Effects of core stability exercise on rehabilitation in stroke patients with hemiplegia: a meta-analysis
2018-08-27TingTingLiuMengJieLeiYaQianLiuLiNaMengChangDeJin
Ting-Ting Liu, Meng-Jie Lei, Ya-Qian Liu, Li-Na Meng, Chang-De Jin*
1Tianjin University of Traditional Chinese Medicine, School of Postgraduate, Tianjin, China.
Abstract Objective: To evaluate the effects of core stability exercise (CST) on rehabilitation in stroke patients with hemiplegia.Methods: Randomly controlled trials about the effects of CST on rehabilitation in stroke patients with hemiplegia were searched in the database, including PubMed, Embase, Web of Science, Cochrane Library, CNKI, Wanfang, CBM and VIP. Search terms include “core stability training / core stability exercise / core stabilization training / core stabilization exercise / core strength training / core strength exercise” and “stroke / brain ischemia / cerebral infarction / cerebral hemorrhage / intracranial thrombosis / brain hemorrhage / cerebrovascular disorder / cerebrovascular accident,cerebrovascular disease / hemiplegia / hemiparesis / stroke rehabilitation”. Study screening, data extraction and quality assessment were conducted by two researchers independently. Data was analyzed using RevMan 5.3 software. Results:Totally 11 studies and 704 patients were included with 352 patients in experiment group and 352 in control group.Results of meta-analysis showed that combination of CST and conventional rehabilitation had better effects on trunk control [MD = 10.44, 95% CI (8.83-12.04), P < 0.001], banlace [MD = 5.6, 95% CI (4.81-6.39), P < 0.001], activities of daily living [MD = 12.06, 95% CI (7.65-16.46), P < 0.001], ambulation functional [MD = 0.72, 95% CI (0.32-1.12), P <0.001] and walking speed [MD = 3.39, 95% CI (2.03-4.76), P < 0.001] than conventional rehabilitation, but there is no clear difference on walking stride [MD = 2.52, 95% CI (-0.25-5.29), P = 0.07] between two groups. Conclusion: CST together with conventional rehabilitation can better improve trunk control, banlace, activities of daily living, ambulation functional and walking speed in stroke patients compared with conventional rehabilitation, but can not make the walking stride better significantly. However, since the conclusion of this meta-analysis was drawn based on middle quality RCTs,future high quality researchs should be conducted to confirm its positive intervention effects.
Key words: Stroke, Hemiplegia, Core stability exercise, Rehabilitation, Meta-analysis
Introduction
Stroke has the characteristics of high morbidity, high disability and high mortality, which seriously threatens people's life and health. With the acceleration of social aging and urbanization, the incidence of stroke in China is still rising at an annual rate of 8.7% [1]. After stroke,about 70%-80% of patients will still have different degrees of dysfunction, which seriously affects their quality of life [2]. Prompt and appropriate rehabilitation measures can promote recovery of limb function and mobility after stroke [3,4]. Huangdineijing (B.C. 220~211,Han Dynasty) recorded that autonomously exercise combined with massage can relax the pain of sudden illness [5]. Taipingshenghuifang (A.D. 220~589, Southern and Northern Dynasties) came up with that the employment of massage in combination with limb movement coincided with modern rehabilitation measures in the treatment of stroke hemiplegia [6]. In recent years,the core stability training (CST), defined as a physical training focused to improve trunk and hip control, has been gradually introduced into the rehabilitation field [5].It is a simple, economical, and suitable method for home rehabilitation. At present, some studies have shown the effectiveness of CST, but the research conclusions are not consistent [7]. In addition, there are no systematic review and meta-analysis about the effects of CST on rehabilitation of stroke patients with hemiplegia now.Therefore, we conduct this meta-analysis to evaluate the clinical effect of CST on rehabilitation of stroke patients with hemiplegia in order to provide a theoretical basis for clinical application.
