude mean ratio=1.65; 99% CI 1.10 to 2.48) depressive symp—toms than in individuals who reported no depressive symptoms; however, this association disappeared after adjusting for confounding factors (table 4). The crude mean ratio of missing teeth was higher among symptom—atic individuals than among individuals with no depressive symptoms. Participants with mild depressive symptoms had a greater mean number of missing teeth than indi—viduals with no depressive symptoms (adjusted mean ratio=1.20; 99% CI 1.06 to 1.37), and individuals with moderate depressive symptoms had even a higher mean number of missing teeth (adjusted mean ratio=1.38; 99% CI 1.15 to 1.66).
DlSCUSSlON
Our study has addressed current gaps in the literature by using a secondary analysis of nationally representative NHANES data to explore the associations between self— reported depressive symptoms and an objective report of clinical oral diseases. While depressive symptoms are usually collapsed into just two categories of respondents—those who reported moderate depressive symptoms and those who did not—our paper increases the granularity of the data by evaluating four separate levels of depres—sion symptoms. Among non— institutionalised US adults aged ≥30 years, about one— fifth reported having at least mild depressive symptoms within the last 2 weeks on the PHQ—9. For clinical oral diseases, participants received complete clinical periodontal and dental examinations (in 2009—2014 cycles and in 2011—2014 cycles, respec—tively) which included more objective clinical data that help achieve more accurate diagnoses. Generally, depres—sive symptoms were associated with poor oral health, and participants with mild and moderate depressive symp—toms were missing more teeth than individuals with no depressive symptoms.
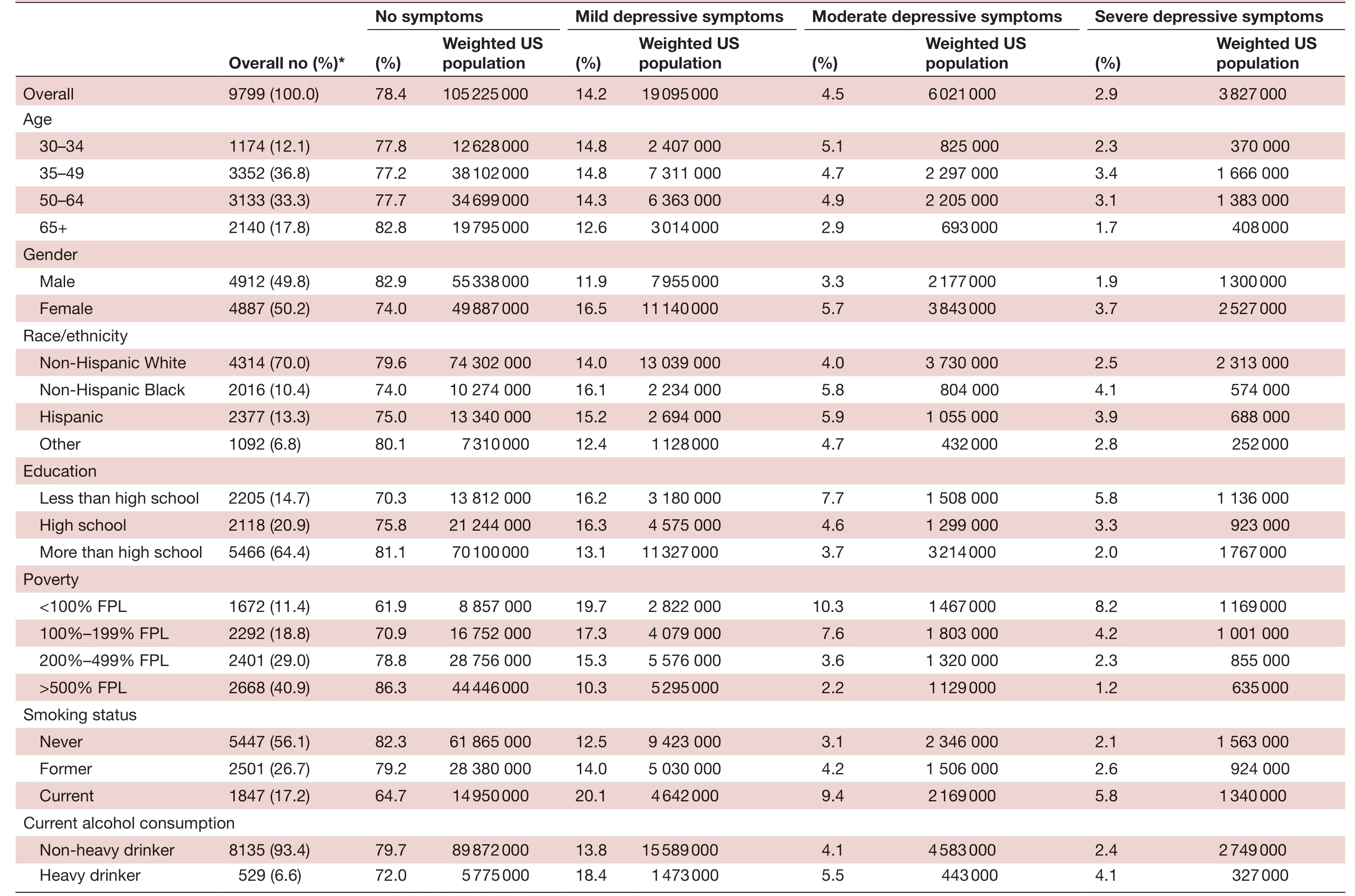
Table 1 Demographics and prevalence of depression among adults who have completed a periodontal examination and the PHQ-9 depression screening questionnaire in the National Health and Nutrition and Examination Survey, 2009–2014
Continued

Table 1 Continued

Table 2 Prevalence of types of periodontitis, presence of untreated caries, mean number of teeth with untreated caries and missing teeth by depressive symptoms among adults aged ≥30 years who completed a periodontal examination and the PHQ-9 depression screening questionnaire in the National Health and Nutrition and Examination Survey

Table 3 Logistic regression models of associations between depressive symptoms and periodontitis as well as presence of untreated dental caries among adults aged ≥30 years who completed a periodontal examination and the PHQ-9 depression screening questionnaire in the National Health and Nutrition and Examination Survey; 2009–2014 for periodontitis, 2011–2014 for dental caries
