Intracranial ricocheted-bullet injuries: An overview and illustrative case
2018-11-19MohammedMaanAbdulAzeezAliAdnanDolacheePadillaZambranoHuberMendozaFlorezRomarioHaithamAhmedObaidAlaaArakwaziMustafaAltaweelSamerHoz
Mohammed Maan AbdulAzeez, Ali Adnan Dolachee, Padilla-Zambrano Huber, Mendoza-Florez Romario, Haitham Ahmed Obaid, Alaa H. Arakwazi, Mustafa M. Altaweel, Samer S.Hoz
1College of Medicine/University of Baghdad, Baghdad, Iraq
2Department of Neurosurgery, College of Medicine, AL-Qadisiyah University, Iraq
3Neurosurgery Department, Neurosurgery Teaching Hospital, Baghdad, Iraq
4Centro de Investigaciones Biomédicas, Cartagena Neurotrauma Research Group Research Line, Faculty of Medicine, University of Cartagena, Cartagena de Indias, Colombia
Keywords:Trauma Head Injury Ricocheted
ABSTRACT The impact of a bullet by firearm is a mortal entity that in recent years has been on the rise due to the increase in crime, confrontations, among other acts of violence. Brain injuries by firearm account for 33.3% of all fatal injuries from this type of weapon. This resulted in a significant number of disabilities with its burden cost at a global level. The types of bullet injuries to the head include: penetrating (inlet without outlet), perforating (through and through), tangential (not enter the skull, causing coupe injury), ricochet (intracranial bouncing of bullet) and careening (rare, enter skull but not brain, runs in the subdural space). There are several situations that can occur once the bullet enters the body or into the intracranial cavity.Unmatched association of the bullet trajectory with the final position of the bullet within the body raise the suspicion for additional phenomena involvement, this can be explained by either internal bullet ricochet or internal bullet migration. The former usually represents an active movement and the latter is a passive movement. Intracranial ricocheting of bullets forms up to 25% of all penetrating bullet injuries to the skull. Such bullets types are commonly tumbling and have an unpredictable trajectory. The surgical management for intracranial bullet injury developed over decades from the time of Harvey Cushing and the World War I till the present.Now, the accepted intervention ranges from simple wound care to a proper surgery that includes hematoma evacuation, removal of only accessible bone fragments and foreign bodies, dural repair and wound debridement with or without decompressive craniectomy. Also, intracranial pressure monitoring is generally indicated. We reported a thirty-three years old male, victim of homicidal bullet injury to the head, presented with Glasgow Coma Scale score of 8 (best eye response: 2, best motor response: 4, best verbal response: 2), upon examination a right parietal(near vertex) inlet without outlet was found. The poor prognostic factors in this patient included bi-hemispheric involvement, associated acute subdural hematoma with interhemispheric extension, ricochet type of injury and effacement of sulci. Intracranial ricocheted-bullet injury is a special entity of bullet injury to the head with its particular ballistics and management that deserve highlighting by the trauma team to gain fluent treatment and better outcome.
1. Introduction
Generally, the bullet injuries are homicidal, suicidal, or accidental.These are usually occurring in the third and fourth decades with more male to female ratio in homicidal than in suicidal[1]. The impact of a bullet by firearm is a mortal entity that in recent years has been on the rise due to the increase in crime, confrontations,among other acts of violence[2]. Brain injuries by firearm account for 33.3% of all fatal injuries from this type of weapon[3]. This resulted in a significant number of disabilities with its burden cost at a global level[4].
The bullet injury can be categorized into high-velocity (more than 300 meters per second) and low-velocity injuries. In general, the high-velocity injuries are usually associated with shockwaves and cavitation while, the low-velocity is associated with a higher risk of infection.
The types of bullet injuries to the head include: penetrating (inlet without outlet), perforating (through and through), tangential (not enter the skull, causing coupe injury), ricochet (intracranial bouncing of the bullet) and careening (rare, enters the skull but it does not enter the brain, runs in the subdural space)[5].
The firearms and ammunition are more available and widespread,especially in countries where celebratory firing is common[6].During the Asian cup in 2007, there were widespread firing of bullets as people celebrating the Iraqi football team winning, three civilians were killed in Baghdad from falling bullet injuries to the head[7]. Studies on gravitational (falling)-bullet injuries report several intracranial ricocheting injuries, although these are described more in the news media than in medical literature[8].
2. Ricocheted bullets vs. intracranial ricocheted bullet
The bullet trajectory is either directly hitting the target or indirectly through bouncing over the intermediate target. The latter is called“ricocheting bullet” which occurs either outside the body (hitting the ground for example before reaching the body) or ricocheting inside the body (hitting a bone within the body then bounces). Our focus in this article is the ricocheted bullet inside the skull, describing its ballistics and management as compared with other types of bullet injuries to the head.
