Exercise-induced muscle fatigue in the unaffected knee joint and its influence on postural control and lower limb kinematics in stroke patients
2017-06-05SunWookParkSungMinSonNaKyungLee
Sun Wook Park, Sung Min Son, Na Kyung Lee
1 Department of Physical Therapy, Faculty of Health Science, Eulji University, Seongnam-si, Gyeonggi-do, Republic of Korea
2 Department of Physical Therapy, College of Health Science, Cheongju University, Cheongju-si, Chungbuk, Republic of Korea
3 Department of Physical Therapy, College of Rehabilitation Science, Daegu University, Gyeongsan-si, Kyeongbuk, Republic of Korea
Exercise-induced muscle fatigue in the unaffected knee joint and its influence on postural control and lower limb kinematics in stroke patients
Sun Wook Park1, Sung Min Son2, Na Kyung Lee3,*
1 Department of Physical Therapy, Faculty of Health Science, Eulji University, Seongnam-si, Gyeonggi-do, Republic of Korea
2 Department of Physical Therapy, College of Health Science, Cheongju University, Cheongju-si, Chungbuk, Republic of Korea
3 Department of Physical Therapy, College of Rehabilitation Science, Daegu University, Gyeongsan-si, Kyeongbuk, Republic of Korea
How to cite this article:Park SW, Son SM, Lee NK (2017) Exercise-induced muscle fatigue in the unaffected knee joint and its influence on postural control and lower limb kinematics in stroke patients. Neural Regen Res 12(5):765-769.
Open access statement:This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This study aimed to investigate the effects of exercise-induced muscle fatigue in the unaffected knee joint on postural control and kinematic changes in stroke patients. Forty participants (20 stroke patients, 20 age-matched healthy participants) were recruited. To induce fatigue, maximum voluntary isometric contractions were performed in the unaffected knee joint in a Leg Extension Rehab exercise machine using the pneumatic resistance. We measured static and dynamic balance and lower-limb kinematics during gait. Changes in postural control parameters anteroposterior sway speed and total center of pressure distance differed significantly between the stroke and control groups. In addition, changes in gait kinematic parameters knee and ankle angles of initial contact differed significantly between stroke (paretic and non-paretic) and control groups. Muscle fatigue in the unaffected knee and ankle impaired postural control and debilitates kinematic movement of ipsilateral and contralateral lower limbs, and may place the fatigued stroke patients at greater risk for falls.
nerve regeneration; knee; muscle fatigue; stroke; postural control; gait kinemetics; neural regeneration
Introduction
Individuals after stroke are often left with disabling motor and sensory impairments, leading to reduced functional ability and quality of life (Paolucci et al., 2003; Hackett and Anderson, 2005). Many stroke patients have limited postural control and walking capability associated with hemiparesis (Ikai et al., 2003; Flansbjer et al., 2006; Balasubramanian et al., 2007). For example, abnormal center of mass while standing leads to dysfunctional balance strategies or asymmetries in kinematics related to decreased power in the affected leg.
Neuromuscular fatigue, defined as exercise-induced reduction in power output and work capacity of the skeletal muscle, can be quantified as the reduction in strength over time or as the duration of sub-maximal sustained tasks (Bigland-Ritchie and Woods, 1984; Bellew and Fenter, 2006; Kanekar et al., 2008; Reimer and Wikstrom, 2010). Muscle fatigue related to the knee joint induces a reduction and delay in the activation of the quadriceps and hamstring muscles in response to rapid destabilizing perturbations potentially reducing the stability around the knee (Parijat and Lockhart, 2008) and altering the knee moment in the sagittal plane in healthy participants during walking (Walter et al., 2010; Murdock and Hubley-Kozey, 2012). Several studies have reported a disturbance of postural control and the changes in gait kinesiology after the performance of a fatiguing motor task involving different lower-limb joints such as the ankle, knee, and hip (Lin et al., 2009; Vuillerme et al., 2009; Berger et al., 2010, 2011; Vuillerme and Boisgontier, 2010).