Limitations to this study include participation and reporting bias, challenges with temporality and a limited population. We controlled for potential known confounding factors to strengthen the internal validity of the estimates; however, problems with participation and reporting bias could present limitations on the data. For instance, populations with the most severe depressive symptoms may disproportionately choose not to partic—ipate in the survey. Additionally, while the PHQ—9 has been shown to successfully screen and diagnose depres—sive symptoms, it is not able to identify participants who received successful treatment for depression; thus, it requires participants to self— report symptoms over time, another process that can be susceptible to reporting bias. Second, because NHANES is a cross— sectional survey, we cannot evaluate the temporal relationship between depression and any oral diseases, or the duration of depressive symptoms. Finally, the dental examination was performed among non— institutionalised adults that were at least 30 years old, which limits our ability to eval—uate the association between depression and oral health among a younger population or vulnerable populations that are institutionalised.
In a systematic review published by Kiselyet al, the authors included fifteen papers to assess the relation—ship between psychiatric status and periodontal diseases. Five of these papers specifically examined depression and periodontitis; however, this review demonstrated no significant association between psychiatric status and periodontitis (pooled OR 0.99; 95% CI 0.93 to 1.06).14We noted a considerable amount of heterogeneity between the included studies and methods that collapsed periodontitis diseases into a dichotomous disease. Simi—larly, a more recent systematic review and meta— analysis published in 2018 also found no association between depression and periodontitis (pooled OR 0.96; 95% CI 0.84 to 1.10)15; the authors found only one study showing an increased risk of depression among individuals with periodontitis (HR 1.73; 95% CI 1.58 to 1.89).22
After adjusting for confounding factors, our results indicate that participants with severe depressive symp—toms have higher odds of mild periodontitis than partic—ipants with no depressive symptoms. This mild form of periodontitis among individuals with severe depressive symptoms could be explained by the disinterest in prac—tising appropriate oral hygiene.23However, depressive symptoms were not associated with moderate or severe periodontitis, as severe forms of periodontitis require longer periods to manifest, and the breakdown of teeth— supporting structures leads to the loss of teeth if neglected long enough. This possible explanation is supported by our finding that more missing teeth are found among individuals with mild or moderate depressive symptoms, possibly caused by severe untreated disease that resulted in a tooth extraction. Since teeth that are missing are not susceptible to other oral diseases, we believe the absence of the relationship between depressive symptoms and periodontitis can be explained by the increased numberof missing teeth among patients reporting depressive symptoms.
