Work-related ocular injuries in Johor Bahru,Malaysia
2016-11-16NyoNyoMinSureshKumarVasudevanAzlynAzwabintiJasmanAisyahbintiAliKayThiMyint
Nyo Nyo Min,Suresh Kumar Vasudevan,Azlyn Azwabinti Jasman,Aisyahbinti Ali,Kay Thi Myint
·Original article·
Work-related ocular injuries in Johor Bahru,Malaysia
Nyo Nyo Min1,Suresh Kumar Vasudevan2,Azlyn Azwabinti Jasman1,Aisyahbinti Ali3,Kay Thi Myint4
1Department of Ophthalmology,Hospital Sultan Ismail,Johor Bahru 81110,Malaysia
2Department of Ophthalmology,Hospital Sultanah Aminah,Johor Bahru 80100,Malaysia
3Clinical Research Centre,Hospital Sultan Ismail,Johor Bahru 81110,Malaysia
4Faculty of Medicine,SEGi University,Sibu campus,Sibu 96000,Sarawak,Malaysia
Correspondence to:Kay Thi Myint.Faculty of Medicine,SEGi University Sibu campus NQ1 Flat,Hospital Sibu,Sibu 96000,Sarawak,Malaysia.kaythimyint.eye@gmail.com
目的:调查马来西亚南部三级医院的工作相关眼外伤的流行病学与其视力情况。
方法:回顾性调查研究。选取2011年1月至2013年12月在马来西亚新山市Sultan Ismail医院就诊的工作相关眼外伤患者的病历资料。运用标准表格形式收集临床表现,损伤种类,眼部保护装置的使用和视力情况等数据。
结果:在3y内共935例眼外伤患者于Sultan Ismail医院就诊,其中440例为工作相关眼外伤,且男性占绝大多数(98.19%),常见年龄在21y至30y之间(45%)。最常见的损伤种类为眼表损伤(70.9%),其次是化学损伤(11.13%),开放性眼外伤(8.4%),闭合性眼外伤(6.83%)和热灼伤(2.7%)。虽然工作相关眼外伤普遍为当地人(78.5%),但其中三分之二的开放性眼外伤出现在外来劳工中。仅59例患者(13.4%)在受伤时配戴眼部保护装置。通常89.9%(n=399)的患者视力良好,5.45%(n=24)的患者视力一般,3.86%(n=17)的患者视力较差。视力预后与损伤类型的相关性分析表明,开放性眼外伤的视力较闭合性眼外伤差(OR=3.33,95%CI= 0.68-16.33)。2011/2013年,工作相关眼外伤新病例的整体就诊率为20.7‰~51.9‰,大约每年下降1.5%(P<0.05)。相比之下,工作相关眼外伤住院患者在3y期间有所增加。工作相关眼外伤致单眼盲或低视力患者(最佳矫正视力≤3/60)约占就诊人数的1.26‰(95%可信区间为0.74至2.02)。
结论:工作相关眼外伤是致从业人员眼病的重要原因,特别是年轻人。当地21y到40y的男性为高危人群。大多数我院接收的工作相关眼外伤患者均为可避免的眼表损伤。本研究表明劳工们需要加强安全措施,预防意外失明,避免增加社会经济负担。除此之外,还需建立眼损伤信息记录系统。
引用:Min NN,Vasudevan SK,Azlyn AJ,Aisyah A,Myint KT.
马来西亚新山市工作相关眼外伤调查分析.国际眼科杂志2016;16(3):416-422
·AIM:To describe the epidemiology of work-related ocular injuries and its visual outcome in tertiary hospital in southern Malaysia.
·METHODS:Retrospective review of medical records of patients diagnosed as work-related ocular injuries who attended to the eye casualty of Hospital Sultan Ismail in Johor Bahru,Malaysia from Jan.2011 to Dec.2013.Data for clinical presentation,types of injuries,use of eye protectivedevice(EPD)andvisualoutcomewere collected using a standardized proforma.