3. Intracranial ricocheted bullet
There are several situations that can occur once the bullet enters the body or into the intracranial cavity. Unmatched association of the bullet trajectory with the final position of the bullet within the body raise the suspicion for additional phenomena involvement,this can be explained by either internal bullet ricochet or internal bullet migration. The former usually represents an active movement and the latter is a passive movement[9]. Intracranial ricocheting of bullets forms up to 25% of all penetrating bullet injuries to the skull[3]. Such bullets types are commonly tumbling and have an unpredictable trajectory.
3.1. Ballistics of intracranial ricocheted bullet
The bullet once fired can be deflected by contact with an external surface or object before striking at its destination, and it is known as a "rebound bullet". This is equivalent to what happened inside the organs, where it can hit with one or several compact structures causing abrasions and bruises in its impact. In the cranial vault, a rebound of the bullet may occur and it is known as "billiard ball effect", generating a tortuous and unexpected course in which the bullet is deflected by striking obliquely[10]. When the bullet penetrates the cerebral parenchyma, the trajectory of it increases in size due to the deformity and the fall of the projectile. However, in some cases, there is no increase but a conical shape that is attributed to the maximum energy at the impact site. Once the bullet enters the cranial vault, it can deviate contralaterally to the internal surface of the skull or in some cases a rebound can occur again, generating another migration in the cerebral parenchyma and generating metallic fragments that can be observed at the impact site[11].
The bullet at the moment of impact presents an angle of incidence,which is formed by the trajectory of it before contact with the target surface. The bullets bounce off their target because they hit the surface at a smaller (shallow) angle than the critical angle of the target. This last angle is determined by the speed of the bullet, its composition and the nature of the surface[3,12].
When the bullet makes contact with the skull, it generates the introduction of bone particles in the brain, which are distributed following the path of the bullet, thus generating an irregular appearance. Sometimes, these fragments can follow routes different from the one traced by the bullet. These characteristics help us determine, at the time of a surgical procedure, what is the direction of the shot, as well as its entry and exit. Similarly, when a bullet enters the brain, it can generate pressure waves that are transmitted and possibly cause fractures in the skull. These fractures can occur anywhere, especially at the entrance of the bullet and at the base of the skull[3].
There are four aspects to consider to determine if a bullet will be retained or not: the composition of the bullet, the caliber of the weapon, the range and the entry site[3]. The larger the caliber of the weapon, the more likely it is to go through the skull. In addition,distant wounds produce only penetration without perforation, unlike contact wounds where the perforation of the skull is more frequent.On the other hand, the bullets that impinge through the temporal bone leave with greater frequency than those that enter through the occipital bone, this due to the thickness of the lobes of the skull. The bullet bounce is suspected more in low velocity, small caliber, round nose and Jacketed bullets with lead-core injuries[3,13,14].
Rebound types: The most common type of rebound is characterized by a bullet that crosses the cerebral parenchyma, striking the inner layer of the skull on the opposite side and distributing cortically or subcortically parallel to the skull, generating a superficial and shallow trajectory. Another type of rebound less frequent is in which the bullet at the moment of impacting the inner layer of the skull of the opposite side bounces back to the brain with an acute angle with respect to its initial trajectory (Figure 1)[2,13,15]. As a bullet follows a tangential path, the damage to the brain may be surprisingly extensive because of laceration of arteries and veins in the subarachnoid space. Intracranial bullet ricochet is not restricted to bony surfaces; it may also occur from other firm structures such as the falx and tentorium[13]. In very rare instances the bullet exits through its entrance wound after ricocheting off the inner table of the skull[16].

Figure 1. Intracranial ricocheted-bullet types (predicted pathways).
3.2. Presentation and initial management of intracranial ricocheted bullet
Along with other types of bullet injury to the head, the intracranial ricocheted bullet injuries usually result in signs of increased intracranial pressure with an associated variable degree of herniation syndromes[17]. When initial radiographic findings of the brain tissue carried on after these types of wounds, it is common to see contusions in the entrance area possibly influenced by the contact of the bone with the brain at the moment of impact; this is observed in 50% of cases. Signs of intracranial hypertension, such as coneshaped cerebellar tonsils in the foramen magnum, may be present in all cases involving the brain. The pressure exerted on the brainstem as a result of this deformation can be fatal[3].
It is important to observe in the computed tomography the exact location of the bullet to evaluate the migration of this in the cerebral parenchyma, which can occur in approximately 4% of cases. The determination of the trajectory allows to understand the mechanisms of injury and obtain a prognosis of the patient. It has been found that the migration of the bullet occurs frequently if it penetrates the ventricular system or if there is a necrotic lesion in the brain[11].
A well-trained and fully prepared team is of paramount importance for effective management and better patient outcome. Initial steps to decrease intracranial pressure should be contemplated and carried in association with the stabilization of the patient’s vital signs to be ready for earlier brain CT scan and definitive treatment[18].