In generally, stroke patients commonly show muscle fatigue, possibly due to the relatively high levels of muscular effort that they need to invest in locomotion. Many functional tasks challenging to stroke patients require sub-maximal symmetric torque production in bilateral lower limb joints to optimal postural control and energy efficiency (Hyngstrom et al., 2012). Stroke-related muscle fatigue may impede the functional mobility and contribute to long term disability. Although a few studies have examined fatigability of the affected lower limb during fatigue protocol of the musculature at sub-maximal torque (Hyngstrom et al., 2012; Rybar et al., 2014), no studies have addressed changes in the unaffected lower limb,i.e., how changes in neuromuscular fatigability in the unaffected lower limb of stroke patients impact postural control and walking kinematics.
Therefore, the purpose of this study was to investigate the effects of exercise-induced muscle fatigue in the unaffected knee joint on postural control and gait kinematic changes of lower-limb in stroke patients.
Subjects and Methods
Participants
Forty participants (20 stroke patients, 20 age-matched healthy participants) were recruited. Stroke patients were recruitedfrom physiotherapy clinics. Inclusion criteria were (1) age between 50 and 70 years, (2) a clinical stroke with brain imaging that is compatible with intracerebral hemorrhage or ischemic stroke occurring at least 6 months before the start of the study, (3) one sided hemiparesis of the lower extremity, and (4) ability to ambulate independently without ankle foot orthoses (AFO). Exclusion criteria were (1) severe cognitive, communicative, perceptual, or sensory problems preventing patient from understanding and/or following verbal instructions, (2) other neurologic, psychiatric problems, or impairments causing difficulties to follow the program, and (3) unstable cardiovascular and ventilatory problems. All of them understood the purpose of this study and provide their written informed consent before participating in the study. The study was performed according to theDeclaration of Helsinki, and the ethical issues were approved by the local committee of the Institutional Review Board (approval number: 1040647-201312-HR-077-3), and the study procedure is shown in Figure 1.
Fatigue protocols
To induce fatigue, maximum voluntary contractions were performed in a Leg Extension Rehab exercise machine using the pneumatic resistance (HUR, Helsinki, Finland). Participants were instructed to sit comfortably in the chair and maintain the knee at 90° of flexion with a free distal extremity. They were asked to extend their non-paretic leg and then slowly flex the knee joint to the starting position. The involved leg of each patient was matched with the corresponding leg of a healthy control according to their dominant side (Negahban et al., 2013). The leg used to kick a ball was defined as dominant (Reimer and Wikstrom, 2010). The fatigue protocol was stopped and it was assumed that the leg muscles were fatigued when the subject expressed inability to continue the task, or when the subject no longer performed at the desired movement frequency, or after 30 minutes (Barbieri et al., 2013; Hatton et al., 2013).
