Impact of gender on outcomes after transcatheter aortic valve implantation
2018-08-17NooraldaemYousifSlaymanObeidRonaldBinderAndreaDenegriMohammadyShahinChristianTemplinThomasscher
Nooraldaem Yousif, Slayman Obeid, Ronald Binder,Andrea Denegri,Mohammady Shahin,Christian Templin, Thomas F Lüscher
Impact of gender on outcomes after transcatheter aortic valve implantation
Nooraldaem Yousif*, Slayman Obeid*, Ronald Binder,Andrea Denegri,Mohammady Shahin,Christian Templin, Thomas F Lüscher
Department of Cardiology, University Heart Center, University Hospital Zurich, Switzerland and Royal Brompton & Harefield Hospital, Imperial College, London, United Kingdom
The influence of gender on clinical outcomes following transcatheter aortic valve implantation (TAVI) was considerably discrepant in previous studies.We aimed to investigate the impact of gender in our registry.The study is a retrospective observational analysis of a prospectively designed cohort (546 consecutive patients treated at the University Hospital Zurich who were enrolled in Swiss TAVI Cohort from May 2008 to April 2014). The Study took place in University Heart Centre at University Hospital Zurich, Switzerland.Both genders were equally represented with 51.5 % (= 281) of the populations being females, who were significantly older and had a more pronounced history of hypertension (< 0.001). Males on the other hand showed a higher incidence of diabetes (= 0.004), coronary artery disease (< 0.001), chronic obstructive pulmonary disease (< 0.001) and renal failure requiring renal replacement therapy (= 0.018). Patients were followed up for a median of 391 days with a 100% complete follow-up at one year. The primary outcome (all-cause mortality) occurred in 6.8% (= 37) and 15% (= 82) of patients at 30 days and one year, respectively. The 30-day all-cause mortality outcome did not significantly differ between females (7.5%) and males (6.0%) (= 0.619), but one year all-cause mortality occurred significantly more in males than in females (18.7%. 11.7%,< 0.037).After TAVI implantation for severe aortic stenosis, males have a less favorable long-term (one year) mortality outcome than females.
J Geriatr Cardiol 2018; 15: 394400. doi:10.11909/j.issn.1671-5411.2018.06.013
Aortic stenosis; Aortic valve; Gender; Transcatheter aortic valve implantation
1 Introduction
Aortic stenosis is the most common valvular heart disease in the elderly, and a considerable increase in its incidence is foreseen for the coming decades because of the progressive aging of western populations.[1,2]Importantly, symptomatic aortic stenosis is not only associated with breathlessness, angina and syncope, but also with a high rate of death, if left untreated.[3–5]
Several studies reported sex-related incidence of complications and death after TAVI, but their results are inconsistent.[6–10]In 2015, Conrotto and his colleges published a meta- analysis, in which they analyzed six studies with 6645 patients from a MEDLINE search, Cochrane Library and Scopus databases and found that female gender was significantly related to a lower risk of death with an odds ratio of 0.82 at one year, but no Mortality difference at 30 day post TAVI.[9]A previous meta-analysis from China that involved 27 articles with a total of 9118 patients, concluded that male gender was associated with significantly higher risk for death at both 30 days with a relative risk of 1.37 and at one year with a relative risk of 1.30.[8]This was in contrast to the retrospective analysis published by the UK National Institute for Cardiovascular Outcomes Research that investigated 1627 patients from the UK TAVI registry and found no gender-related mortality difference at 30 day and one year follow up.[10]
In view of considerable discrepancies with regard to gender-related differences in complications and outcomes after TAVI and the fact that the contributing factors remain incompletely understood; we designed this retrospective observational study to explore the prognostic influence of gender in patients who underwent TAVI in our registry.
2 Methods
2.1 Setting
The study is a retrospective observational analysis of a prospectively designed cohort (546 consecutive patients treated at the University Hospital Zurich who were enrolled in Swiss TAVI Cohort from May 2008 to April 2014). The Study took place in University Heart Centre at University Hospital Zurich, Switzerland.