·RESULTS:A total of 935 ocular injuries attended to Hospital Sultan Ismail during 3y period.Among them 440 cases were work-related ocular injuries and included in the study.There was significant male preponderance(98. 19%)and commonest age group affected was 21 to 30y(45%).The most common type of injury was superficial injuries(70.91%),followed by chemical(11.13%),open globe(8.41%),closed globe(6.83%)and thermal(2.72%).Although Malays are commonly involved in work-related ocular injury accounted for 78.47%,twothirds ofopenglobeinjurieswereseeninforeign workers.Only 59 patients(13.41%)reported that they wore EPD at the time of incident.Generally,89.86%(n= 399)had good vision,5.45%(n=24)had moderate vision and 3.86%(n=17)poor vision.Visual outcome related to specific types of injuries showed that poor outcomewashigherinopenglobeinjuriesgroups compared with closed globe injuries[odd ratio(OR)= 3.33,95%confidence interval(CI)=0.68 to 16.33]. Overall hospital attendance rate of work-related ocular trauma ranged from 20.7 to 51.9 per 1000 new cases and decline of approximately 1.5%per year(P<0.05)from 2011 to 2013.In contrast,the in-patient admission due to work-related ocular injuries increased over 3y period. Estimated rate of monocular blindness or low vision[best-corrected visual acuity(BCVA)≤3/60]due to workrelated ocular injury was 1.26 per 1000 hospital attendance(95%CI=0.74 to 2.02).
·CONCLUSION:Work-related ocular trauma is important cause of ocular morbidity in working forces particularly young men.Malay males between 21 to 40y have higher risk.Majority of work-related ocular trauma seen in our hospital are generally of superficial injuries and potentially preventable.This study indicates they need to improve safety measures to prevent undesirable sight loss and economic burden to society as well as to establish for eye injury registry.
work-related;eye injuries;protective devices;visual outcome
INTRODUCTION
O cular injury is a major cause of monocular blindness and visual impairment throughout the world.It is one of the common reasons for extended hospitalization of ophthalmic patients particularly in industrialized nations[1].Globally,there areapproximately 1.6millionpeopleblind,an additional 2.3 million people with bilateral low vision,and almost 19 million with unilateral blindness or low vision resulting from eye injuries[2].The spectrum of injuries ranges from very mild,non-sight threatening to extremely serious with potentially blinding consequences.A significant portion of ocular injuries occur in workplace.The United States National Safety Council estimated that job-related injuries account for approximately one-third of all eye injuries[3].A prospective study conducted in east Malaysia reported that work-related injuries accounted for 36.9%of all ocular traumas[4].However,Singapore reported higher percentage of work-related injuries as 71.4%of total ocular trauma attended the eye casualty in which industrial related activities such as grinding,cutting metals and drilling accounted for more than 90%[5].
We conducted a hospital-based retrospective study in Johor Bahru,a capital city of Johor State in the southern part of Malaysiawith1.38millionpopulations,whichis approximately 40%of the population of the entire state[6].It is an industrial,commercial city and its major industries include construction,electric,chemical processing plants and petrochemical refinery aswellasagricultureindustries. Although no one is free from risk of injuries,industrial workers are at high risk depending on nature of their job. Moreover,majority of ocular injuries are seen in working age group and are preventable.It may lead to permanent disability from loss of eye sight and loss of productivity which in turn will have an economic impact to the country[2].
To date,published data for work-related injury is still lacking particularly in developing countries.This study aims to present the profile of work-related ocular injuries in a hospital setting,identifying types of injury as well as to assess the visual outcomes.
SUBJECTS AND METHODS
This study was conducted in accordance to the tenets of the Declaration of Helsinki.The study protocol was approved by Medical Research Ethics Committee,Malaysian Ministry of Health(National Medical Research Registry ID:NMRR-14-379-19613).
