Therapeutic efficacy of acupuncture combined with neuromuscular joint facilitation in treatment of hemiplegic shoulder pain
2019-04-22YanHuiWeiDeChaoDuKeJiang
Yan-Hui Wei, De-Chao Du, Ke Jiang
Yan-Hui Wei, Department of Rehabilitation, Nanjing University of Chinese Medicine, Nanjing 210028, Jiangsu Province, China
De-Chao Du, Department of Rehabilitation, Nanjing Red Cross Hospital, Nanjing 210028,Jiangsu Province, China
Ke Jiang, Department of Rehabilitation Physiotherapy, Jiangsu Provincial Hospital of Integration of Chinese and Western Medicine, Nanjing 210028, Jiangsu Province, China
Abstract
Key words: Acupuncture; Neuromuscular joint facilitation; Hemiplegic shoulder pain;Visual analogue scale; Fugl-Meyer assessment; Therapy
INTRODUCTION
Stroke is a type of cerebrovascular disease with high prevalence, mortality, and onset of disability.It has become the second leading cause of death in human beings today[1].According to the statistics, the incidence of new-onset stroke in China exceeds 2 million per year[2], and its incidence is increasing year by year.With the increase in the level of social medical care, the mortality of stroke has decreased, but the disability rate of up to 80% has always been a serious burden for individuals, families,and the society.Shoulder pain is one of the common stroke sequelae, and has an incidence rate as high as 84%[3], two thirds of which occur within 4 wk to 2 mo after stroke, which is the best period for rehabilitation of stroke patients.It is often presented as a common mode of motion.However, the occurrence of hemiplegic shoulder pain (HSP) can easily affect the upper limb training, hinder the movements,and have a certain effect on the recovery of joint function, the daily living ability, and the quality of life in the patients.It also causes harm to the mental health of patients,resulting in the occurrence and aggravation of adverse psychological reactions such as depression and anxiety after stroke[4,5].
As a neurodevelopmental therapy, NJF is widely used in the treatment of orthopedic and neurological disorders in the clinical practice[6-9].In particular, it is mainly used for central nervous system diseases or orthopedic diseases, movement disorders, and pain rehabilitation.According to related studies, NJF can also be used as a rehabilitation treatment in patients with HSP.However, the research is still insufficient.The present study combined acupuncture with NJF technology to treat HSP, with an aim to provide a new treatment choice for this disease.
METERIALS AND METHODS
Participants
From January 2016 to February 2017, 40 patients with HSP were selected at the Department of Acupuncture and Rehabilitation and the Department of Neurology,Integration of Chinese and Western Medicine.
Diagnostic criteria
The criteria for traditional Chinese medicine diagnosis used in the present study were the Standards for Diagnosis and Efficacy of Stroke Diseases compiled by the State Administration of Traditional Chinese Medicine in 1996[10].
The criteria for Western medicine diagnosis used in the present study were the Guidelines for the Diagnosis and Treatment of Acute Ischemic Stroke in China published by the Cerebrovascular Diseases Group of the Chinese Medical Association Neurology Branch in 2014[11].
Inclusion and exclusion criteria
To be included, patients should meet the following criteria:(1) Diagnosed as having cerebral hemorrhage or cerebral infarction according to the diagnostic criteria of Chinese and Western medicine, and by head computed tomography or magnetic resonance imaging (MRI); (2) Aged between 35 and 85 years; (3) First seizure with a disease course of 2 wk to 6 mo; (4) Hemiplegia and shoulder pain after stroke; (5)Sober-minded, with stable vital signs, and without communication barriers or other serious disorders; and (6) Willing to receive the treatment.
Patients were excluded if they clearly met one or more of the following exclusion criteria:(1) With a history of progressive stroke or multiple episodes, or having undergone a previous thrombolysis; (2) With aphasia, sensory processing disorder, or cognitive dysfunction; (3) With pre-existing orthopedic or neurological diseases which affect upper limb functional activities such as cervical spondylosis, frozen shoulder,upper limb fracture, thalamic lesion, and peripheral nerve injury; and (4) With a history of brain trauma, tumor, or surgery, or other heart disease with atrial fibrillation or pacemaker installed.
In addition, patients who cannot complete the study and naturally dropped out during the observation period, patients who took other drugs without permission during the study, which affects the validity of efficacy, patients whose condition was unstable and whose condition was aggravated during the treatment, and patients in whom adverse reactions or other serious complications occur were also excluded.