Methods
Search strategy
We searched for relavent articles published in the PubMed, Embase, Web of Science, Cochrane Library,China National Knowledge Infrastructure, Wanfang,CBM and VIP databeses up to January 2018. Search terms include "core stability training / core stability exercise / core stabilization training / core stabilization exercise / core strength training / core strength exercise /core stabili model / core stabili program", and "stroke /brain ischemia / cerebral infarction / cerebral hemorrhage/ intracranial thrombosis / cerebral infarc / brain infarc /brain hemorrhage / cerebrovascular disorder /cerebrovascular accident / cerebrovascular disease /hemiplegia / hemiparesis / stroke rehabilitation”. A combination of topic words and free words was used.Authors were contacted to obtain more relevant data not presented in the original articles. There was no language restriction on the search of relavent articles.
Selection criteria
An article would be included in our meta-analysis if it met the following selection criteria: (1) Study type was randomized controlled trial; (2) Study subjects were stroke patients with clearly diagnosis criteria, whose age was more than 18 years. Subjects’ stroke duration was within 6 months, but the types of stroke were not limited;(3) Intervention: the experimental group used CST on the basis of routine rehabilitation, while the control group used routine rehabilitation only; (4) Outcome measures:the primary outcomes were trunk control, balance ability,daily activities and walking fuction. The secondary outcomes were step length and walking speed. Test method and evaluation standard for each outcome were shown in Table 1.
Exclusion criteria
(1) Repeatedly published articles; (2) Studies that were published in abstracts only; (3) Study subjects had other severe organ dysfunctions such as heart, lung, liver, or kidney; (4) Baseline data were inconsistent between the intervention group and the control group; (5)Interventions were sling exercise training; (6) Outcome datas were incomplete and were still not available by contacting its’ author.
Literature screening and data extraction
Two evaluators screened all search articles according to the inclusion and exclusion criteria of the literature independently who had received systematic evidence-based medicine training. For the studies that met the inclusion criteria, two evaluators extracted data using a unified data extraction table independently. If there was a disagreement, it would be determined through discussion with the third evaluator. Data extraction included the following information: first author, year of publication, study object (sample size, age, gender, types of stroke, duration of stroke), intervention (intervention content, time, frequency, control content) and outcome measures.
Quality evaluation
The Cochrane Randomized Controlled Trial Bias Risk Tool was used to evaluate the quality of the included literature [12]. This method mainly evaluates the original studies from seven aspects, which including random sequence generation, allocation concealment, blinding of research subjects and researchers, blindng of outcome measure, incomplete outcome data, selective reporting,and other biases. The two evaluators independently made judgments on each aspect of the literature with high risk of bias, low risk of bias, or unclear bias. If there were any inconsistencies, it would be discussed and resolved by the third evaluator. If the study fully satisfies the above aspects, it is rated as A grade; if partially satisfing, it is rated as B grade; if not satisfing at all, it is rated as C grade.
Statistical analysis
All statistical analyses were performed using RevMan 5.3 software [13]. Firstly, clinical heterogeneity or methodological heterogeneity among the included studies should be considered. Then under the condition of clinical and methodological homogeneity, use the Q test and I2test to perform statistical heterogeneity tests. When P >0.1 and I2< 50%, which suggested that there was no statistical heterogeneity in each study, we would use fixed effect model for analysis. When P ≤ 0.1 and I2≥50%, which suggested that there was statistical heterogeneity among studies, we would use subgroup analysis or sensitivity analysis to find out the source of heterogeneity as much as possible. If source of heterogeneity can not be eliminated still, then the random effect model would be adopted [12]. Mean difference or standardized mean difference and its 95% confidence interval were used as the effect indicators of the measurement data of this study.