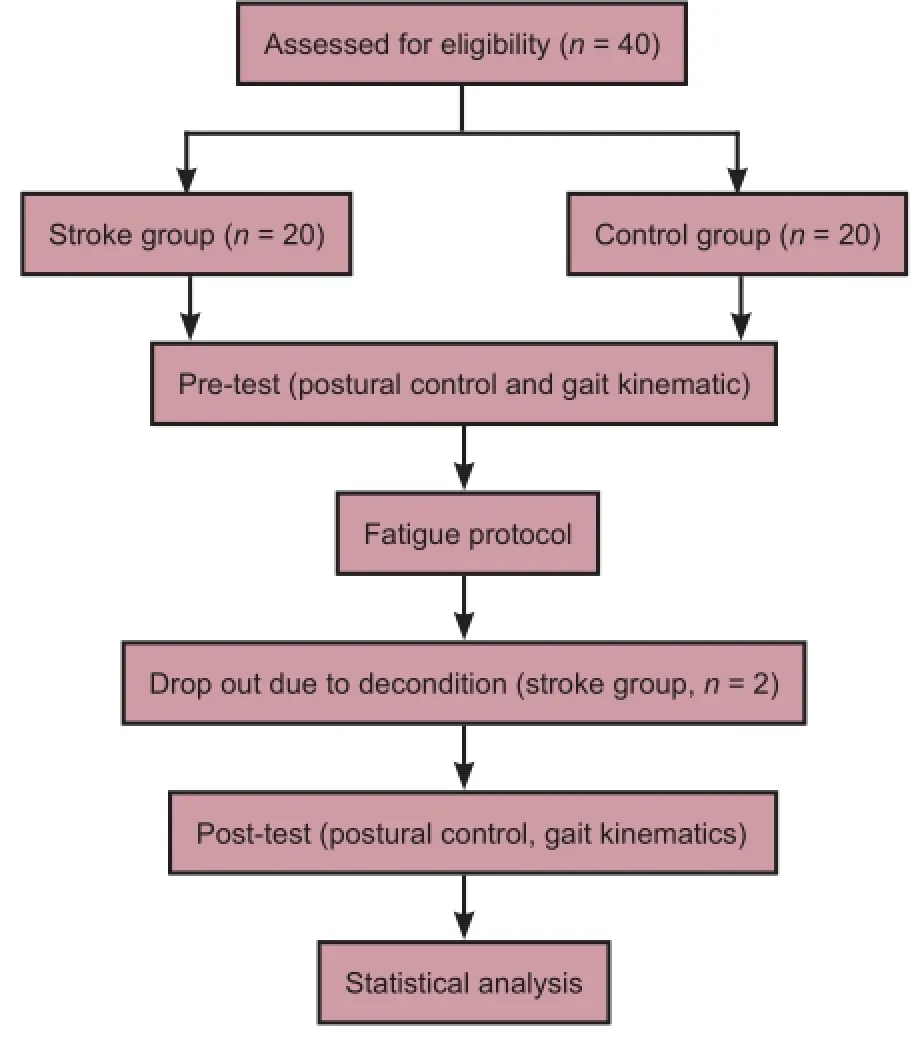
Figure 1 Flowchart of the study.
Measurements
Postural control
Balance was assessed by using the Good Balance System Ver. 3.06 (Metitur Oy, Jyvaskyla, Finland). The platform facilitates the evaluation of stance symmetry and sway of the center of feet pressure for the tested posture (static conditions) (Park and Yim, 2016). It also allows for the dynamic balance test. The evaluation of weight-bearing symmetry was performed for each lower limb separately and differences were expressed in percentages. Measurements were performed in silence for the normal standing position, with the feet placed parallel 20 cm from each other (Lisinski et al., 2012). Static balance testing was performed with the patient standing on the platform with eyes open. Then the participant was asked to maintain maximum focus to remain motionless for 30 seconds.
The participants were instructed to perform the dynamic balance testing by shifting their weight forward toward the target when one of the peripheral targets was presented randomly, and then back to the central target. After demonstrating the tests, the subjects were allowed to practice a preliminary test once before the measurements were taken. Subsequently, the participant swayed to the extent and direction determined by the Good Balance System program. This point moved in accordance with the direction and extent of sways performed by the participant standing on the platform. The maximum, permissible time for task was 120 seconds. The subject was instructed to reach the targets as quickly and accurately as possible, and to avoid unnecessary and uneconomic movements.
Gait kinematics
Sagittal plane movements were simultaneously captured with a standard digital video camera (Sony DCR-HC20E) sampling at 50 Hz. The camera was placed on a tripod perpendicular to the sagittal plane, at a height of 60 cm and a distance of 3.5 m (Dingenen et al., 2015). The reflective markers on the trochanter major, lateral femoral epicondyle, lateral malleolus and metatarsal head V were used to assist manual digitization (Borel et al., 2011). The joint angles of paretic and non-paretic leg of stroke patients and the dominant leg of healthy controls were measured (Figure 2).
Data analysis
Anteroposterior, mediolateral sway speed (mm/s) and total center of pressure (COP) distance were calculated automatically with the Good Balance System Ver. 3.06 (METITUR) (Lisinski et al., 2012).
