急性ST段抬高型心肌梗死患者行急诊PCI无复流的危险因素分析
2016-12-19袁驰柯永胜柯可
袁驰,柯永胜,柯可
· 论著 ·
急性ST段抬高型心肌梗死患者行急诊PCI无复流的危险因素分析
袁驰1,柯永胜1,柯可2
目的 分析急性ST段抬高型心肌梗死(STEMI)患者行急诊经皮冠状动脉介入治疗(PCI)后出现无复流的相关危险因素。方法 选择2012年5月~12月于皖南医学院第一附属弋矶山医院心内科就诊STEMI且行急诊PCI的患者166例,其中男性139例,女性27例,年龄36~91(63.10±11.96)岁。按照血管机械开通后的造影情况分为正常灌注组(142例)和无复流组(24例)。采集患者缺血时间、合并基础疾病等一般临床资料,入院即刻和入院后采静脉血,检测中性粒细胞百分比、血小板计数(PLT)、低密度脂蛋白胆固醇(LDL-C)水平等,测定病变血管直径和靶病变长度。结果 无复流组缺血时间和中性粒细胞百分比均高于正常灌注组,差异有统计学意义(P均<0.01)。结果显示,缺血时间>6 h(OR=1.578,95%CI:1.245~2.000)和中性粒细胞百分比>80.0%(OR=3.405,95%CI:1.027~11.293)均为急诊PCI术后无复流的危险因素。结论 急性ST段抬高型心肌梗死行急诊PCI的患者,缺血时间明显延长,中性粒细胞百分比明显升高,发生无复流的概率会更高。
急性ST段抬高型心肌梗死;急诊PCI;无复流
急性ST段抬高型心肌梗死(STEMI)是最常见的致死原因之一[1]。对于STEMI患者,尽管行急诊经皮冠状动脉介入治疗(PCI)是最理想的治疗策略,但无复流发生率为15%~60%[2]。无复流定义为行PCI后,尽管梗死相关血管开通,但心肌组织无血流灌注[3]。无复流可导致心肌梗死面积扩大、脑卒中、负性左室重构、心力衰竭及死亡率增高等一系列恶性临床事件,降低PCI带来的获益[4-6]。目前无复流的机制尚未完全阐明,多数学者认为由微血管栓塞、远端栓塞、微血管痉挛等导致[3]。同时涉及多种因素,包括内皮损伤、微血管损伤、血小板和中性粒细胞以及内皮细胞的互相作用[7]。本研究主要回顾分析了STEMI行急诊PCI出现无复流的危险因素,为临床防治提供依据。
1 资料与方法
1.1 研究对象和分组 选择2012年5月~12月于皖南医学院第一附属弋矶山医院心内科就诊STEMI且行PCI的患者166例,其中男性139例,女性27例,年龄36~91岁,平均63.10±11.96。所有患者均在发病12 h内入院,确诊为STEMI,诊断标准参考第3版《心肌梗死通用定义》[8]。无复流定义为尽管罪犯血管开通,但造影时TIMI血流≤2级[9]。排除标准:①NSTEMI患者;②由于血管钙化等原因,未能成功置入支架的患者;③存在血液系统疾病的患者;④既往行PCI患者;⑤合并严重的感染、甲亢、癌症、自身免疫病等;⑥数据不完整,影响统计分析的患者。按照血管机械开通后的造影情况分为正常灌注组(n=142)和无复流组(n=24)。
1.2 主要观察指标 采集患者入院后病史资料,如缺血时间、合并基础疾病等。所有患者均于急诊PCI前抽取静脉血,采用SYSMEX-XT1800i全自动血细胞分析仪,检测中性粒细胞百分比、血小板计数(PLT)、血小板平均容积(MPV)。入院后择期采静脉血,采用HITACHI 7600全自动生化分析仪(试剂由HITACHI公司提供)检测低密度脂蛋白胆固醇(LDL-C)水平,行PCI时观测病变血管直径和靶病变长度。