2.2 Study population
All patients have been selected for TAVI after multidisciplinary team review by a dedicated heart team of invasive and non-invasive cardiologists, cardiac surgeons and anesthesiologists at our institution. Voluntary informed written consent was obtained from all patients to be included in the Swiss TAVI registry.
2.3 TAVI procedure
TAVI was performed via either the transfemoral, transapical or transaortic routes with implantation of diverse valves such as the Medtronic’s CoreValve®, Edwards®, Symetis®or Ventor Embracer®. A transfemoral first policy was applied, if non-applicable due to any reason (i.e., femoral artery size, aortic disease among others) then alternate access routes were considered.
All procedures conducted through transapical and transaortic routes were performed under general anesthesia, whereas devices implanted through the transfemoral route were most commonly performed with sedation with local anesthesia and only rarely under general anesthesia.
Transthoracic echocardiography was used to measure aortic valve pressure gradient and aortic valve area before TAVI. Aortic regurgitation grade and left ventricular ejection fraction (LVEF) before and after TAVI was also determined in each patient using echocardiography. Mean aortic gradient was further confirmed during cardiac catheterization with invasive measurement before and after the procedure. The Valve Academic Research Consortium Criteria were used to assess and evaluate procedural success, safety end points and clinical outcomes.[11]
2.4 Eligibility
Inclusion criteria were elderly patients with symptomatic severe aortic stenosis, deemed at high risk for conventional surgical aortic valve replacement. Exclusion criteria were patient’s refusal of informed consent to participate in the registry or lack of capacity to consent and/or high probability of non-adherence to follow-up requirements.
2.5 Outcomes
The primary outcome comprised all-cause death at 30 days and one year. The secondary outcomes were complications at 30 days after TAVI including stroke, major bleeding, major vascular access related complications, deranged creatinine level, and valve related dysfunction; other studied outcomes were the occurrence of any of the following during the one year follow-up: valve related dysfunction, NYHA III or IV, hospitalization for valve related symptoms and the requirement for a pacemaker implantation. All clinical end points were in concordance with the widely accepted VARC-2 definitions.
2.6 Statistical analysis
Descriptive statistics were performed using summary statistics (mean, standard deviation, and range) for quantitative variables and frequencies for binary and nominal variables. Demographic and clinical variables were tested at baseline against the primary variable of interest (gender) using parametrictest, non-parametric chi-square test, or non-parametric Wilcoxon rank sum test as appropriate. Box-and- whisker plots were used to display such relationships. We evaluated the unadjusted effect for gender on survival following TAVI procedure, and then moved on to include the potential clinical and demographic covariates utilizing the log-likelihood and behaviour of the residuals to assess the model fit and confirm the independent impact of gender on survival posy-TAVI. Kaplan-Meier plots were used to display the cumulative survival functions of males and females in terms of the prognostic outcomes specified.
为了解决低段学生书籍匮乏之苦,学校发动全校老师为学生捐书,把家中优秀的注音读物贡献出来,存放在学校连廊的小书吧中,供学生课间及午间进行阅读。这一举措同时也带动了许多家长主动来捐书。在读书节,中高年级的学生也把拼音读物搬上了跳蚤市场,为低段的学生创造了一个收集课外书的机会。每个班级还把在跳蚤市场义卖所得,用来购买课外书,充实了班级的图书角。
We used the statistical software package SPSS-20 for windows to perform the statistical analysis and for producing graphs and plots. The statistical significance threshold was set at 5%.
3 Results
3.1 Baseline and procedural characteristics
Male and female participants of the study were comparable in numbers (49.5 %. 51.5%). With regard to age, females tended to be significantly older than males (mean: 83.3 ± 6.95. 80.7 ± 6.91 years,< 0.001), while males outnumbered females in terms of the following co-morbidities: diabetes mellitus (59.8%. 40.2%,= 0.004 ), cardiovascular disease (CAD; 58.7%. 41.3%,< 0.001), chronic obstructive airway disease (COPD; 65.0%. 35.0%,= 0.0003), renal impairment (mean: 130.48 ± 72. 100.95 ± 71 µmol/L,< 0.001) and the need for regular dialysis (76.2%. 23.8%,= 0.018). On the other hand, there were far less hypertensive males than females [46.4%. 53.6%, respectively (< 0.001)].