Results
Searching Results A total of 1462 publications were preliminarily identified after systematically searching the aforementioned databases based on our search strategy using different search term combinations. All searched literatures were managed using Endnote X7 software,during which, 466 duplicated articles were removed, 959 articles that did not meet the inclusion criteria were excluded after reading the title and abstract, and 26 articles that did not meet the inclusion criteria were excluded after reading the full text. Finally, 11 randomized controlled trials were included in the study.The detailed selection process is shown in Figure 1.
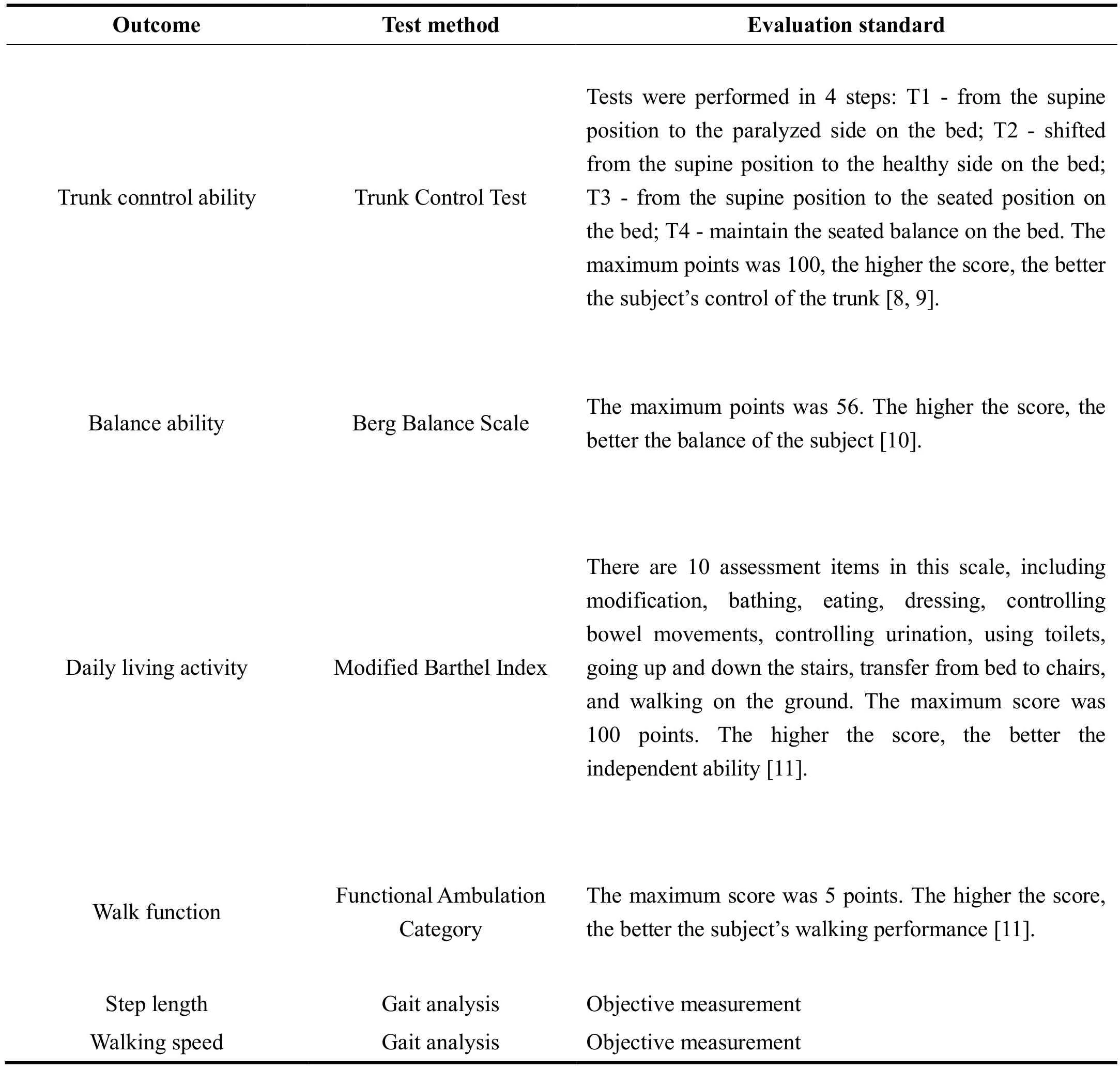
Table 1 Test method and evaluation standard for each outcome
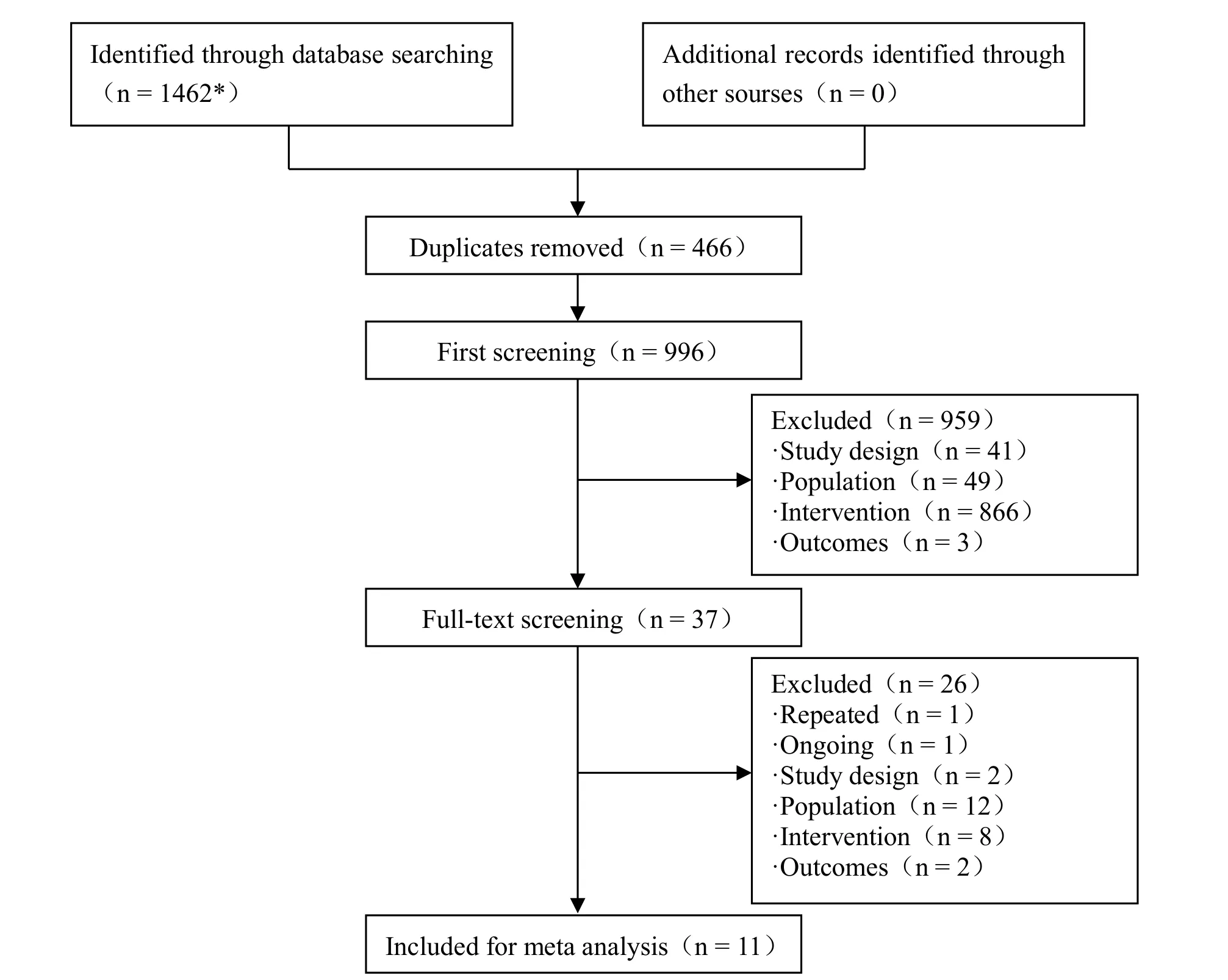
Figure 1 Prisma flowchart of selection process of the meta analysis
Characteristics of the included studies
A total of 11 randomized controlled trials with 704 stroke patients were included in the meta analysis finally, which published in 2012-2017. Of the 704 patients included in this study, there were 417 cerebral infarction patients, 269 cerebral hemorrhage patients and 56 mixed patients. The sample size of the intervention group and