1.3 急诊PCI 术前常规嚼服阿司匹林300 mg和氯吡格雷300 mg,结合心电图表现判断病变血管,若病变血管可见血栓影,使用抽吸导管抽吸血栓,并经导管推注GP IIb/IIIa 受体拮抗剂(替罗非班)。术后皮下注射低分子肝素5~7 d,口服阿司匹林100 mg/d,氯吡格雷75 mg/d,口服血管紧张素转化酶抑制剂、β受体阻滞剂(若无低血压、显著心动过缓等禁忌)和他汀类药物。
1.4 统计学处理 所有的数据均采用SPSS 19.0统计软件进行分析。计量资料采用均数±标准差(±s)表示,两组间均数的比较采用t检验,计数资料采用例数(构成比)表示,组间比较采用χ2检验。采用Logistic回归分析急诊PCI后无复流的影响因素。P<0.05为差异有统计学意义。
2 结果
2.1 两组临床资料比较 无复流组与正常灌注组在冠状动脉病变支数、病变血管直径、靶病变长度、PLT、MPV、LDL-C等方面比较,差异无统计学意义(P均>0.05)。在无复流组中,未观察到罪犯血管为回旋支、左主干。无复流组缺血时间和中性粒细胞百分比均高于正常灌注组,差异有统计学意义(P均<0.01)(表1)。
2.2 多因素Logistic回归分析 为进一步排除混杂因素的影响,以急诊PCI后是否出现无复流作为因变量,引入单因素分析有显著差异的因素进行Logistic回归分析。结果显示:缺血时间>6 h(OR=1.578,95%CI:1.245~2.000)和中性粒细胞百分比>80.0%(OR=3.405,95%CI:1.027~11.293)均为急诊PCI术后无复流的危险因素(表2)。
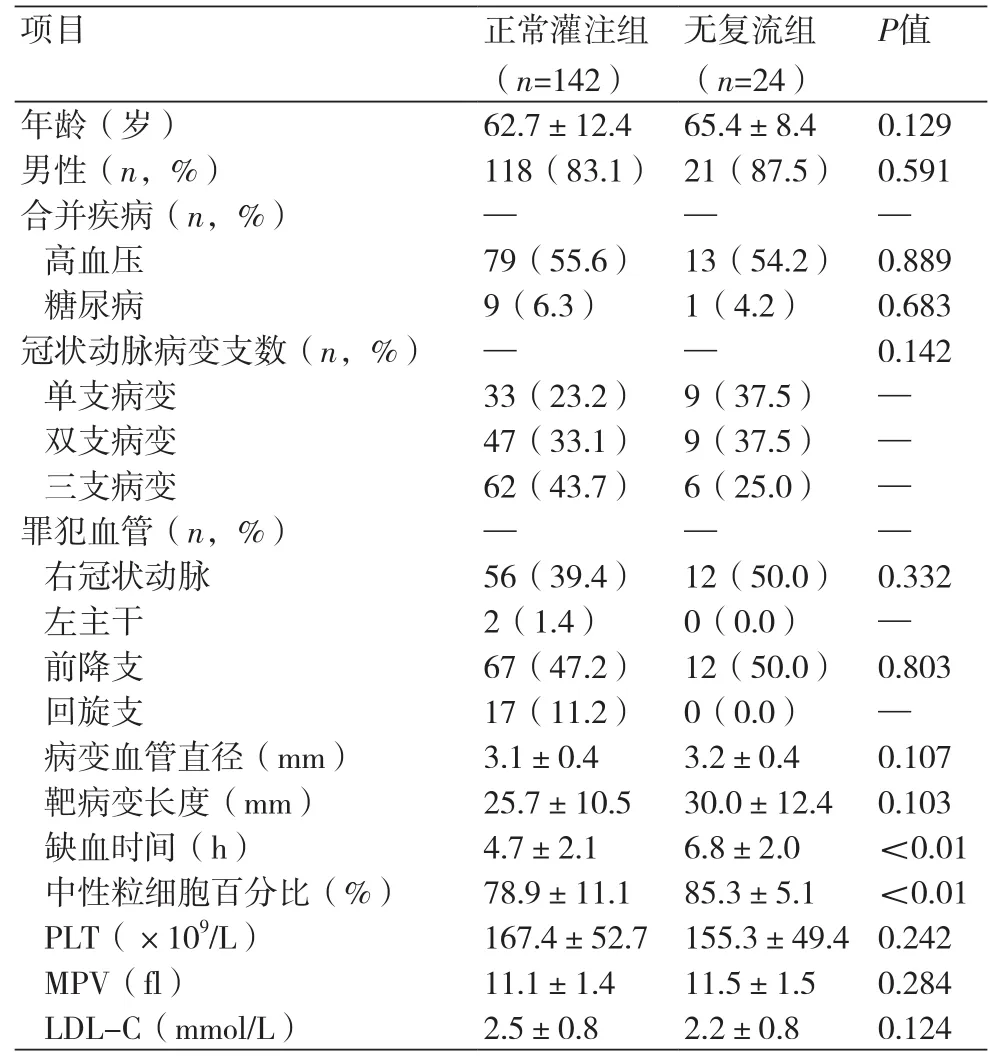
表1 两组患者临床资料比较

表2 无复流发生的多因素回归分析
3 讨论
无复流与心肌梗死面积大小、近期以及远期的死亡率有关,预测预后[10]。本研究的无复流发生率为14.5%,与之前文献报道基本相符[2]。冠状动脉闭塞引起心肌缺血可导致氧自由基增多,进而导致心肌细胞结构改变和代谢紊乱,同时也会引起胞质和线粒体内钙超载,进一步加重细胞膜降解[11]。Iwakura等[12]研究发现,由缺血相关损伤导致的冠状动脉微血管栓塞中,缺血时间起重要作用。通过观察发现,冠状动脉闭塞90 min后再灌注,导致严重的毛细血管损伤,内皮细胞突起以致阻塞毛细血管腔,血管外红细胞也将堵塞内皮细胞间隙[13]。当持续缺血时间超过3 h,再灌注可加重缺血相关损伤[14]。缺血时间延长在致死性再灌注损伤(再灌注引起的心肌坏死)和冠状动脉微血管栓塞中尤为关键[15]。冠状动脉栓塞通过引起中性粒细胞和血小板聚集,又产生大量收缩血管物质和炎症介质。
另外本研究亦提示,中性粒细胞百分比升高更容易发生无复流。冠状动脉硬化是炎症反应的过程,而炎症标志物可以作为预测临床结局的因子[16]。在冠状动脉疾病患者中,炎症因子的增加可能加剧病情[17]。受损心肌区域首先出现的是中性粒细胞,促凝物质由局部的白细胞释放,这增加了氧化损伤和蛋白水解损伤[18]。此外,中性粒细胞浸润可增加血液粘滞度,增加无复流发生。
总之,无复流现象有着复杂的病理生理学特点,可能还与患者的临床特征、影像学特征以及手术方式有关。本研究存在以下不足:①未观察评价心肌灌注的其他影像学特征,如心肌显像积分和TIMI帧计数等;②入选的病例数仍然偏少,且入选病例行PCI并非同一术者;③本研究是单中心、小样本的回顾性研究,因此仍需大样本、多中心、前瞻性、随机临床试验来证实本研究结论的可靠性。