In terms of pre-procedural left ventricular ejection fraction (LVEF), the mean value averaged 55% (SD = 13.3%, range: 19%-88%), with males tending to have significantly lower LVEF than females (51.5% ± 13.9%. 58.4% ± 11.7%,< 0.001). These differences in baseline characteristics were reflected in a significantly higher logistic EuroSCORE of males 22.7% ± 14%) compared to females (21.1% ± 12.7%;= 0.031).
The common femoral artery was the most common access site in 85.2% of the cases. In terms of valve types, both the CoreValve®(50.5%) and Edwards®Valve (48.4%), were most commonlly used, while only a few patients received the Symetis®or Ventor®device (1.2% of the cases). With respect to gender differences, more CoreValve®and Symetis®were used in females, whereas more Edwards Sapien®were used in males, a difference that reached statistically significance (= 0.003).
The complete list of baseline characteristics of the patients is depicted inTable 1.
3.2 Primary outcome
3.2.1 30-day mortality
In terms of the 30-day all-cause mortality, death occurred in 6.6% of patients (= 37), which was not statistically different between females (7.5%;= 21) and males (6.0%;= 16) (2= 0.2467, df = 1,= 0.6194)
3.2.2 1-year mortality after TAVI
Even after adjusting for the effect of all other covariates, the effect of gender on the risk of post-TAVI mortality was statistically significant (adjusted HR = 1.71,= 0.015). So, in patients with comparable covariates, a male patient, will have an increased risk of death after a TAVI than a female patient by 71.0% (95% CI: 11.0%-163.6%).
3.3 Secondary outcomes
Males tended to have higher creatinine plasma levels post-TAVI compared to females (148 ± 101. 109.7 ± 98 mg/dL,< 0.001; Figure 3).
Regarding the other possible gender-related differences in outcomes 30 days after TAVI, all were statistically non- significant during short term follow-up (i.e., major bleeding, vascular complications, stroke, valve dysfunction and follow-up NT brain natriuretic plasma level during hospitalization post TAVI) as well as the differences in long-term outcomes during the entire period of follow-up post TAVI (i.e., all causes of valve dysfunction, NYHA III or IV, hospitalization for valve related symptoms or pacemaker implantation) were also not statistically significant. The complete list of the primary and secondary outcomes is depicted in Table 2.
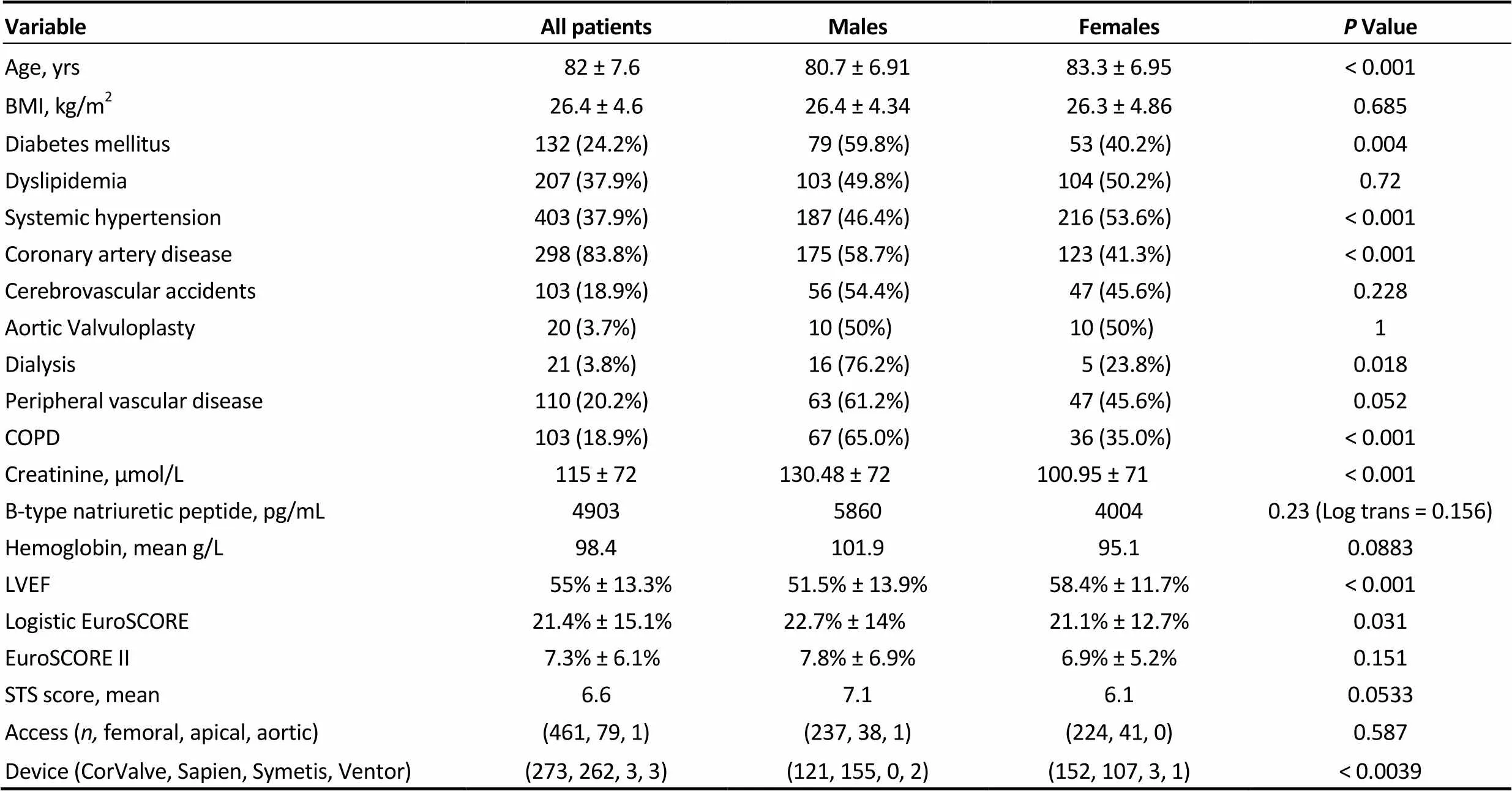
Table 1. Baseline characteristics and procedural demographics.
Data are presented as mean ± SD or(%) unless other indicated. BMI: body mass index; COPD: chronic obstructive airway disease; LVEF: left ventricular ejection fraction.
