Provision of primary care by specialist physicians: a systematic review
2020-04-04MuhammadJawadHashim
Muhammad Jawad Hashim
ABSTRACT Patients with stable chronic diseases such as diabetes and hypertension can be safely managed at the primary care level. Yet many such patients continue to follow- up with specialists at a higher expense with no added benefit.We introduce a new term to describe this phenomenon:scope inversion, defined as the provision of primary care by specialist physicians. We aimed to quantify the extent of scope inversion by conducting a systematic review.MEDLINE and five other databases were searched using the keywords ‘specialist AND (routine OR primary) AND provi*’ as well as other variations. The search was limited to human research without restrictions on language or date of publication. The inclusion criterion was studies on rates of the provision of routine primary care by specialist physicians. Thirteen observational studies met the inclusion criteria. A wide range of primary care involvement was observed among specialists, from 2.6% to 65% of clinic visits. Among children, 41.3% of visits with specialists were routine follow- ups for conditions such as allergic rhinitis and seborrhoeic dermatitis which could be managed in primary care. Data quality was moderate to low across the studies due to limitations of source data and varying definitions of primary care. Specialist physicians provide primary care to patients in a substantial proportion of clinic visits. Scope inversion is wasteful as it diverts patients to more expensive care without improving outcomes. A systems approach is needed to mitigate scope inversion and its harmful effects on healthcare service delivery.
lNTRODuCTlON
Common medical conditions, which can be safely managed in primary care, are sometimes treated by specialist physicians.1A new term is introduced in this article to highlight this health systems issue: scope inversion is defined as the provision of primary care by specialist physicians. It can occur as routine follow- up of chronic diseases or management of mild acute illnesses by a specialist (figure 1). Health systems aim to triage patients to appropriately qualified professionals. Scope inversion is inappropriate triage. As a health systems problem,scope inversion needs identification, quantification and mitigation.
Scope inversion can undermine the healthcare system in several insidious ways. Primary care provision by subspecialists leads to more expensive care without improving outcomes.
Tertiary care clinics can be bogged down by the large number of patients with primary care needs thus resulting in longer waiting times for available appointments for patients who genuinely need specialist care.2For example, patients who need appointments for specialty care can face waiting times of over 40 days.3Patients may expect to receive all of their care from specialists including treatment of common illnesses, further undermining primary care and wasting tertiary care resources. Specialist physicians do not perform the full scope of primary care such as preventive services and care coordination for patients with multiple chronic diseases.4Quality measures based on specialist- oriented guidelines are often inappropriately applied to primary care settings. The value of primary care extends to the care of the whole person and the overall health of populations.5
Although studies on referrals by family physicians and general practitioners (GPs)to specialists have been published repeatedly,6there is limited research on the issue of patients returning to GPs to resume continuity of care. There is some evidence that in health systems with robust primary care, generalists provide more efficient care.7For instance,medical expenses per episode of back pain are almost twice as high with orthopaedic surgeons compared with primary care physicians(PCPs).8Specialists are likely to utilise more diagnostic tests and procedures.8In health services research, care by specialist physicians does not result in better outcomes such as time to recovery or control of chronic diseases.9
Thus, the provision of primary care by specialists can undermine healthcare delivery in numerous ways. As this phenomenon is relatively understudied, we aimed to quantify the extent of scope inversion by conducting a systematic review.
METHODS Definitions
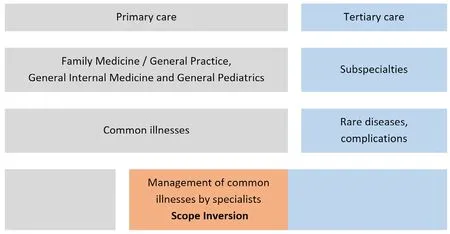
Figure 1 Scope inversion: the provision of primary care by specialist physicians.