2D images were captured onto an external hard disk drive that was plugged into a laptop computer. The point of joint ankle was measured on 2D video images using a commercial software package (Dartfish software 6.0, Fribourg, Switzerland) (Dingenen et al., 2015). The knee angle was the angle between the line formed by the greater trochanter and the lateral femoral epicondyle, and a second line connecting the lateral femoralepicondyle and the lateral malleolus. The ankle angle was the angle between the line formed by the lateral femoral epicondyle and the lateral malleolus, and a second line connecting the lateral malleolus and metatarsal head V. The reliability of the measurement of these 2D angles was previously shown to be good to excellent (Dingenen et al., 2014, 2015).
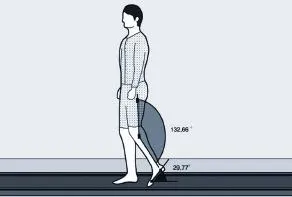
Figure 2 Video screen measurement of knee joint and ankle in toe off with Dartfish software 6.0.
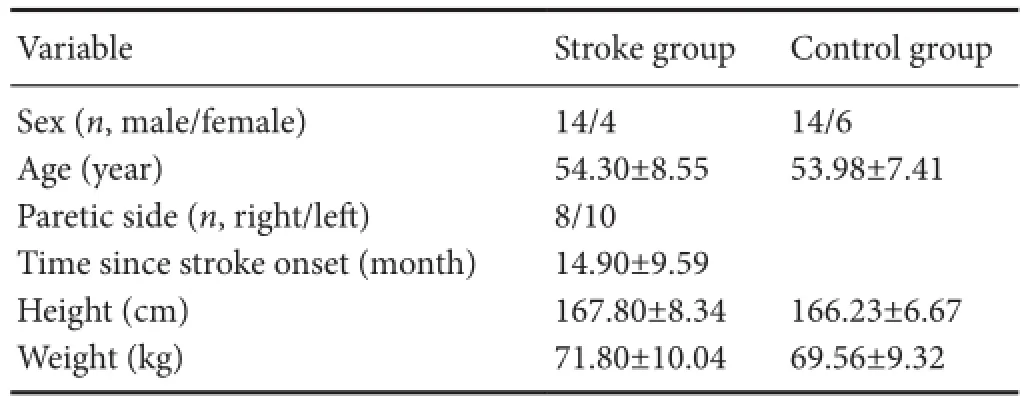
Table 1 Baseline characteristics of participants

Table 2 Postural control testing results of participants in each group

Table 3 Gait kinematic of participants in each group
Statistical analysis
Demographic data, such as sex and age, were analyzed using an independentt-test. Pre- and post-intervention data were examined using the paired t-test within each group of subjects and the analysis of covariance was used between the groups. Analysis of covariance was used to control the variance in the pretest score. The pretest score was the covariate, group was the independent variable, and posttest score was the dependent variable. All statistical analyses were performed using PAWS 18.0 (SPSS, Chicago, IL, USA), andP< 0.05 was used as the criterion for statistical significance.
Results
Baseline variables in the patients in the stroke group did not differ significantly from the control group (P> 0.05; Table 1). Two patients dropped out during this study because of adverse effects, such as pain, de-condition.
Effects of fatigue protocol on postural control
Following the fatigue protocol, compared to pre-test, mediolateral sway speed and total COP distance showed a significant increase in both groups (P< 0.05). However, anterioposterior sway speed showed a significant increase only in the stroke group (P< 0.05). The stroke group showed significantly more increment in anterioposterior sway speed and total distance than the control group (P< 0.05; Table 2).
Effects of fatigue protocol on gait kinematics
After fatigue protocol, compared to pre-test, knee and ankle angles of initial contact showed a significant decrease in three groups (P< 0.05). The stroke group (paretic and non-paretic side) showed significantly more increment in knee and ankle angle during initial contact than control group (P< 0.05, Table 3).