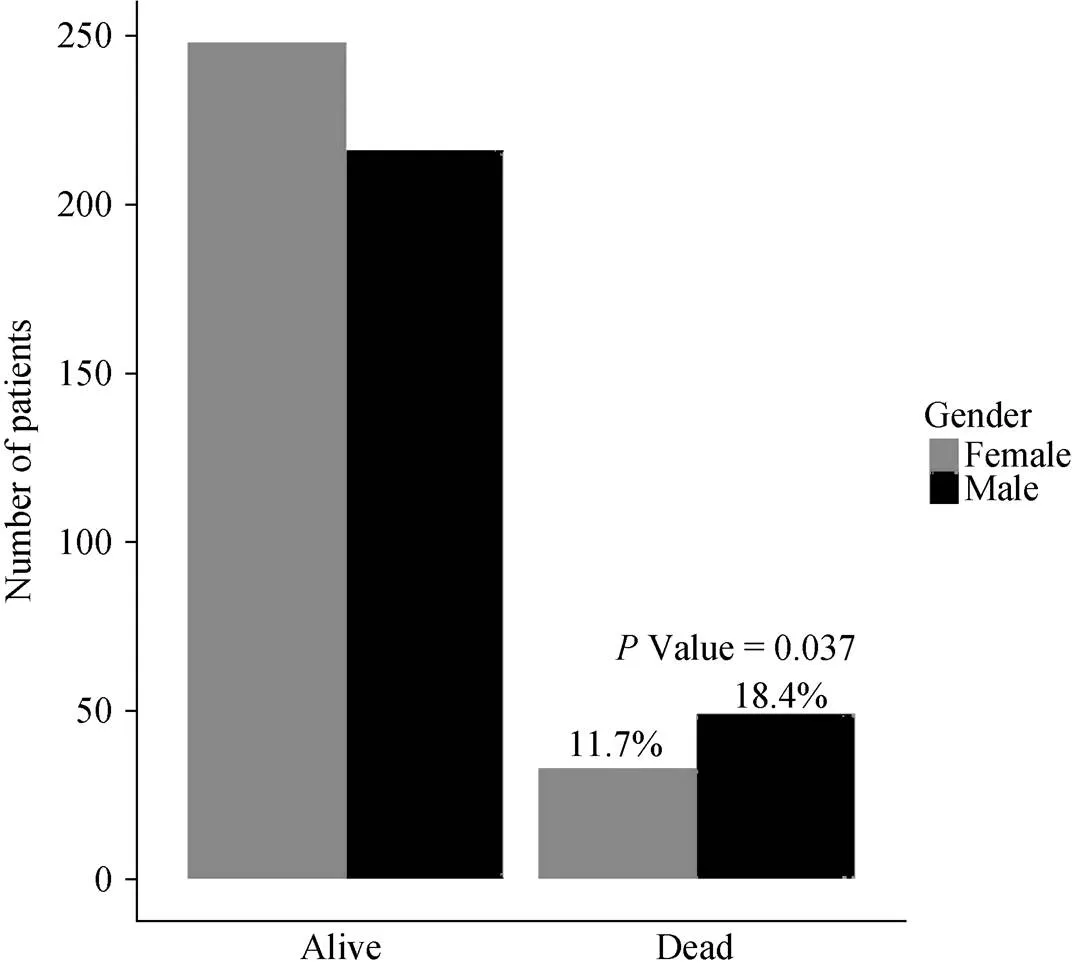
Figure 1. One year mortality outcome after transcatheter aortic valve implantation.
4 Discussion
The current study shows a significant survival benefit of females undergoing TAVI when compared to male patients with severe and symptomatic aortic stenosis. This benefit, although not obvious at 30 days, was significant at one year follow-up with an odds ratio of 1.70. Our finding therefore support the findings of the Italian meta-analysis of 6 studies incorporating 6645 patients, where they found that female gender was significantly related to a lower risk of death at one year, but not at 30 day post TAVI.[9]
There is currently no clear cut explanation for the fact that women do better than men after TAVI. However, the interplay of several risk factors and co-morbidities as well as different gender-related cardiac pathophysiological responses to pressure afterload might be involved. Indeed, gender has a major impact on the development of left ventricular hypertrophy due to a different response to pressure overload.[12–15]Indeed, women with aortic stenosis tend to develop a more concentric form of left ventricular hypertrophy with smaller ventricular diameters, greater relative wall thicknesses, and a better systolic function, while men with comparable degree of pressure overload exhibit a more eccentric form of left ventricular hypertrophy with more ventricular dilation, fibrosis, a decreased ejection fraction and development of heart failure.[12,16]In line with this interpretation, males of our cohort were found to have statistically significant lower left ventricular hypertrophy at the time of TAVI compared to females (51.5%. 58.4%). This finding could as well be explained by the fact that more aggressive cardiac remodeling is normally seen in men secondary to longstanding pressure overload; eventually leading to a more dilated left ventricle and less favorable geometry to preserve systolic function.[17,18]

Figure 2. Cumulative survival after TAVI. TAVI: transcatheter aortic valve implantation.