the control group were all 352 cases respectively. The disease duration of all the patients was within 6 months. The intervention was CST on the basis of conventional rehabilitation therapy and intervention time was 4-8 weeks. The control group used only conventional rehabilitation therapy, which included drug therapy,traditional physical therapy, exercise therapy,occupational therapy, electrical stimulation,center-of-gravity training, and neurodevelopment therapy.All 11 studies included were Chinese literature. The characteristics of the eligible studies are shown in Table 2.
Quality assessment of included studies
Nine of the 11 randomized controlled studies [14-18, 20,22-24] correctly reported random sequence generation methods and processes, but all studies did not report allocation concealment. Due to the particularity of the study, it is difficult to implement blinding methods for the implementers and patients. Therefore, 10 studies [14, 15,17-24] were rated as high risk of bias in this regard.Although Bai’ study [16] did not implement the blinding method for researchers and patients, its outcome (step length and walking speed) were measured by objective instruments and subjectively influenced little by individuals, so we rated it as low risk. There were six studies [14, 16, 17, 19, 21, 24] which reported the blinding of outcome measures. All studies did not have withdrawing or missing cases, and there was no obvious alternative reporting and other biases. In terms of the overall quality of the literature, the quality of the 11 studies included was all Grade B. The specific methodological quality assessment of the study was shown in Figure 2 and Figure 3.
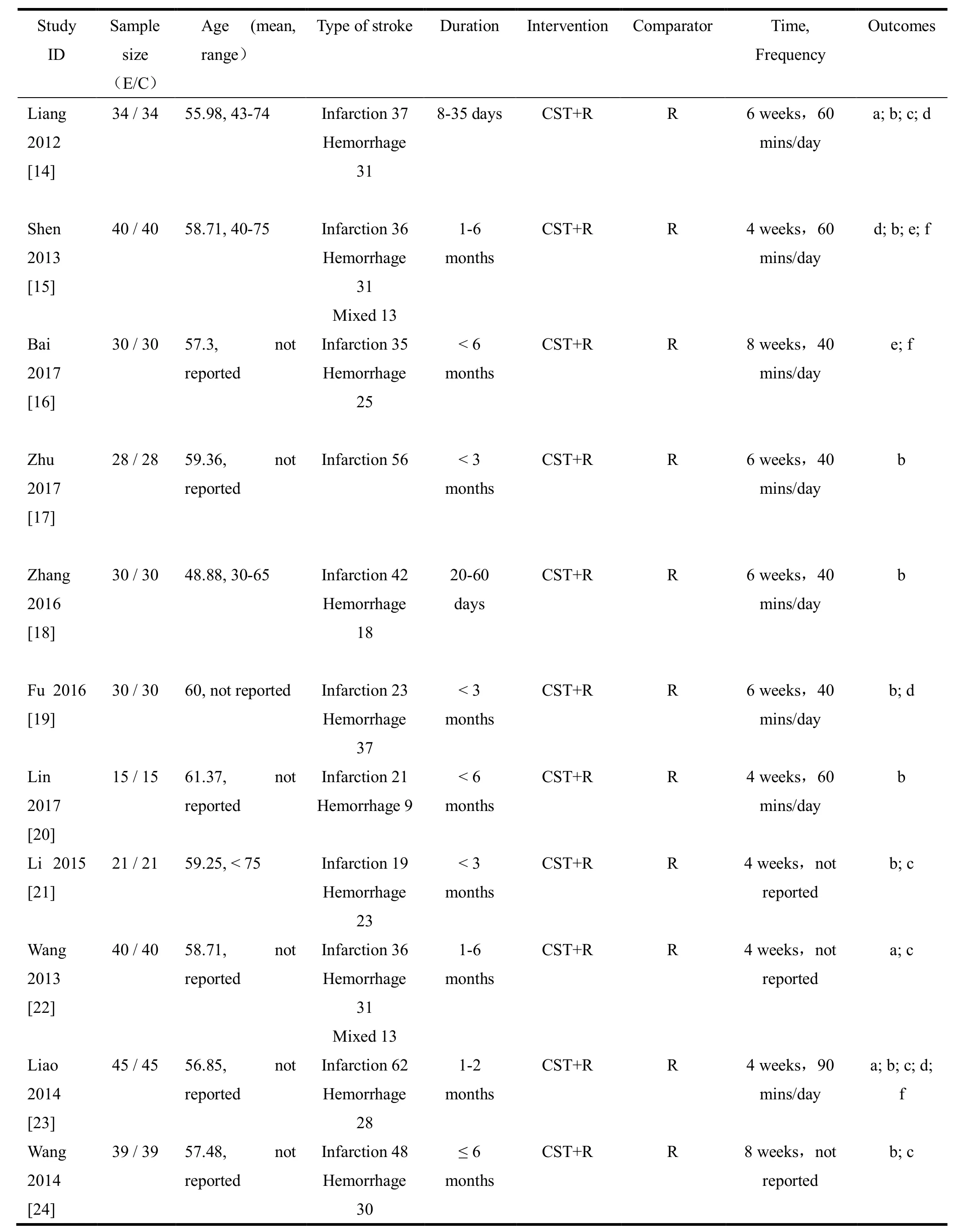
Table 2 Characteristics of the included studies

Figure 2 Risk of bias graph of included studies

Figure 3 Risk of bias summary of included studies

Figure 4 Effects of core stability exercise on trunk control

Figure 5 Effects of core stability exercise on balance ability

Figure 6 Effects of core stability exercise on daily life activities
Meta-analysis results and sensitivity analysis
Trunk control Three studies [14, 22, 23] reported this outcome measures. Statistical heterogeneity between the three studies was not obvious (P = 0.17, I2= 44%), so a fixed effect model was conducted. The results showed that the ability of trunk control in the CST group was better than that of the conventional rehabilitation group[MD = 10.44, 95% CI (8.83-12.04), P < 0.001] (Figure 4).
Balance ability Nine studies [14, 15, 17-21, 23, 24]reported the patient's balance ability. Heterogeneity test showed that there were statistical heterogeneity across the 9 studies (P < 0.01, I2= 80%), so a sensitive analysis was conducted by excluding individual studies one by one,which revealed that the baseline balance of the subjects included in Liao's study [23] was quite different from other studies and was the main source of heterogeneity.Therefore, we only effected the other 8 studies (P = 0.27,I2= 20%) and adopted the fixed-effect model. The results showed that the balance stability of the CST group was better than that of the conventional rehabilitation group[MD = 5.6, 95% CI (4.81-6.39), P < 0.001] (Figure 5).
Daily life activities A total of 5 studies [14, 21-24]reported the daily living activities of patients. Statistical heterogeneity existed among the five studies (P = 0.08, I2= 51%), and specific sources of heterogeneous were not found. So a random effect model was used for statistical integration. The results showed that the activities of daily living in the CST group were superior to those in the conventional rehabilitation group [MD = 12.06, 95% CI(7.65-16.46), P <0.001] (Figure 6).