Treatment
The 40 patients selected were numbered according to the date of the visit, and were randomly assigned to a treatment group and a control group according to the random number table method, with 20 patients in each group.
Hua Tuo brand disposable acupuncture needles (0.30 mm × 40 mm) were used as acupuncture needles in the study.Our acupuncturists mainly selected the following acupuncture points to perform the acupuncture procedure:Jianyu (LI15), punctured obliquely 0.8–1.5 inches on the deltoid muscle; Jianzhen (SI9), punctured obliquely 1–1.5 inch; Jianliao (SJ14), punctured straightly 1–1.5 inch; Tianzong (SI11), punctured obliquely 0.5–1 inch; Jianqian (EX-UE), punctured straightly 1–1.5 inches; Binao(LI14), punctured straightly 0.8–1 inch; Quchi (LI11), punctured straightly 0.5–1 inch;Waiguan (SJ5), punctured straightly 0.5–1 inch; Hegu (LI4), straightly pricked 0.5–1 inch; and Shousanli (LI10), punctured straightly 0.8–1.2 inches.We suggest using the method of inserting and twisting, mild reinforcing and attenuating acupuncture to achieve arrival of the qi.Each time the needle was left for 30 min, once a day and six times a week, for a total of three weeks.
For the control group, the following acupuncture points were selected on the affected side of the shoulder:LI15, SI9, SJ14, SI11, EX-UE, LI14, LI11, LI10, SJ5, and LI4.For the treatment group, the acupuncture treatment was the same as the control group.In addition, NJF was applied for rehabilitation training.
Patients in the treatment group were also trained to do exercises mainly involving articular surface movement including extension-adduction-internal rotation, flexionabduction-external rotation, flexion-adduction-external rotation, and extensionabduction-internal rotation.Opposite joint motion was also performed, which involved the upper limb-shoulder, including extension-adduction-internal rotation +shoulder abduction-upper rotation, flexion-abduction-external rotation + shoulder adduction-lower rotation, extension-abduction-internal rotation + shoulder abduction-above rotation, and flexion-adduction-external rotation + shoulder extension-lower rotation.
Effectiveness evaluation
Patients were assessed for rehabilitation before and after treatment.The Clinical Diagnosis and Treatment Guide, Physical Medicine and Rehabilitation compiled by the Chinese Medical Association in 2005[12]was used to evaluate the functional activity of the shoulder joint.The relevant rehabilitation indexes were used to evaluate the rehabilitation effect of HSP in the following four aspects:(1) Visual analogue scale(VAS); (2) Passive range of shoulder joints (PROM); (3) Barthel index score (BI); and(4) Fugl-Meyer assessment (FMA) score for upper limb motor function.
Statistical analysis
Statistical analyses were performed on relevant clinical data with IBM SPSS Statistics 20.0.Student’st-test was used for the data measured which conform to a normal distribution.Student’st-test was also used to compare the difference before and after treatment.Independentt-test was used to compare the difference between groups.χ2test was used to compare the difference in quantitative data, and nonparametric test was used for data which do not conform to a normal distribution.P< 0.05 indicated that there was a statistical difference.
RESULTS
Patient characteristics
There was no significant difference in age or duration of disease between the treatment group and the control group (P> 0.05, Table 1).
VAS scores
Table 2 shows that there was no significant difference in VAS scores between the two groups before treatment (P> 0.05).However, after the treatment, the VAS scores were significantly reduced in the two groups (P< 0.05).The VAS score was significantly better in the treatment group than in the control group (P< 0.05).
PROM scores
Table 3 shows that there was no significant difference in the PROM scores between the two groups before treatment (P> 0.05).However, after the treatment, the PROM scores were significantly increased in the two groups (P< 0.05).The PROM score was significantly better in the treatment group than in the control group (P< 0.05).
FMA scores
There was no significant difference in FMA scores between the two groups before treatment (P> 0.05).However, after the treatment, the FMA scores of the two groups were significantly increased (P< 0.05).The FMA score was significantly better in the treatment group than in the control group (P< 0.05, Table 2).
BI scores
There was no significant difference in BI scores between the two groups before treatment (P> 0.05, Table 2).After the treatment, the BI scores of the two groups were significantly increased (P< 0.05).However, there was no significant difference in BI scores between the two groups after the treatment (P> 0.05).