Figure 3. Highest creatinine after transcatheter aortic valve implantation.

Table 2. Clinical outcomes after TAVI.
Data are presented as mean ± SD or(%) unless other indicated. TAVI: transcatheter aortic valve implantation.
At the cellular level, there is a large body of evidence linking such an abnormal myocardial hypertrophy and fibrosis in men with aortic stenosis to increased expression of transforming growth factor beta-1 protein (TGF-β1) and phosphorylation of SMAD2. Furthermore, periostin, a down-stream target of TGF-β1 signaling and a key regulator of cardiac fibrosis is more expressed in men.[19]In human failing hearts, up-regulation of periostin expression is associated with cardiac fibrosis.[20]Higher periostin levels were finally found in blood obtained from male compared with female patients with heart failure. This link between pattern of remodeling and survival raises the question of optimizing the management of aortic stenosis in a sex-specific manner.[21–23]
From a metabolic point of view, recent findings linking aortic stenosis to common atherosclerotic pathways could help to further explain the lower incidence of coronary artery disease in females in conjunction to the protective role of estrogen with its anti-atheromatous effects, aiding to better area of viable myocardium reflected by a higher left ventricular ejection fraction and swift recovery post TAVI in females.[24,25]The latter finding of higher left ventricular ejection fraction and lower percentage of coronary artery disease in women undergoing TAVI compared to men was documented in our study as well as in many other studies like the UK TAVI registry and other Meta-analyses.[8–10]
It is also worth noting that males in our cohort were evidently a sicker population than females, as they had an overall higher surgical risk reflected by a slightly higher Logistic EuroSCORE, along with a higher incidence of comorbidities and cardiovascular risk factors including but not limited to diabetes mellitus, coronary artery disease and renal impairement, in some even requiring hemodialysis. Of note, males tend to have significantly higher creatinine post-TAVI than females. However, this was also true for baseline pre-procedural creatinine levels. Furthermore, in logistic regression analysis we found that an increase in eGFR by one unit makes a patient, on average, less likely to die within 30-days post TAVI (OR =-0.003, 95% CI:-0.005 to-0.001). This impact of renal function has long been addressed in patients undergoing surgical valve replacement, where chronic kidney disease and acute kidney injury after the procedure were both found to be independent predictors of mortality.[26–28]However, these variables created a bit of controversy regarding their predictive ability in TAVI, While some studies have found a staged classification of chronic kidney disease before valve implantation to be a predictor of both mortality and the development of acute kidney injury, others did not share the same view. Furthermore, the association of acute kidney injury with worse outcome is also still debatable due to similar inconsistencies in studies’ outcomes and that the definition of acute kidney injury post TAVI has been much disputed.[29,30]Overall,the risk profile of the current cohort of TAVI patients is consistent with most of other registries’ baseline characteristics.[8–10]
Interestingly, the study showed that there were no statistically significant gender differences in the rate of vascular and bleeding complications during the TAVI procedure, although many of the previous studies reported more access- related vascular and bleeding complications in women.[31–33]This may reflect insufficient statistical power, because of the small event numbers off these complications in our study population (4.2% and 2.4%, respectively), but also may reflect the experience of the center and the successful implementation of vascular closure devices to achieve hemostasis post TAVI.
4.1 Limitations
The current study is limited by being a retrospective analysis, albeit from a prospectively acquired data set. However, the principle comparison is being made between genders (which are fixed) and thus there is less risk of erroneous conclusions from allocation bias. Also, despite that a great care was taken in selecting patients, the possibility of selection bias reflected by Sex-differences in baseline characteristics and comorbidities cannot be completely ruled out, as Men at baseline outnumbered females in term of diabetes mellitus, CAD, COPD, dialysis, lower LVEF, higher logistic EuroSCORE while females were older with higher percentage of Arterial HTN diagnosis, but it is always infeasible to balance and standardize the pre-procedural characteristics giving the fact that TAVI is reserved for elderly patients with severe AS, deemed high risk for conventional surgical intervention and this category of elderly patients likely to present with numerous comorbidities.