This is a retrospective review of medical records of patients diagnosed as work-related ocular injuries who attended to the eye casualty of Hospital Sultan Ismail in Johor Bahru,Malaysia from Jan.2011 to Dec.2013.We designed a standardized proforma to retrieve the following data:1)demographic information including age,sex,nationality and ethnicity;2)nature of injury(laterality,type of injury,clinical diagnosis);3)visualacuityatthetimeof presentation and at least one follow up.The visual outcome was graded as good(best corrected visual acuity≥6/12),moderate(6/18 to 6/60)and poor(worse than 6/60)by using Snellen chart;4)management:medical or surgical;5)the use of eye protective devices(EPD).
Work-related ocular injury was defined as any injury or foreign body to eye as well as ocular adnexa which occurred at work.We excluded all other injuries that occurred outside work places such as resident-related,sport-related,accidents and assaults.Nationality of patients was identified as Malaysian if they have Malaysian identity card and if not,as non-Malaysian.For Malaysian,ethnicity was classified into four groups namely Malays,Chinese,Indian and Others(which include Iban,Sabahan and Orang Asli).Non-Malaysians were foreigners working in Johor Bahru.The use of EPD was documented as yes or no.
Types of injuries were classified as:1)superficial injuries which include foreign body cornea or ocular adnexa and corneal abrasion or lid injuries;2)chemical injuries;3)thermal injuries;4)mechanical injuries for which we adopted theBirminghamEyeTraumaTerminology(BETT)classification[7]as;closed globe injury(CGI)in which no full-thickness wound of eye wall and open globe injury(OGI)if associated with full-thickness wound of eye wall. Data were analyzed using SPSS(version 16.0,USA).
RESULTS
A total of 935 ocular trauma cases attended the eye casualty in Hospital Sultan Ismail from Jan.2011 to Dec.2013(Figure 1).Among them,440 patients(47.05%)were associated with work-related eye injuries with 10%(n=45)of them being admitted as in-patient.Details of work-related ocular injuries in this study are shown in Table 1.There was significant male preponderance(98.19%vs 1.81%),commonest age group affected was 21-30y(ranged 18 to 66y)and Malays(78.47%)had higher injury rates than other ethnicities.For non-residents,the most common country of origin was Indonesia followed by Bangladesh and Nepal.The most frequent diagnosis was superficial injuries(70.91%).Only 59 patients(13.41%)reported that they wore EPD at the time of incident compared to 381(86.59%)who did not wear it.
The majority of cases(94.09%)sustained unilateral trauma and only 26 patients(5.91%)had bilateral involvement accounting for a total of 466 eyes of 440 patients.Among the bilateral cases,14 were chemical injuries,10 thermal,1 blunt trauma and 1 bilateral corneal foreign body.Among close globe injuries(CGI),there were 4 reported cases of traumatic optic neuropathy,2 cases of commotio retinae,2 cases of retinal detachment and rest were traumatic hyphema with uveitis.Out of 37 open globe injuries(OGI),4 cases were associated with intraocular foreign bodies in anterior chamber.All cases involved in OGI were male with 72.97% in 21 to 40y age group.Approximately two-third(67.8%)were foreign workers.A detail of OGI cases was shown in Table 2.
A total of 44 cases underwent surgical intervention including 37 OGI,5 eyelid lacerations and 2 traumatic cataracts after CGI.Twelve patients were referred for further consultation. Final visual outcome was analysed as full analysis set which showed 89.86%(n=399)had good vision,5.45%(n= 24)had moderate vision and 3.86%(n=17)poor vision at follow-up period of 1wk to 1y.Visual outcome related to specific types of injuries showed that poor outcome was higher in OGI groups compared with CGI[odd ratio(OR)=3.33,95%confidence interval(CI)=0.68 to 16.33(Figure 2)]. Overall hospital attendance rate of work-related ocular trauma ranged from 20.7 to 51.9 per 1000 new cases and decline of approximately 1.5%per year(P<0.05)from 2011 to 2013(Table 3).In contrast,the in-patient admission due to workrelated ocular injuries increased over 3y period(Table 4). Estimated rate of monocular blindness or low vision(BCVA≤3/60)due to work-related ocular injury was 1.26 per 1000 hospital attendance(95%CI=0.74 to 2.02).