DISCUSSION
Acupuncture has a positive effect on shoulder joint activity in patients with hemiplegia[13].The acupuncture points we selected based on the disease are mainly on the extensor muscle.For example, LI15, SI9, SJ14, EX-UE and LI14 are located on the deltoid muscle; SI11 is located on the infraorbital muscle; LI11 is located on the radial extensor muscle.LI4 is located between the 1st and 2nd metacarpal bones, and at its deep layer there is the elbow extensor muscle.The acupuncture points are mainly on antagonistic muscle groups, the upper limbs contain lots of extensor muscle groups,and the lower limbs contain lots of flexor muscle groups.The acupuncture points near the extensor muscle group can improve muscle strength[14].This helps to improve motor dysfunction and limb function activities in patients after stroke.The present study found that acupuncture has a certain effect on shoulder mobility and upper limb motor function in patients with hemiplegia.
Acupuncture can change the microenvironment of damaged muscles[15-20].Moreover, it promotes the recovery of muscle fiber structures by improving arrangement of filament in muscle, eliminating mitochondrial swelling, dilatingsarcoplasmic reticulum and so on; it also improves intracellular calcium metabolism by promoting cell membrane sodium and calcium exchange, promotes the recovery of resting potential of skeletal muscle, accelerates muscle regeneration by promoting the proliferation of muscle satellite cells, and accelerates polymerization and recombination by inhibiting myosin degradation.By inhibiting the production of myogenic IL-6, it has an effect on skeletal muscle inflammation.Acupuncture can play a protective role in the treatment of muscle injury through a series of microstructural changes of skeletal muscle.For the effect of acupuncture on pain relief, studies[21]have shown that acupuncture can not only activate the endogenous opioid peptide system in the body, result in the release of related transmitter products, increase pain threshold, and relieve pain, but also stimulate the transmission of pain-induced fibers and C fibers through the excitatory and central nervous system inhibition of the spinal cord.This may ultimately influence the interaction of various functional intervals of the cortex and achieve analgesic purposes, result in the release of amine and enkephalin-like neurotransmitters, and promote the decline of striatal adrenaline and cortical adrenaline[22].A study shows that electro-acupuncture for rabbits at LI10, LI4,ST36, and LI14 can evoke the caudate nucleus and increase the pain threshold[23].Using fMRI to observe the brain function image of the patients after needling at LI4 on the right side, these authors found that the signal intensity of many functional areas of the brain can be changed by needling.It was also observed that the signal intensity of the gray matter and lenticular nucleus on the left side was enhanced, and the signal intensity of the occipital lobe and anterior cingulate gyrus on both sides was weakened[24].Acupuncture alone and acupuncture combined with NJF for HSP can achieve appreciated clinical efficacy.

Table 1 Comparison of basic conditions between the two groups
NJF is a movement pattern that is diagonal and spiral in nature and applies the concave and convex rule in joint mobilization.It is a new type of exercise therapy that can achieve therapeutic effects on joints, muscles, and nerves[25,26].Joint pain and limited activity, from the perspective of anatomy, generally involve internal or external causes of joint capsule.The internal capsule includes joint capsule, ligament,bone, and articular cartilage.The external joint capsule mainly includes skin, muscle,tendon, and nerve factors, and hemiplegia and shoulder pain are just a kind of disorders caused by changes in joint structure stability and tissue.Shoulder joint is a triaxial joint.Different from head and the joint iliac crest, it can perform multidirectional movement such as flexion, extension stretching, and rotation on three mutually perpendicular axes.In terms of the concave and convex rule, the axis for the rotation at the shoulder joint is on the humerus, and the movement of the articular surface is opposite to the direction of bone movement.In the normal mode of motion,patients with hemiplegia will exhibit flexor-based mode motion for their upper limbs,mainly manifested as retraction and pull-up of scapular band, extension, abduction,and rotation of the shoulder joint, flexion of the elbow joint, forearm rotation, wrist flexion, and finger flexion and adduction.Generally, shoulder pain makes the patient unable to lift the upper limb.Long-term pain can affect the patient’s psychology.Loss of scapular rhythm and inadequate external rotation of the humerus are the major mechanism for shoulder pain[27].NJF can assist and resist the movement of the articular surface, and add spiral diagonal motion, which can reduce joint impact and pain, correct force line, and improve motion ability.The muscle shuttle can reflexively contract by extension.Traction can increase joint clearance and increase mobility[28].Extrusion can make the joint gap smaller and increase joint stability.Active resistance motion can promote the excitability of proprioceptors and promote the production of muscle, muscle strength, and tendon tension[29,30].This study found that acupuncture combined with NJF has clinical efficacy in the treatment of limb movement disorders and joint pain in patients with hemiplegia.