4.2 Conclusion
Female gender is associated with a better survival at one-year follow up after TAVI. This finding reflects that gender plays a significant prognostic role and should be integrated in a potential risk stratification model of patients considered for the procedure. On the other hand, risk factors could be rendered obsolete, as they do not fit the risk profile of a gender based risk assessment. Furthermore, our findings could open the door for a gender tailored medical therapy where males with severe aortic stenosis could benefit from a more intense pre-procedural treatment reflected as an improvement in survival post valve implantation.
Acknowledgments
Yousif N and Obeid S have no conflicts of interest to disclose. Lüscher TF has received research and educartional grants from Medtronic, Inc., Tollachenaz and Switzerland, Edwards Inc., to the institution. Obeid S and Denegri A were supported by grants of the Zurich Heart House— Foundation for Cardiovascular Research thanks to donations of H.H. Sheikh Khalifa Bin Hamad AL—Thani and Medtorinc, Inc.
1 Rodés-Cabaua J, Ureñaa M, Nombela-Francoa L. Indications for transcatheter aortic valve replacement based on the PARTNER trial.2012; 65: 208–214.
2 Webb JG, Pasupati S, Humphries K,. Percutaneous transarterial aortic valve replacement in selected high-risk patients with aortic stenosis.2007; 116: 755–763.
3 Grube E, Buellesfeld L, Mueller R,. Progress and current status of percutaneous aortic valve replacement: results of three device generations of the CoreValve revalving system.2008; 1: 167–175.
4 Cribier A, Litzler PY, Eltchaninoff H,. Technique of transcatheter aortic valve implantation with the Edwards-Sapien heart valve using the transfemoral approach.2009; 34: 347–356.
5 Iung B, Baron G, Butchart EG,. The Euro heart survey on valvular heart disease.2003; 24:1231–1243.
6 Stangl V, Baldenhofer G, Knebel F,. Impact of gender on three-month outcome and left ventricular remodeling after transfemoral transcatheter aortic valve implantation.2012; 110: 884–890.
7 Zahn R, Gerckens U, Linke A,. Predictors of one-year mortality after transcatheter aortic valve implantation for severe symptomatic aortic stenosis.2013; 112: 272–279.
8 Zhao ZG, Liao YB. Sex-related differences in outcomes after transcatheter aortic valve implantation.2013; 6: 543–551.
9 Conrotto F, D'Ascenzo F, Presbitero P, Humphries KH. Effect of gender after transcatheter aortic valve implantation.2014; 103: 613–620.
10 Al-Lamee R, Broyd C, Parker J,. Influence of gender on clinical outcomes following transcatheter aortic valve implantation from the UK transcatheter aortic valve implantation registry and the National Institute for Cardiovascular Outcomes Research.2014; 113: 522–528.
11 A. Pieter Kappetein, Stuart J. Head, Martin B. Leon. The Valve Academic Research Consortium-2 consensus document.2012; 60: 1438–1454.
12 Petrov G1, Dworatzek E2, Schulze TM,. Maladaptive remodeling is associated with impaired survival in women but not in men after aortic valve replacement.2014; 7: 1073–1080.
13 Stansfield WE, Andersen NM, Tang RH, Selzman CH. Periostin is a novel factor in cardiac remodeling after experimental and clinical unloading of the failing heart.2009; 88: 1916–1921.
14 Villar AV, Llano M, Cobo M. Gender differences of echocardiographic and gene expression patterns in human pressure overload left ventricular hypertrophy.2009; 46: 526–535.
15 Fliegner D, Schubert C, Penkalla A. Female sex and estrogen receptor-beta attenuate cardiac remodeling and apoptosis in pressure overload.2010; 298: R1597–R1606.
16 Douglas PS, Katz SE, Weinberg EO. Hypertrophic remodeling: gender differences in the early response to left ventricular pressure overload.1998; 32: 1118–1125.