Walk function A total of 4 studies [14, 15, 19, 23]reported the patient's walking function. Statistical heterogeneity existed among the four studies (P < 0.01, I2= 88%) and specific sources of heterogeneous were not found. So statistical integration was performed using a random effect model. The results showed that the Holden walking function grading was better in the CST group than in the conventional rehabilitation group [MD = 0.72,95% CI (0.32-1.12), P < 0.001] (Figure 7).
Step length Two studies [17, 18] reported the patient's step length. After analysis of the two studies, there was no statistical heterogeneity (P = 0.9, I2= 0%), so a statistical consolidation was performed using a fixed effect model.The results showed that the step length of patients in the CST group was not significantly different from that of the conventional rehabilitation group [MD = 2.52, 95% CI(-0.25-5.29), P = 0.07] (Figure 8).
Walking speed A total of six studies reported the patient's walking speed. Three of the studies [15, 16, 23]reported the speed of free walking, and there was no statistical heterogeneity in them (P = 0.2, I2= 39%).Therefore, statistical analysis was performed using a fixed effect model. It was shown that the free walking speed of patients in the CST group was higher than that of the conventional rehabilitation group [MD = 3.39, 95%CI (2.03-4.76), P < 0.001]. The other 3 studies [17, 19, 24]reported the patient's maximum walking speed of 10 meters. There was no statistical heterogeneity between the studies (P = 0.22, I2= 35%), and a fixed effect model was used for statistical integration. The results showed that the maximum walking speed of 10 meters in the CST group was higher than that of the conventional rehabilitation group [MD = 10.18, 95% CI (6.37-14.00),P < 0.001] (Figure 9).

Figure 7 Effects of core stability exercise on walking function

Figure 8 Effects of core stability exercise on step length
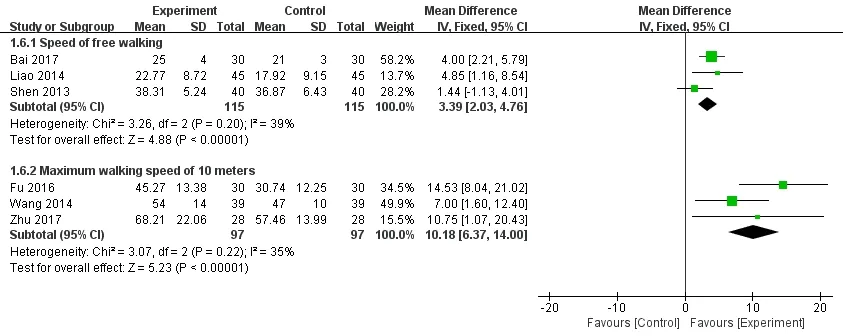
Figure 9 Effects of core stability exercise on walking speed
Discussion
Influence on the trunk control
The functional activities of the human body require the interaction between the limb and the trunk. And the control of the trunk will directly affect the human motor function, balance function and walking ability [25]. In addition, studies have shown that the ability to control the trunk is also highly correlated with the ability of daily living activities of patients [26]. In this study,meta-analysis was used to quantitatively integrate the evidence of trunk control ability through core stability training. The results showed that the core stability training could significantly improve the trunk control ability of stroke patients with hemiplegia. The reason may be that the core stability training focused on the strength and control training of the pelvis muscle,transversus muscle, multifidus muscle, iliopsoas muscle,and the gluteal muscles compared with traditional exercise therapy, and more emphasis is placed on the exercise of the core muscles of the trunk. The increase in muscle strength of the core muscles of the trunk may improve the control of the trunk [26, 27].