Table 1 Characteristics of work-related ocular trauma cases in Hospital Sultan Ismail(2011-2013)
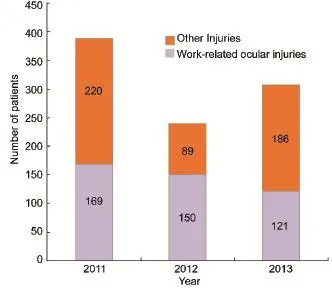
Figure 1 Hospital attendance of ocular injuries in Hospital Sultan Ismail,Johor Bahru from Jan.2011 to Dec.2013.
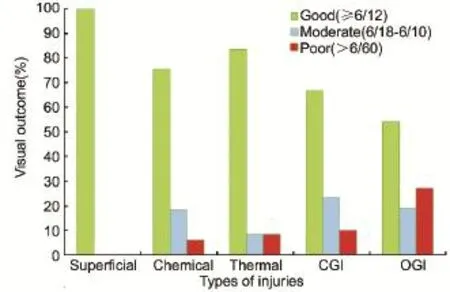
Figure 2 Visual outcome related to specific types of injuries.

Table 2 Characteristics of open globe injuries in Hospital Sultan Ismail(2011-2013)(n=37,all males)

Table 3 Estimated hospital attendance rate of total and work-related ocular injuries

Table 4 Estimated in-patient admission rate of total and work-related ocular injuries
DISCUSSION
Ocular trauma in developing countries is still under-reported. The impact of ocular injuries is enormous,not only to the affected individual,alsotothehealthcaresystemand society[8].Work-related injuries are particularly important as it has significant economic implication since it affects the working age group and there are potential for effective prevention[9].Several reasons may account for the decline in rate of work-related eye injury during 3y period in our hospital which serves as a secondary eye care centre for approximately half of the population in the area.It may be partly due to change of work place,or more credible explanation is some cases particularly superficial injuries sought treatment at primary care physicians as well as private practice ophthalmologists.
Our study revealed that work-related injury accounts for almost half(47.05%)of all ocular injuries attended to the eye casualty.Recent studies from Asia-Pacific countries reported that work-related injuries to the eye accounted for substantial portion of all eye injuries;71.4%and 56%from Singapore in 2001 and 2006 respectively[5,10],56%from India in 2006[11],36.9%from East Malaysia in 2008[4],38.9%from Taiwan in 2007[12],44%from Malaysia in 2011[13],47%from China in 2012[14]and 49.8%from Thailand in 2014[15].Similar to the other studies from Malaysia[4,13],Malays are most commonly affected ethnic group;whereas,in Singapore,a neighbour of Johor,it was reported that majority of work-related ocular injuries were among non-resident foreign workers[5].Our data also follows the almost universal pattern of work-related ocular injuries,that is significant association with male gender and age group 21-40y[4-5,16-18].
Superficial injuries such as foreign body cornea or adnexa were the commonest injuries(70.01%)which agreed with many other studies[5,10,19].Although visual recovery was excellent in most of the superficial injuries the impact should not be underestimated.All corneal foreign bodies are potentially sight threatening from possible infection.It was estimated that median time loss of 4h from work in approximately 70%of patients with corneal foreign bodies[20].
Ocular surface burns were the second most common types with 49 chemical and 12 thermal burns.There were 11.13%of chemical burns in this study.Recent studies reported the incidence of work-related chemical injuries to the eye at 8 to 19.6%[10,12,18].Those involved in chemical burns were from manufacturing,chemical and petroleum industries whereas thermal burns were seen in construction and food industries with exposure to welding,flame,cooking oil or other liquid. There were more alkali burns(33 alkalis vs 16 acids)and common agents implicated were caustic soda,aluminium hydroxide,lime water or calcium hydroxide and sodium silicate.Apart from only 3 patients with severe chemical burns of grade 3 or 4,the rest were either grade 1 or chemical conjunctivitis with good visual outcome.In thermal burns,those who worked in food industries had associated burns in eyelids and other parts of the body such as face or hands.One patient involved in gas cylinder explosion had periorbital burns with corneal abrasion.One case was referred due to severe thermal burn with swollen lids and opaque cornea.Other cases had good visual outcome better than 6/12.Usually there are favourable outcome in majority of patients with thermal ocular injuries[21].Direct thermal burns to eyes secondary to facial burns may lead to lid damage and corneal complications which may necessitate longer follow-ups.