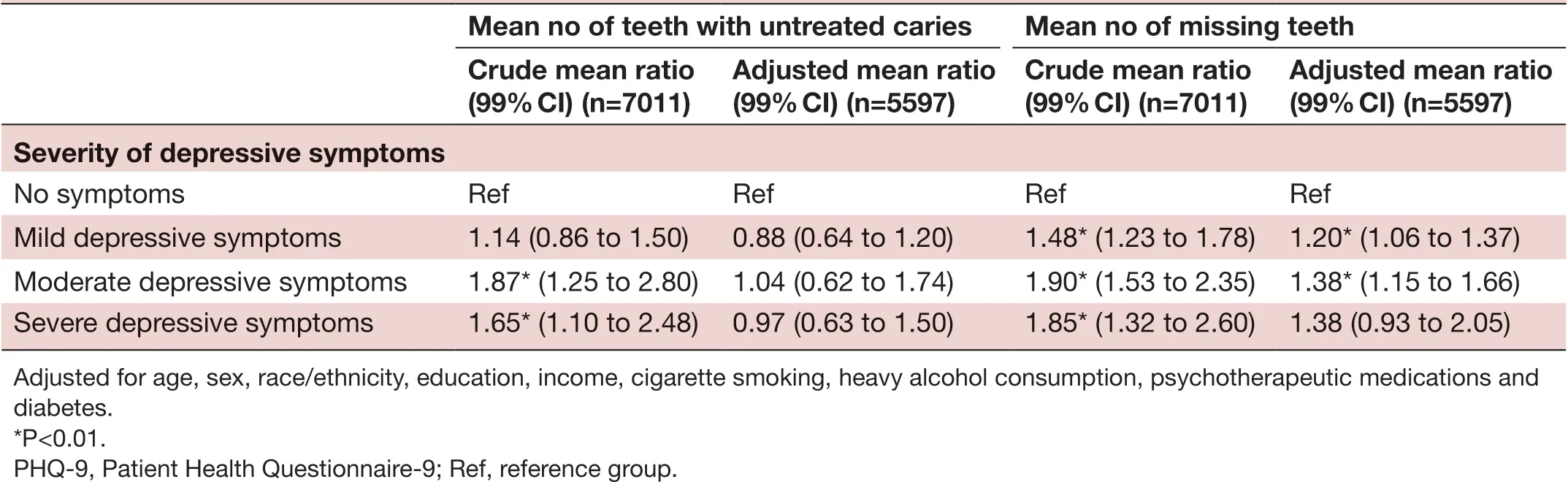
Table 4 Poisson regression analysis of the associations of depressive symptoms with mean number of teeth with untreated caries and missing teeth among adults aged ≥30 years who completed a periodontal examination and the PHQ-9 depression screening questionnaire in the National Health and Nutrition and Examination Survey; 2011–2014
Our findings suggest the severity of depressive symp—toms is associated with a higher average of missing teeth than in non— depressive individuals, which coincides with the findings from several studies in the literature.14152425We believe the influence of missing teeth among individ—uals reporting mild or moderate depressive symptoms could also explain our results regarding depression and dental caries. Although other studies have indicated an association between dental caries and depression, our research showed the association between the severity of depressive symptoms and dental caries to be eliminated after controlling for the confounding factors.1415Again, the extraction of affected dentition would explain the higher number of missing teeth, and the influence these missing teeth have on dissolving the association between dental caries and depressive symptoms. Differences between our findings and the findings from the literature might also be attributed to different methods of depres—sion assessment, differences in the population studied, or differences in oral examination protocols and diagnosis.