17 Piro M, Bona RD, Abbate A,. Sex-related differences in myocardial remodeling.2010; 55: 1057–1065
18 Gardner JD, Brower GL, Janicki JS. Gender differences in cardiac remodeling secondary to chronic volume overload.2002; 8: 101–107.
19 Douglas PS, Otto CM, Mickel MC,. Gender differences in left ventricle geometry and function in patients undergoing balloon dilatation of the aortic valve for isolated aortic stenosis.1995; 73: 548–554.
20 Kupari M, Turto H, Lommi J. Left ventricular hypertrophy in aortic valve stenosis: preventive or promotive of systolic dysfunction and heart failure?2005; 26: 1790–1796.
21 Kararigas G, Bito V, Tinel H. Transcriptome characterization of estrogen-treated human myocardium identifies myosin regulatory light chain interacting protein as a sex-specific element influencing contractile function.2012; 59: 410–417.
22 Edwards F, Peterson E, Coombs L,. Prediction of operative mortality after valve replacement surgery.2001; 37: 885–892.
23 Petrov G, Regitz-Zagrosek V, Lehmkuhl E. Regression of myocardial hypertrophy after aortic valve replacement: faster in women?2010; 122: S23–S28
24 Adams MR, Williams JK, Kaplan JR. Effects of androgens on coronary artery atherosclerosis and atherosclerosis-related impairment of vascular responsiveness.1995; 15: 562–570.
25 Muller M, van den Beld AW, Bots ML,. Endogenous sex hormones and progression of carotid atherosclerosis in elderly men.2004; 109: 2074–2079.
26 Neragi-Miandoab S, Michler RE. A review of most relevant complications of transcatheter aortic valve implantation.2013; 2013: 956252.
27 Tchetche D1, Van der Boon RM, Dumonteil N,. Adverse impact of bleeding and transfusion on the outcome post- transcatheter aortic valve implantation.2012; 164: 402–409.
28 D'Ascenzo F, Gonella A, Moretti C,. Gender differences in patients undergoing TAVI.2013; 9: 367–372.
29 Hobson CE, Yavas S, Segal MS,. Acute kidney injury is associated with increased long-term mortality after cardiothoracic surgery.2009; 119: 2444–2453.
30 Aregger F, Wenaweser P, Hellige G,. Risk of acute kidney injury in patients with severe aortic valve stenosis undergoing transcatheter valve replacement.2009; 24: 2175–2179.
31 Wessely M, Rau S, Lange P,. Chronic kidney disease is not associated with a higher risk for mortality or acute kidney injury in transcatheter aortic valve implantation.2012; 27: 3502–3508.
32 Wessely M, Rau S, Lange P,. Frequency, determinants, and prognostic effects of acute kidney injury and red blood cell transfusion in patients undergoing transcatheter aortic valve implantation.2011; 77: 881–889.
33 Cribier A, Eltchaninoff H, Tron C,. Treatment of calcific aortic stenosis with the percutaneous heart valve, the French experience.2006; 47: 1214–1223.
*The first two authors contributed equally to this manuscript
Thomas F Lüscher, MD, Royal Brompton & Harefield Hospital, Imperial College, London, SW3 6NP, United Kingdom. E-mail: cardio@tomluescher.ch
December 24, 2017
February 11, 2018
March 20, 2018
June 28, 2018
猜你喜欢
杂志排行

Journal of Geriatric Cardiology的其它文章
- “Malignant” right coronary artery presenting as an ST-segment elevation myocardial infarction—a case report
- Influenza vaccination in acute coronary syndromes patients in Thailand: the cost-effectiveness analysis of the prevention for cardiovascular events and pneumonia
- The trend of change in catheter ablation versus antiarrhythmic drugs for the management of atrial fibrillation over time: a meta-analysis and meta-regression
- Early mortality and safety after transcatheter aortic valve replacement using the SAPIEN 3 in nonagenarians
- Depression and chronic heart failure in the elderly: an intriguing relationship
- CIED implantation in elderly patients: a single-center experience