Discussion
Individuals with stroke often rely more on the unaffected side for limb advancement during walking due to the contralateral weakness of a damaged hemisphere, but the effects of muscle fatigue in this group is unknown. In the current study, we investigated the effects of non-paretic knee muscle fatigue on balance and lower limb kinematics in stroke patients. We found that fatigability induced in the knee muscles, with and without stroke, had large functional consequences for people with stroke including balance and major alterations in the lower limb kinematics. Compared with controls following fatiguing, dynamic knee muscle contractions of non-paretic lower limb, stroke participants showed larger relative reduction in anterioposterior sway speed and total center of pressure distance and greater decrements in knee and ankle range of motion during initial contact in the paretic and non-paretic lower limbs.
Muscle fatigue of the lower limb has been indicated to increase postural sway, which is documented through variables calculated from the displacements of the center of pressure. As expected, our results showed that the muscle fatigue protocol of the knee joint affected postural control in both the stroke and control groups. Moreover, individuals with stroke had larger relative increment in anterioposterior and mediolateral sway speed following fatiguing knee flexion and extension. These finding are consistent with those of previous studies that examined the effects of lower limb muscle fatigue induced by isokinetic method on postural control of healthy individuals using a static or dynamic moveable platform (Gribble et al., 2004; Harkins et al., 2005; Dickin and Doan, 2008). Previous studies have observed that postural stability decreased when the difficulty of the task increased, for example, by diminishing the input from one or more sensory systems (Bayouk et al., 2006), or by decreasing the efficiency of neuromuscular system related to muscle fatigue (Caron, 2003; Gribble and Hertel, 2004; Vuillerme et al., 2006; Salavati et al., 2007; Springer and Pincivero, 2009). Hence, from our results, we can deduce that the disturbance of postural control after unilateral knee muscle fatigue is related to a reduction in muscle strength and especially to impairment of the effectiveness of sensorimotor function. The adverse effect on neuromuscular control after muscle fatigue exercise is attributable to the inhibition of afferent and efferent signaling patterns in relation to delayed muscular reaction times (Gribble and Hertel, 2004; Gribble et al., 2004; Salavati et al., 2007). Delayed onset of muscle activity affects the ability to compensate for movement of lower limb and to maintain postural stability (Hassanlouei et al., 2012). As the results, especially, when compared with the control group, an individual with stroke has difficulty in maintaining postural muscle control, due to fatigue of the unaffected lower limb and weakness of the side contralateral to the damaged hemisphere.
Our results indicated that muscle fatigue of the unaffected knee joint decreased the articular angle of the ipsilateral knee and ankle to a greater degree during initial contact in stroke patients, when compared with that in the control group, but did not significantly change during toe off. A possible mechanism for this decrement in the articular angle following muscle fatigue has been suggested in previous studies, which reported that muscle fatigue is associated with reduced power output and work capacity of the skeletal muscle (Enoka and Stuart, 1992; Yeung et al., 1999; St Clair Gibson et al., 2001; St Clair Gibson and Noakes, 2004). Parijat and Lockhart (2008) also reported that fatigue of the quadriceps reduced the articular angle of the knee and the extensor movement during gait. It is also well known that joint and muscle receptors mediate alteration in efferent output of muscles which control the joint movement. It seems that neuromuscular control is disrupted for a short term because muscle fatigue may lead to an increased threshold of muscle discharge. Thus, it is interpreted that muscle fatigue could lead to change in kinematic movement.
Moreover, our results reveal a greater decrease in the articular angle in the stroke group when compared with that in the control group. It is deduced that there was a concurrent lack of modulation of the ipsilateral side of damaged hemisphere such as ipsilateral motor and sensory deficits (e.g., proprioception) in stroke patients. Previous studies have reported the presence of subtle motor and sensory deficits in motor performance on the ipsilateral side as well (Kwon et al., 2007; Son et al., 2013). Additionally, significant changes in the kinematic movement of the contralateral lower limb during gait were also observed. Paillard et al. (2010) indicated that cross-over fatigue disturbs postural control, implying a disturbance in the contralateral monopedal postural control after fatigue of the ipsilateral lower limb muscles. Taken together, these results indicate that fatigue may cause the stroke patients to become vulnerable to falls during destabilizing perturbation and gait.