The current NHANES data indicate that nearly one out of five US adults aged 30 or above report depressive symp—toms.5Research indicates an overall association between depressive symptoms with adverse oral diseases. Although some studies investigate the effects of depressive disorders or mental illnesses generally while others focus on one specific type of depression, the most— reported adverse oral diseases have tended to be tooth decay, tooth loss, edentulism, dryness of the mouth and a decreased overall oral health— related quality of life. In general, individuals with depressive disorders can find activities of daily living, such as oral hygiene, challenging and may consume a cariogenic diet which in turn can lead to periodontal diseases and development of dental caries.26
The National Center for Health Statistics reports 12.7% of the population has taken an antidepressant medication in the last month.27Our analysis adjusted for individuals taking antidepressant and/or antipsychotic medications, the rationale being that psychotherapeutic medications has been associated with a significantly greater risk for symptoms of xerostomia (dry mouth).28Xerostomia is reported as the most common side effect of both antide—pressants and antipsychotics and has been associated with a decreased salivary flow rate.29A decreased flow rate, in turn, results in a lower salivary pH and reduced buffering capacity.30As a result, patients with depressive symptoms taking antidepressants often suffer from medication— induced xerostomia or MiX disease. A cross— sectional study evaluated the differences between three groups of medi—cally compromised patients: one group taking chronic medications not associated with xerostomia, one group taking a single drug associated with xerostomia, and one group taking multiple medications associated with xero—stomia. The study showed statistically and clinically signif—icant differences in unstimulated salivary flow, reporting of symptoms associated with xerostomia, and decreased quality of life with patients who take one or more xero—stomic medications.31Another recently published case report supplements these findings, connecting the oral environmental changes caused by MiX disease to resul—tant severe oral disease.32
As oral health professionals, we are tasked with treating the whole person. In the case of patients with depressive symptoms, this involves offensive preventive dental treat—ment that includes addressing symptoms associated with depression medications, early diagnosis and treatment of oral disease, and helping patients with an oral hygiene routine that supports their oral health and ability to perform the activities of daily living.32Moving forward, we recommend research exploring the temporal relation—ship between depression diagnosis, symptom severity and oral diseases.
CONCLUSlONS
Severe depressive symptoms were associated with a higher prevalence of mild periodontitis. In addition, mild and moderate depressive symptoms were associated with a higher number of missing teeth. In our analysis, depres—sive symptoms were not associated with greater odds of having teeth with untreated dental caries, mean number of carious lesions or moderate to severe periodontitis. Awareness of oral health status among patients with depression can encourage both dental and mental health providers to recognise oral diseases in a timely fashion, provide offensive preventive dentistry and encourage patients to continue to access regular and comprehensive oral healthcare.
TwitterMuath Aldosari @DrAldosari
AcknowledgementsThe authors thank the Centers for Disease Control and Prevention for the use of their publicly available data set. We would also like to thank Dr Mary Angela Tavares for her support in this manuscript.
CollaboratorsMary Angela Tavares; Centers for Disease Control and Prevention.
ContributorsMA, IA and CV contributed to the conception and design of study. SO prepared the dataset for analysis and MA carried out the analysis and data interpretation. MH, ENK and BR drafted the manuscript. All authors revised, discussed and approved the final manuscript. IA and CV supervised this project.
FundingThe authors have not declared a specific grant for this research from any funding agency in the public, commercial or not- for- profit sectors.
Competing interestsNone declared.
Patient consent for publicationNot required.
Ethics approvalThe Harvard Medical School’s IRB deemed this research exempted (IRB protocol #19-1611). The Harvard Medical School’s IRB deemed this research exempted (IRB protocol #19-1611).
Provenance and peer reviewNot commissioned; externally peer reviewed.
Data availability statementData are available in a public, open access repository. Data are available in a public, open access repository at the link here: https://www. cdc. gov/ nchs/ nhanes/ index. htm.
Supplemental materialThis content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer- reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Open accessThis is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY- NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non- commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non- commercial. See: http:// creativecommons. org/ licenses/ by- nc/ 4. 0/.
ORClD iDMuath Aldosari http:// orcid. org/ 0000- 0002- 2200- 2408
杂志排行

Family Medicine and Community Health的其它文章
- How well did Norwegian general practice prepare to address the COVID-19 pandemic?
- Perceived barriers and primary care access experiences among immigrant Bangladeshi men in Canada
- Family medicine residency training in Ghana after 20 years: resident attitudes about their education
- Bridging the mental health treatment gap: effects of a collaborative care intervention (matrix support) in the detection and treatment of mental disorders in a Brazilian city
- Cultural adaptation and content validity of a Chinese translation of the ‘Person- Centered Primary Care Measure’: findings from cognitive debriefing
- Effect of BATHE interview technique on patient satisfaction in an ambulatory family medicine centre in South India