A generalist may be defined as a physician(or other healthcare provider such as a nurse practitioner) trained to manage a wide scope of illnesses, whereas ‘specialist’ denotes a clinician who is trained to manage a narrow range of medical conditions(eg, a nephrologist or an ophthalmologist). A PCP is a generalist who provides continuity of care to patients while coordinating care with specialists. Such physicians include general physicians/internists, general paediatricians and GPs. The terms GP and family physician are used synonymously in the literature to indicate a PCP who has received training in the clinical specialty of General Practice/Family Medicine.5General Practice/Family Medicine is defined as the medical specialty that manages common and long- term illnesses in children and adults focusing on overall health and well- being.10
Search strategy
A systematic review was conducted using Preferred Reporting Items for Systematic Reviews and Meta- Analyses(PRISMA) guidelines.11The PRISMA statement provides a framework for conducting a comprehensive and reproducible review of research studies on a topic. MEDLINE,EBSCO Academic Search Complete, Scopus, Science-Direct, Web of Science and Embase databases were searched using the keywords ‘specialist AND (routine OR primary) AND provi*’ as well as other variations (online supplementary appendix). The inclusion criterion was studies on rates of provision of routine primary care by specialist physicians. All study designs were considered.Exclusion criteria were review articles with no original data, and articles on shared comanagement of patients by specialists and generalists, or on referrals from GPs to specialists. A trained medical research librarian experienced in conducting systematic reviews provided guidance on search strategy and methodology. The search was conducted over several months with the final refresh in December 2019.
Search results were screened for appropriate articles based on the titles and abstracts initially (see the online supplementary appendix for details on study selection).It was not feasible to combine the results from different studies in a meta- analysis due to the heterogeneity of individual study designs. Data quality was moderate to low across the studies due to limitations of source data and varying definitions of primary care.

Figure 2 Estimates of scope inversion.
RESuLTS
A wide range of estimates were found in the 13 studies that met inclusion criteria (Figure 2 and online supplementary appendix). An early study found the involvement of specialists in primary care to be between 9% and 34% depending on the definition of primary care.12Data from the US National Ambulatory Medical Care Survey(NAMCS) in 2002 showed that in about one- half of all clinic visits, specialist physicians indicated that they were the PCP for the patient.13Among children, 41.3% of visits with specialists were routine follow- ups for conditions such as allergic rhinitis and seborrhoeic dermatitis which‘could be managed in primary care settings’.14In the 2013 NAMCS, general surgeons, for instance, reported that they were providing primary care in 2.6% of patient visits (table 1; NAMCS 2013 data).15According to a US report on the care of the elderly, only 60% identified a family physician as their usual source of healthcare.16The remaining 40% of respondents were potentially receiving primary care from specialists. In a US population- based survey, 14% of respondents named a specialist as their source of primary care.17For example, 6% reported receiving primary healthcare from a cardiologist.17In fact, about half of the respondents were potentially relying on a specialist for their routine medical needs.17A review of earlier NAMCS data found that in 44% of visits to nephrologists and 65% of visits to infectious disease consultants, the specialist physicians reported being the PCP.9In Colorado, 46.5% of 2745 specialists reported providing primary care.18A retrospective analysis of a large US Medicare database reported that 25% of beneficiaries received care from a specialist.19
DlSCuSSlON
Specialist physicians provide primary care to patients in a substantial proportion of clinic visits, ranging from 2.6% to 65% of their consultations. This variation may be explained by the heterogeneity of study designs, data quality, different ways of defining primary care and the level of involvement of specialists. The latter has beencategorised in a typology by Kendall et al: family physiciandominated comanagement, specialist- dominated comanagement and exclusively specialist care.20In contrast,multidisciplinary shared care occurs when GPs refer patients to allied health professionals such as dieticians,physical therapists and psychologists.21

Table 1 Provision of primary care by specialists, according to specialty (n=2879)
We know that specialists provide less comprehensive primary care than generalists such as family physicians.9Thus, specialists tend to see fewer new problems, treat a limited range of conditions and provide less preventive care.7The scope of practice among specialist physicians is narrower in terms of the range of illnesses seen.22Although patients may identify a gynaecologist as their‘PCP’, they may not be receiving comprehensive primary care.23Primary care in this context is more than the care of a chronic condition. A specialist might counsel a patient to quit smoking if it helps to improve the disease status; however, this should not be construed as full primary care.