In summary, our study shows that exercise-induced muscle fatigue of the muscles in the unaffected knee impairs postural control and debilitates kinematic movement of ipsilateral and contralateral lower limbs. Impaired postural control and debilitated kinematic movement due to exercise-induced muscle fatigue may place stroke patients at a greater risk for falls and therefore a therapist should be invited to help reduce muscle fatigue during conditioning and rehabilitations of stroke patients. In addition, patients with muscle fatigue were able to shift less body weight onto their paretic leg. These patients should be encouraged to practice shifting their body weight towards their paretic leg. The challenge of lower limb constraint-induced movement therapy helps patients overcome the learned disuse mechanism by forcing them to use the paretic lower limb. Our study had some limitations. First, although the fatigue protocol was designed to induce fatigue predominantly in the knee muscles, it is important to consider that other joint muscles,e.g., hip muscles are involved and may have been fatigued as well. Second, due to the relatively small number of subjects, the results of this study should be considered as preliminary finidngs. Finally, other kinematic data were not assessed regarding electromyography and gait parameters. Future studies will be required to investigate kinetic and kinematic measurements related to muscle fatigue of the lower limb.
Declaration of patient consent:The authors certify that they have obtained all appropriate participant consent forms. In the form the participants have given their consent for their images and other clinical information to be reported in the journal. The participants understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Author contributions:SWP designed this study. SWP and NKL were responsible for participant recruitment. SMS and NKL collected and analyzed experimental data and contributed to writing the paper. All authors approved the final version of this paper.
Conflicts of interest:None declared.
Plagiarism check:This paper was screened twice using CrossCheck to verify originality before publication.
Peer review:This paper was double-blinded and stringently reviewed by international expert reviewers.
Balasubramanian CK, Bowden MG, Neptune RR, Kautz SA (2007) Relationship between step length asymmetry and walking performance in subjects with chronic hemiparesis. Arch Phys Med Rehabil 88:43-49.
Barbieri FA, dos Santos PC, Vitorio R, van Dieen JH, Gobbi LT (2013) Effect of muscle fatigue and physical activity level in motor control of the gait of young adults. Gait Posture 38:702-707.
Bayouk JF, Boucher JP, Leroux A (2006) Balance training following stroke: effects of task-oriented exercises with and without altered sensory input. Int J Rehabil Res 29:51-59.
Bellew JW, Fenter PC (2006) Control of balance differs after knee or ankle fatigue in older women. Arch Phys Med Rehabil 87:1486-1489.
Berger L, Regueme SC, Forestier N (2011) Effects of unilateral fatigue of triceps surae on undisturbed stance. Clin Neurophysiol 41:61-65.
Berger LL, Regueme SC, Forestier N (2010) Unilateral lower limb muscle fatigue induces bilateral effects on undisturbed stance and muscle EMG activities. J Electromyogr Kinesiol 20:947-952.
Bigland-Ritchie B, Woods JJ (1984) Changes in muscle contractile properties and neural control during human muscular fatigue. Muscle Nerve 7:691-699.
Borel S, Schneider P, Newman CJ (2011) Video analysis software increases the interrater reliability of video gait assessments in children with cerebral palsy. Gait Posture 33:727-729.
Caron O (2003) Effects of local fatigue of the lower limbs on postural control and postural stability in standing posture. Neurosci Lett 340:83-86.
Dickin DC, Doan JB (2008) Postural stability in altered and unaltered sensory environments following fatiguing exercise of lower extremity joints. Scand J Med Sci Sports 18:765-772.