3.3. Surgery for intracranial ricocheted bullet
The surgical management for intracranial bullet injury developed over decades from the time of Harvey Cushing and the World War I till the present. Now, the accepted intervention ranges from simple wound care to a proper surgery that includes hematoma evacuation,removal of only accessible bone fragments and foreign bodies,dural repair and wound debridement with or without decompressive craniectomy[19]. Also, intracranial pressure monitoring is generally indicated[20].
Indications for surgery: The major indications for proper surgery include Glasgow coma scale score of six or more, significant intracranial hematoma and pupils’ asymmetry[21].
Surgical procedures: The main surgical steps include: large skin flap, large hemicraniectomy when indicated, consider external ventricular drain if the bullet trajectory involves the ventricles,irrigate generously with antibiotic solution, effective and boggy duroplasty is of paramount importance, removal of all accessible devitalized tissue along with bone debris and accessible foreign bodies, elevation of depressed fractures, and antimicrobial prophylaxis coverage[18,22-24].
3.4. Complications and postoperative management of intracranial ricocheted bullet injury
Complications are categorized as either early (within 7 days) or late (more than 7 days). Early complications include hemorrhage,vascular injury, infarction, and edema, while late complications include infections, hydrocephalus, cerebrospinal fluid fistulas,posttraumatic epilepsy and spontaneous bullet migration[5].
Postoperative management in the intensive care unit should consist of maintenance of cerebral perfusion pressure, antibiotic and antiepileptic prophylaxis, early tracheostomy, gastrostomy and deep venous thrombosis preventive measures[18].
3.5. Outcome
The significant poor prognostic factors include multilobar,transventricular, bi-hemispheric, Glasgow coma scale score of 4 or less and diabetes insipidus. A rather favorable outcome can be expected when injuries associated with the following factors: young age, Glasgow coma scale score more than 5, isolated injury to the head, hemodynamically stable, non-eloquent areas involved, and early management in specialized neurosurgery center[5,18,24].
4. Illustrative case
Thirty-three years old male a victim of homicidal bullet injury to the head, presented with Glasgow Coma Scale score of 8 (best eye response:2 best motor response:4 best verbal response:2), upon examination a right parietal (near vertex) inlet without outlet was found.
Based on the brain CT scan shown in (Figure 2), the type of bullet injury to the head is penetrating bullet injury in the right parietal cortex with fragmentation and ricocheting along the contralateral inner table of the skull to be settled above the left anterior cranial fossa floor. It also shows intracranial bone chips, small acute subdural hematoma, and tract hematoma.
One hour from the accident, surgical intervention was contemplated through debridement of the inlet with the removal of easily accessible bone and metallic fragments that is done through an extension of the already present wound in a lazy "S" pattern. Then removal of accessible bullet parts and bone chips via the right parietal craniectomy. Pericranium was used for duroplasty upon closure. Patient, unfortunately, died in the neuro-intensive care unit 17 days from admission after initial postoperative improvement.The cause of death was a pulmonary embolism. The poor prognostic factors in this patient include bi-hemispheric involvement, associated acute subdural hematoma with interhemispheric extension, ricochet type of injury and effacement of sulci.
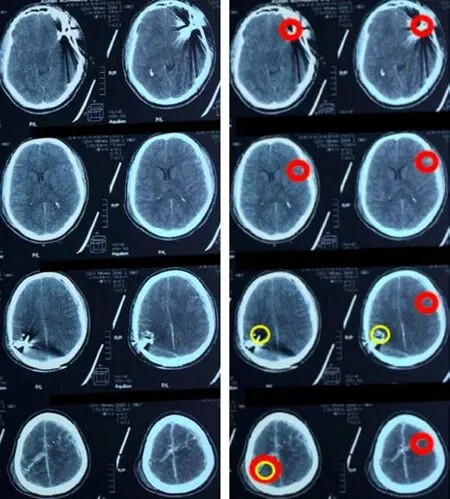
Figure 2. Brain CT scan of intracranial ricocheted-bullet injury.
5. Conclusions
The intracranial ricocheted-bullet injury is a special entity of bullet injury to the head with its particular ballistics and management that deserve highlighting by the trauma team to gain fluent treatment and better outcome.
Conflict of interest statement
We declare that we have no conflict of interest.
杂志排行

Journal of Acute Disease的其它文章
- Comparison of risk factors associated with sepsis between road traffic injuries and non-road traffic injuries in ICU patients with severe trauma
- Efficiency of EBUS-TBNA for diagnosing benign and malignant lymphadenopathy
- Inhibiting effect of immunoeffector cells induced by denderitic cells vaccine on growth of PC3 and BEL7402
- Survival rate among tuberculosis patients identified in south of Iran,2005-2016
- Think muscle; Think rhabdomyolysis
- Intracranial hematoma development following thrombolysis inpatients suffering with acute myocardial infarction: Management strategy