Mechanical injuries to eye accounted for total of 67(30 CGI vs 37 OGI)in this study.There were 2 cases of phthisis and 2 cases(6.89%)of evisceration in OGI group.Usually,for all OGI,systemic antibiotic is routinely given as intravenous ciprofloxacin 400 mg bid for 3-5d followed by oral for 14d. ThoseOGIwithlaceratedwoundcorneaweregiven intracameral cefuroxime(ZinacefⓇGlaxo Smith Kline,UK)1 mg at the time of repair.If endophthalmitis is suspected,intravitreal injectionofvancomycin 1mg/0.1mland ceftazidime 2 mg/0.1 ml was given.In this study,2 cases of phthisis were associated with extensive injuries involving uveal tissue.Evisceration cases were secondary to endophthalmitis,both were presented late with suspicious endophthalmitis at the time of repair so that intravitreal antibiotics were given. Percentage of loss of globe in occupational OGI was reported at approximately 6%by Kanoff et al[16]and Bauza et al[22];and 16.28%by Vasu et al[23].Our data revealed that poor visual outcome was seen in greater number of eyes with OGI(n=10)compared to CGI(n=3)(OR=3.33,95%CI= 0.68 to 16.33).Estimated rate of monocular blindness or low vision due to work-related OGI was higher than that of CGI(0.74 vs 0.22 per 1000 hospital attendance).Studies had reported thatCGI had relativelybettervisualoutcomes compared to OGI[13,24-26].Occupational OGIs are important cause of morbidity among young healthy adults[16].In terms of public health point of view,estimated cost for primary repair of OGI is approximately 800-900 Malaysian Ringgit(280-300 USD).Furthermore,the impact will be huge when adding hospital stay and lost workdays as a result of injury. Only 59 patients(13.41%)from this study reported the EPD wear which also confirms the findings from many other studies[4,5,23,27-28].There are several reasons for not wearing EPD.Although main issue is compliance of the workers,some reported that they were not comfortable with devices as it may interfere with vision and depth perception particularly to those working at multi-storey building construction sites.Some reported that device wear increases perspiration which may leads to fogging of the devices.It was interesting that therewere 4 patients with OGI from our study reported that they wore EPD at the time of incidents.Three reported that EPD was broken when it was being struck and in the other one,EPD was dislodged.There is a concern with the quality and appropriateness of EPD for a particular given job.EPDs,when properly worn,are known to be effective in preventing impact of injuries as well as reducing the severity of injuries when impacts occur[29-31].Lombardi et al[32]identified the barriers for EPD wear as quality of EPD,vision-related issues andotherswhichincludelackofenforcement,low management priority and lack of awareness of hazards.To overcome these barriers strategies should aim to strengthen enforcement where EPD wear is required as a condition of employment.Next is to provide modern style and comfort of EPD which must be made available and accessible by workers and last but not the least work place safety training should be conducted regularly.Adams and colleagues[33]reported that EPDs designed to suit the working conditions are accepted and welcomed by quarry workers in India.They also reported that sustainedandlongerperiodofenhancededucational programme over 6mo improved the compliance with EPDs which reducestheincidenceofoculartraumaamongst workers.
To our best knowledge,the current study is the first report of work-related ocular injuries in southern Malaysia.There are limitations to our study.Being a retrospective study,we were not able to retrieve some information such as specific activity at the time of incidents due to the lack of completeness of data.Like many other work-related ocular injuries,the hospital-based data cannot be generalised to the entire population[12,19,27].However,McCallandMcCalland Horwitz[34]indicated that hospital-based studies provided valuable information which permits inter-study variability. We believe that data from current study highlight the impact of work-related ocular injury in terms of clinical as well as public health point of view.