Dingenen B, Malfait B, Vanrenterghem J, Verschueren SM, Staes FF (2014) The reliability and validity of the measurement of lateral trunk motion in two-dimensional video analysis during unipodal functional screening tests in elite female athletes. Phys Ther Sport 15:117-123.
Dingenen B, Malfait B, Nijs S, Peers KH, Vereecken S, Verschueren SM, Staes FF (2015) Can two-dimensional video analysis during single-leg drop vertical jumps help identify non-contact knee injury risk? A one-year prospective study. Clin Biomech 30:781-787.
Enoka RM, Stuart DG (1992) Neurobiology of muscle fatigue. J Appl Physiol (1985) 72:1631-1648.
Flansbjer UB, Downham D, Lexell J (2006) Knee muscle strength, gait performance, and perceived participation after stroke. Arch Phys Med Rehabil 87:974-980.
Gribble PA, Hertel J (2004) Effect of lower-extremity muscle fatigue on postural control. Arch Phys Med Rehabil 85:589-592.
Gribble PA, Hertel J, Denegar CR, Buckley WE (2004) The effects of fatigue and chronic ankle instability on dynamic postural control. J Athl Train 39:321-329.
Hackett ML, Anderson CS (2005) Predictors of depression after stroke: a systematic review of observational studies. Stroke 36:2296-2301.
Harkins KM, Mattacola CG, Uhl TL, Malone TR, McCrory JL (2005) Effects of 2 ankle fatigue models on the duration of postural stability dysfunction. J Athl Train 40:191-194.
Hassanlouei H, Arendt-Nielsen L, Kersting UG, Falla D (2012) Effect of exercise-induced fatigue on postural control of the knee. J Electromyogr Kinesiol 22:342-347.
Hatton AL, Menant JC, Lord SR, Lo JC, Sturnieks DL (2013) The effect of lower limb muscle fatigue on obstacle negotiation during walking in older adults. Gait Posture 37:506-510.
Hyngstrom AS, Onushko T, Heitz RP, Rutkowski A, Hunter SK, Schmit BD (2012) Stroke-related changes in neuromuscular fatigue of the hip flexors and functional implications. Am J Phys Med Rehabil 91:33-42.
Ikai T, Kamikubo T, Takehara I, Nishi M, Miyano S (2003) Dynamic postural control in patients with hemiparesis. Am J Phys Med Rehabil 82:463-469; quiz 470-462, 484.
Kanekar N, Santos MJ, Aruin AS (2008) Anticipatory postural control following fatigue of postural and focal muscles. Clin Neurophysiol 119:2304-2313.
Kwon YH, Kim CS, Jang SH (2007) Ipsi-lesional motor deficits in hemiparetic patients with stroke. NeuroRehabilitation 22:279-286.
Lin D, Nussbaum MA, Seol H, Singh NB, Madigan ML, Wojcik LA (2009) Acute effects of localized muscle fatigue on postural control and patterns of recovery during upright stance: influence of fatigue location and age. Eur J Appl Physiol 106:425-434.
Lisinski P, Huber J, Gajewska E, Szlapinski P (2012) The body balance training effect on improvement of motor functions in paretic extremities in patients after stroke. A randomized, single blinded trial. Clin Neurol Neurosurg 114:31-36.
Murdock GH, Hubley-Kozey CL (2012) Effect of a high intensity quadriceps fatigue protocol on knee joint mechanics and muscle activation during gait in young adults. Eur J Appl Physiol 112:439-449.
Negahban H, Etemadi M, Naghibi S, Emrani A, Shaterzadeh Yazdi MJ, Salehi R, Moradi Bousari A (2013) The effects of muscle fatigue on dynamic standing balance in people with and without patellofemoral pain syndrome. Gait Posture 37:336-339.
Paillard T, Chaubet V, Maitre J, Dumitrescu M, Borel L (2010) Disturbance of contralateral unipedal postural control after stimulated and voluntary contractions of the ipsilateral limb. Neurosci Res 68:301-306.
Paolucci S, Caltagirone C, Mastrilli F, Sandrini G, Nappi G (2003) Planning availability in stroke rehabilitation units. Funct Neurol 18:191-194.