[1] 卫生部心血管病防治研究中心. 中国心血管病报告[M]. 中国大百科全书出版社,2013.
[2] Carrick D,Oldroyd KG,McEntegart M,et al. A randomized trial of deferred stenting versus immediate stenting to prevent no- or slowreflow in acute ST-segment elevation myocardial infarction (DEFER-STEMI)[J]. J Am Coll Cardiol,2014,63(20):2088-98.
[3] Jaffe R,Charron T,Puley G,et al. Strauss BH. Microvascular obstruction and the no-reflow phenomenon after percutaneous coronary intervention[J]. Circulation,2008,117(24):3152-6.
[4] Morishima I,Sone T,Okumura K,et al. Angiographic no-reflow phenomenon as a predictor of adverse long-term outcome in patients treated with percutaneous transluminal coronary angioplasty for first acute myocardial infarction[J]. J Am Coll Cardiol,2000,36(4):1202-9.
[5] Harrison RW,Aggarwal A,Ou F,et al. Incidence and outcomes of noreflow phenomenon during percutaneous coronary intervention among patients with acute myocardial infarction[J]. J Am Cardiol,2012,111 (2):178-84.
[6] Ndrepepa G,Tiroch K,Fusaro M,et al. 5-year prognostic value of noreflow phenomenon after percutaneous coronary intervention in patients with acute myocardial infarction[J]. J Am Coll Cardiol,2010, 55(21):2383-9.
[7] Muller O,Trana C,Eeckhout E. Myocardial no-reflow treatment[J]. Cur Vasc Pharmacol,2013,11(2):278-85.
[8] Thygesen K,Alpert JS,Jaffe AS,et al. Third universal definition of myocardial infarction[J]. J Am Coll Cardiol,2012,60(16):1581-98.