It is well recognised that a case mix of patients with the mild disease is well suited to the continuity of care by primary care doctors. For specialist physicians, having these stable patients on their panel improves performance measures while avoiding high- risk cases.24By shifting to stable patients with the controlled disease,specialists avoid clinical care that is more time and effortintensive. Among patients with stable chronic diseases,routine office visits are less complex and often billed at the same level as those with complex, unstable problems.Financial inducement may play a role in the ‘perennial follow- up’ of stable patients by specialists.25
The care provided by generalists and specialists is similar to common chronic diseases.2627Patients perceive family physicians positively when transitioning back from tertiary to primary care.28Thus, there seems to be no evidence- based rationale to continue the follow- up of patients with the mild stable disease with subspecialists. It is not surprising that the likelihood of consultation with a specialist physician by elderly patients is more linked to their incomes than healthcare needs.29Gaps in specialists’ clinical knowledge base often lead to cross- referrals to other specialties resulting in tortuous patient journeys leading to diagnostic delays.30
Some experts have noted that the shortage of family physicians may necessitate the provision of primary care by specialists.91231As such, continuity of care provided by these specialists is better than having no usual source of care.32Examples include ongoing care of HIV+ patients by infectious disease specialists and the care of patients on dialysis by nephrologists.20However, these stopgap measures should not be viewed as a long- term substitute for accessible and affordable primary care.
Limitations of this review include a dearth of studies,especially the lack of published research from outside the USA. The varying definitions of primary care and metrics used to quantify it make it difficult to pool the results in a meta- analysis or produce a summary statistic. Specialist physicians may gradually switch into generalist disciplines later in their careers.33The extent of primary care provision by specialists seems to have changed over the last few decades.9
Potential solutions to reduce scope inversion
The return of patients from specialists to primary care can be a potential ‘fault line’ in the continuum of care.34This observation underscores the need for a clear summary (such as a hospital discharge note)and a detailed patient care plan to be provided by the specialist to the GP.35Interclinician communication can guide the transfer of patient management from specialty to primary care.36Family physicians have raised this concern in earlier research.37Discussion of the care plan between the specialist and the family physician,either face- to- face or via teleconferencing, can reduce hospital readmissions and improve independent living and quality of life.38
Reminder letters to patients have improved follow- up rates with GPs from a baseline of 56%-90% after the mailings.39Innovative solutions such as a telemedicine service can reduce scope inversion by decreasing the need for face- to- face consultations with a specialist.40Community health services can augment the care provided by family physicians without transferring to a specialist.41Such strategies underscore the importance of the safe and timely return of patients to the care of communitybased GPs.37Generalists are essential to guide patients given the rising multimorbidity of chronic illnesses.42The overall goal of healthcare is integrated primary- specialist care exemplified by teamwork, information exchange,shared guidelines, continuous training, access to care and sustainable financing. Enforcement of timely return of stable patients to primary care is perhaps needed to reduce scope inversion.
AcknowledgementsThe authors would like to thank Linda Ostlundh, research librarian and director of the National Medical Library for her guidance in conducting the searches for the systematic review.
ContributorsMJH: conceived of the research idea, conducted the literature search and wrote the manuscript.
FundingThe authors have not declared a specific grant for this research from any funding agency in the public, commercial or not- for- profit sectors.
Competing interestsNone declared.
Patient consent for publicationNot required.
Provenance and peer reviewNot commissioned; externally peer reviewed.
Open accessThis is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY- NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non- commercially,and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non- commercial. See: http:// creativecommons. org/ licenses/ by- nc/ 4. 0/.
ORClD iDMuhammad Jawad Hashim http:// orcid. org/ 0000- 0002- 9280- 9709
杂志排行

Family Medicine and Community Health的其它文章
- Cost or revenue: is diabetes prevention doomed due to misalignment of incentives?
- Variable selection strategies and its importance in clinical prediction modelling
- Identifying diabetes management opportunity areas in the USA
- Evaluation and prospect of scientific research capacity ranking for community healthcare centres in China
- Global health training in Canadian family medicine residency programmes
- Perceptions of Malaysian medical students from different academic years on primary care: a qualitative research