Parijat P, Lockhart TE (2008) Effects of quadriceps fatigue on the biomechanics of gait and slip propensity. Gait Posture 28:568-573.
Park J, Yim J (2016) A new approach to improve cognition, muscle strength, and postural balance in community-dwelling elderly with a 3-D virtual Reality Kkayak Program. Tohoku J Exp Med 238:1-8.
Reimer RC, 3rd, Wikstrom EA (2010) Functional fatigue of the hip and ankle musculature cause similar alterations in single leg stance postural control. J Sci Med Sport 13:161-166.
Rybar MM, Walker ER, Kuhnen HR, Ouellette DR, Berrios R, Hunter SK, Hyngstrom AS (2014) The stroke-related effects of hip flexion fatigue on over ground walking. Gait Posture 39:1103-1108.
Salavati M, Moghadam M, Ebrahimi I, Arab AM (2007) Changes in postural stability with fatigue of lower extremity frontal and sagittal plane movers. Gait Posture 26:214-218.
Son SM, Kwon YH, Lee NK, Nam SH, Kim K (2013) Deficits of movement accuracy and proprioceptive sense in the ipsi-lesional upper limb of patients with hemiparetic stroke. J Phys Ther Sci 25:567-569.
Springer BK, Pincivero DM (2009) The effects of localized muscle and whole-body fatigue on single-leg balance between healthy men and women. Gait Posture 30:50-54.
St Clair Gibson A, Noakes TD (2004) Evidence for complex system integration and dynamic neural regulation of skeletal muscle recruitment during exercise in humans. Br J Sports Med 38:797-806.
St Clair Gibson A, Lambert ML, Noakes TD (2001) Neural control of force output during maximal and submaximal exercise. Sports Med 31:637-650.
Vuillerme N, Boisgontier M (2010) Changes in the relative contribution of each leg to the control of quiet two-legged stance following unilateral plantar-flexor muscles fatigue. Eur J Appl Physiol 110:207-213.
Vuillerme N, Sporbert C, Pinsault N (2009) Postural adaptation to unilateral hip muscle fatigue during human bipedal standing. Gait Posture 30:122-125.
Vuillerme N, Burdet C, Isableu B, Demetz S (2006) The magnitude of the effect of calf muscles fatigue on postural control during bipedal quiet standing with vision depends on the eye-visual target distance. Gait Posture 24:169-172.
Walter JP, D’Lima DD, Colwell CW Jr, Fregly BJ (2010) Decreased knee adduction moment does not guarantee decreased medial contact force during gait. J Orthop Res 28:1348-1354.
Yeung SS, Au AL, Chow CC (1999) Effects of fatigue on the temporal neuromuscular control of vastus medialis muscle in humans. Eur J Appl Physiol Occup Physiol 80:379-385.
Copyedited by Li CH, Song LP, Zhao M
*< class="emphasis_italic">Correspondence to: Na Kyung Lee, P.T., Ph.D., dlskrud21@hanmail.net.
Na Kyung Lee, P.T., Ph.D., dlskrud21@hanmail.net.
orcid: 0000-0002-2678-9121 (Na Kyung Lee)
10.4103/1673-5374.206647
Accepted: 2017-04-18
杂志排行

中国神经再生研究(英文版)的其它文章
- Cerebral mechanism of puncturing at He-Mu point combination for functional dyspepsia: study protocol for a randomized controlled parallel trial
- Therapeutic opportunities and challenges of induced pluripotent stem cells-derived motor neurons for treatment of amyotrophic lateral sclerosis and motor neuron disease
- Inhibition and enhancement of neural regeneration by chondroitin sulfate proteoglycans
- Collapsin response mediator protein-2 plays a major protective role in acute axonal degeneration
- Hypoxia inducible factor-1 alpha stabilization for regenerative therapy in traumatic brain injury
- Minocycline targets multiple secondary injury mechanisms in traumatic spinal cord injury