Table 2 Comparison of scores between the two groups
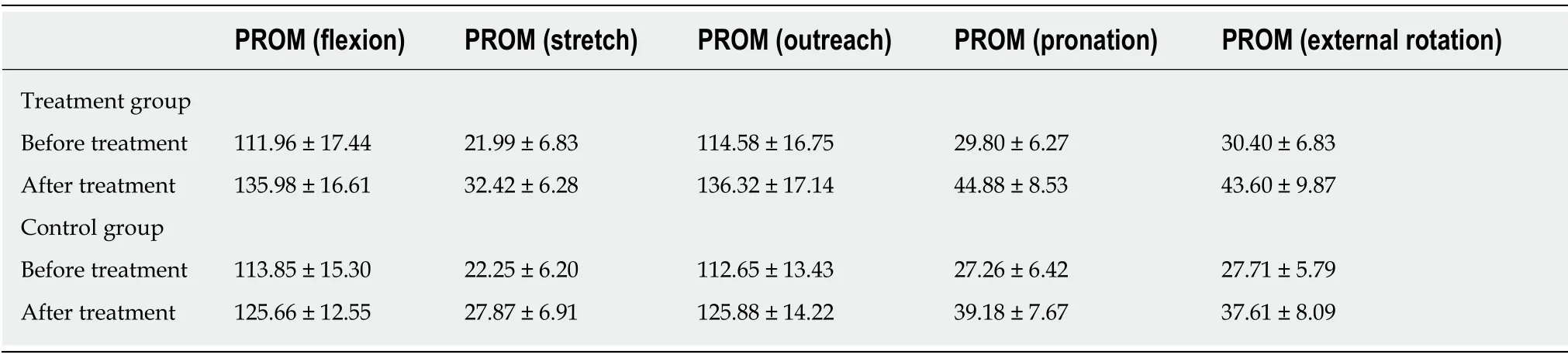
Table 3 Passive range of motion scores in the treatment group vs the control group
ARTICLE HIGHLIGHTS
Research background
Hemiplegic shoulder pain (HSP), a common sequela of stroke, causes damage to patients’movements and quality of life.Both traditional acupuncture and neuromuscular joint facilitation(NJF) help alleviate shoulder pain and inflammation associated with bursitis and/or tendonitis.However, the combination of the two therapies was seldom applied in the clinical practice.
Research motivation
The present study combined acupuncture with NJF technology to treat HSP, with an aim to provide a new treatment choice for this disease.
Research objectives
To study whether the efficacy of acupuncture combined with NJF is superior to acupuncture alone.
Research methods
Forty patients with HSP were randomly divided into a treatment group and a control group.The treatment group was treated with acupuncture combined with NJF and the control group was treated with acupuncture alone.In addition, patients in the treatment group were also trained to do exercises including articular surface movement and extension-abduction-internal rotation.The efficacy of the therapies was assessed by using the visual analogue scale (VAS), Fugl-Meyer assessment (FMA), Barthel index (BI), and passive range of motion (PROM) before and after the training.
Research results
After the treatment, the scores of VAS, FMA, and PROM were better in patients receiving neuromuscular joint facilitation combined with acupuncture than in patients only receiving acupuncture.However, there was no significant difference in BI scores between the two groups after the treatment.
Research conclusions
Both acupuncture alone and acupuncture combined with NJF in the treatment of HSP are effective, and can improve the clinical symptoms of patients.Acupuncture combined with NJF can improve the upper limb motor function, relieve pain, and increase joint mobility in patients with HSP.The combination therapy is better than acupuncture alone.However, there is no significant difference in improving the score of patients’ self-care ability.
Research perspectives
Multidisciplinary treatment plan should be further studied in patients with HSP.
杂志排行

World Journal of Clinical Cases的其它文章
- Overview of organic anion transporters and organic anion transporter polypeptides and their roles in the liver
- Value of early diagnosis of sepsis complicated with acute kidney injury by renal contrast-enhanced ultrasound
- Value of elastography point quantification in improving the diagnostic accuracy of early diabetic kidney disease
- Resection of recurrent third branchial cleft fistulas assisted by flexible pharyngotomy
- Comparison of intra-articular injection of parecoxib vs oral administration of celecoxib for the clinical efficacy in the treatment of early knee osteoarthritis
- Celiomesenteric trunk:New classification based on multidetector computed tomography angiographic findings and probable embryological mechanisms