[9] Niccoli G,Burzotta F,Galiuto L,et al. Myocardial No-Reflow in Humans[J]. J Am Coll Cardiol, 2009,54(4):281-92.
[10] Brosh D,Assali AR,Mager A,et al. Effect of no-reflow during primary percutaneous coronary intervention for acute myocardial infarction on six-month mortality[J]. J Am Cardiol,2007,99(4):442-5
[11] Reimer KA,Hill ML,Jennings RB. Prolonged depletion of ATP and of the adenine nucleotide pool due to delayed resynthesis of adenine nucleotides following reversible myocardial ischemic injury in dogs[J]. J Mol Cell Cardiol,1981,13(2):229-39.
[12] Iwakura K,Ito H,Kawano S,et al. Prediction of the no-reflow phenomenon with ultrasonic tissue characterization in patients with anterior wall acute myocardial infarction[J]. J Am Cardiol,2004,93 (11):1357-61.
[13] Reffelmann T,Kloner RA. The no-reflow phenomenon: a basic mechanism of myocardial ischemia and reperfusion[J]. Basic Res Cardiol,2006,101(5):359-72.
[14] Frohlich GM,Meier P,White SK,et al. Myocardial reperfusion injury: looking beyond primary PCI[J]. Eur Heart J,2013,34(23):1714-22.
[15] Bekkers SC,Yazdani SK,Virmani R,et al. Microvascular obstruction: underlying pathophysiology and clinical diagnosis[J]. J Am Coll Cardiol,2010,55(16):1649-60.
[16] Korkmaz L,Kul S,Korkmaz AA,et al. Increased leucocyte count could predict coronary artery calcification in patients free of clinically apparent cardiovascular disease[J]. Turk Kardiyol Dern Ars,2012,40(3):223-8.
[17] Arbel Y,Halkin A,Birati EY,et al. Neutrophil/lymphocyte ratio is related to the severity of coronary artery disease and clinical outcome in patients undergoing angiography[J]. Atherosclerosis,2012,225(2): 456-60.
[18] Ducloux D,Challier B,Saas P,et al. CD4 cell lymphopenia and atherosclerosis in renal transplant recipients[J]. J Am Soc Nephrol, 2003,14(3):767-72.
本文编辑:姚雪莉
Risk factors of no-reflow during primary percutaneous coronary intervention in patients with acute ST-segment elevation myocardial infarction
YUAN Chi*, KE Yong-sheng, KE Ke.*Department of Cardiovascular Diseases, Yijishan Hospital, Wannan Medical College, Wuhu 241000, China.
Objective To analyze the relevant risk factors of no-reflow during primary percutaneous coronary intervention (PCI) in patients with acute ST-segment elevation myocardial infarction (STEMI). Methods STEMI patients undergone primary PCI were chosen (n=166, male 139, female 27, aged from 36 to 91 and average age=63.10±11.96) from the Department of Cardiovascular Diseases of the First Affiliated Yijishan Hospital of Wannan Medical College from May 2012 to Dec. 2015. All patients were divided into normal perfusion group (n=142) and no-reflow group (n=24) according to the outcomes of angiography after vascular mechanical patency. The general clinical materials including ischemia time and complicating basic diseases were collected. The samples of vein blood were collected at the time of hospitalization and after hospital admission for detecting neutrophil percentage, platelet count (PLT) and low-density lipoprotein-cholesterol (LDL-C), and diseased vascular diameter and target lesion length were measured. Results The ischemia time and neutrophil percentage were all higher in no-reflow group than those in normal perfusion group (all P<0.01). The results of regression analysis showed that ischemia time>6 h (OR=1.578, 95%CI: 1.245~2.000) and neutrophil percentage>80.0% (OR=3.405, 95%CI: 1.027~11.293) were risk factors of no-reflow after primary PCI. Conclusion In the patients with acute STEMI undergone primary PCI, ischemia time is longer and neutrophil percentage increases significantly and probability of no-reflow will be higher.
Acute ST-segment elevation myocardial infarction; Primary percutaneous coronary intervention; No-reflow
R541.4
A
1674-4055(2016)11-1354-03
1241000 芜湖,皖南医学院弋矶山医院心血管内科;2102249 北京,中国人民解放军装备学院昌平士官学校门诊部
柯永胜,E-mail:keyongsheng@163.com
10.3969/j.issn.1674-4055.2016.11.20