Influence on the balance ability
The muscles of the hemiplegia side of the stroke patients have such problems, such as muscle weakness,muscle abnormalities, and motor control disorders,which makes the balance function of the patient severely affected [29]. This meta-analysis showed that core stability training could improve the balance of stroke patients with hemiplegia, which was consistent with the study of Cabanas [31]. The reason for this may be that the core stability training focuses on the strength and control of the trunk and other deep and core muscles. And the strengthening of the trunk muscles and the increased control and coordination ability of the core muscles may improve the patient's balance function [29, 30].
Influence on the ability of daily living activities
Studies have shown that about 70%-80% of stroke patients suffer from decreased of strength, sensory and coordination functions, which leads to balance disorders and physical activity disorders, so the ability of daily living activities of patients and their quality of life would be seriously affected [32]. In this study,meta-analysis was used to quantitatively integrate the evidence of activities of daily living activities. The results showed that core stability training could significantly improve the ability of daily living activities of stroke patients with hemiplegia. This is consistent with the research results of Sun et al. [33],which may be due to core stability training that improves the upper and lower extremity motor function and balance ability of the patient and makes it possible to increase daily activity intensity and activity.
Influence on walking function
Recovery of walking function is the focus and ultimate goal of stroke rehabilitation training. The walking function is the premise and guarantee of daily activities and is closely related to the quality of life. This meta-analysis showed that core stability training could significantly improve the walking function of stroke patients with hemiplegia. This is consistent with the findings of Haruyama et al. [34]. The reason may be that the core stability training focuses on the muscle strength control training of the trunk and pelvic muscle groups, and adjusts the coordination of the lumbar and pelvic girdle muscle groups to make the affected side and the healthy side muscles strength tend to balance,improve the control of the contralateral and ipsilateral muscle groups, improve the coordination of the patient's limb movements, and thus improve walking function.
Influence on step length and walking speed
Stroke patients with hemiplegia often have problems with prolonged support of the lower extremities,balance and coordination dysfunction, lower limb weights and weakened control ability, which can affect the patient's gait, reduce the pace, and affect the patient's self-image perception. It also increases the risk of falling patients [35]. The results of this meta-analysis showed that core stability training could improve the pace of stroke patients with hemiplegia, but had little effect on their stride length. The reason may be that the core stability training focuses on the strength and control of deep muscle groups such as the pelvis and torso, enhances the controllability and contractility of the ventral muscles, provides the fulcrum for the swing of the lower extremity of the affected side, and suspends the weight of the legs, thereby increasing the patient's walking pace [36, 37]. However, the study on patient's pace was only included in two articles, and the sample size was small and there might exist a bias.
Limitations
Some limitations in the present meta-analysis should be noted: (1) All the randomized controlled trials included in this study were based on conventional rehabilitation therapy combined with core stability training in the intervention group and conventional rehabilitation training only in the control group, but the contents of routine rehabilitation treatment in each study were different, which might result potential clinical heterogeneity; (2) All the quality ratings included in this meta-analysis were B-level, and lacked of well-designed, high-quality grade-related studies; (3)Since the number of indicators in this study was small,they were all less than 10, so we did not draw the funnel diagram, so there was a possibility of publication bias;(4) The included studies were all domestic studies,which weakened the extrapolation of the study.
Conclusion
Core stability training on the basis of conventional rehabilitation therapy can improve the trunk control ability, balance ability, walking function and activity of daily living in patients with stroke hemiplegia, and increase the patient's walking speed, but there is no significant difference in stride length. Since the quality of randomized controlled trials included in this study is not of very high and the sample size is small, it is recommended that more well-designed, large-sample,high-quality relevant studies should be conducted to further determine the effectiveness of core stability training interventions and make more reliable conclusions to guide clinical practice.
杂志排行

TMR Non-Drug Therapy的其它文章
- Acupuncture as a potential approach to improving the health of women with obesity
- Randomized control study in the influence of different training methods of Tai Chi on Chinese medicine constitution of international students with depression or depression tendency
- Surgical use of fire needle for connective tissue external hemorrhoids:a case report
- Fire needle combined with filiform needle therapy for hemifacial spasm: a case report