In conclusion,it is evident from our study that work-related ocular trauma is important cause of ocular morbidity in working forces particularly young men.Malay males between 21 to 40y have higher risk.Majority of work-related ocular trauma seen in our hospital are generally of superficial injuries and potentially preventable.This study indicates the need to improve safety measures to prevent undesirable sight loss and economic burden to society as well as to establish for eye injury registry.
REFERENCES
1 Kuhn F,Mester V,Mann L,Witherspoon CD,Morris R,Maisiak R. Eye injury epidemiology and prevention of ophthalmic injuries.In Kuhn F,Pieramici DJ,ed.Ocular Trauma:Principles and Practice Thieme,2011:14-21
2 Negrel AD,Thylefors B.The global impact of eye injuries.Ophthalmic Epidemiol 1998;5(3):143-169
3 US Eye Injury Registry.Available at:http://www.useironline.org/ epidemiology.Accessed 2 Oct.2014
4 Mallika P,Tan A,Asok T,Faisal H,Aziz S,Intan G.Pattern of ocular trauma in kuching,malaysia.Malays Fam Physician 2008;3(3): 140-145
5 Voon LW,See J,Wong TY.The epidemiology of ocular trauma in Singapore:perspective from the emergency service of a large tertiary hospital.Eye(Lond)2001;15(Pt 1):75-81
6 Statistics YearbookMalaysia 2012.Availableat:http://www. statistics.gov.my/portal/download_Buku_Tahunan/files/BKKP/2012/ pdf/TAB03.pdf.Accessed 18 Sep.2014
7 Kuhn F,Morris R,Witherspoon CD.Birmingham Eye Trauma Terminology(BETT):terminology and classification of mechanical eye injuries.Ophthalmol Clin North Am 2002;15(2):139-143
8 Thylefors B.Epidemiological patterns of ocular trauma.Aust N Z J Ophthalmol 1992;20(2):95-98
9 Wong TY,Tielsch JM.Epidemiology of ocular trauma.In:Tasman W,Jaeger EA,editors.Duane's Foundations of Clinical Ophthalmology Vol.5.Philadelphia:JB Lippincott,1998:56.1-56
10 Woo JH,Sundar G.Eye injuries in Singapore-don't risk it.Do more.A prospective study.Ann Acad Med Singapore 2006;35(10):706-718
11 Krishnaiah S,Nirmalan PK,Shamanna BR,Srinivas M,Rao GN,Thomas R.Ocular trauma in a rural population of southern India:the Andhra Pradesh Eye Disease Study.Ophthalmology 2006;113(7):1159 -1164
12 Ho CK,Yen YL,Chang CH,Chiang HC,Shen YY,Chang PY. Epidemiologic study on work-related eye injuries in Kaohsiung,Taiwan. Kaohsiung J Med Sci 2007;23(9):463-468
13 Soong TK,Koh A,Subrayan V,Loo AV.Ocular trauma Injuries:a 1-year surveillance study in the University of Malaya Medical Centre,Malaysia.2008.Graefes Arch Clin Exp Ophthalmol 2011;249(12):1755-1760
14 Cao H,Li L,Zhang M.Epidemiology of patients hospitalized for ocular trauma in the Chaoshan region of China,2001-2010.PLoS One 2012;7(10):e48377.
15 Chaikitmongkol V,Leeungurasatien T,Sengupta S.Work-Related Eye Injuries:Important Occupational HealthProbleminNorthern Thailand.Asia Pac J Ophthalmol(Phila)2015;4(3):155-160
16 Kanoff JM,Turalba AV,Andreoli MT,Andreoli CM.Characteristics and outcomes of work-related open globe injuries.Am J Ophthalmol 2010;150(2):265-269
17 Jafari AK,AnvariF,AmeriA,BozorguiS,ShahverdiN. Epidemiology and sociodemographic aspects of ocular traumatic injuries in Iran.Int Ophthalmol 2010;30(6):691-696
18 Serinken M,Turkcuer I,Cetin EN,Yilmaz A,Elicabuk H,Karcioglu O.Causes and characteristics of work-related eye injuries in western Turkey.Indian J Ophthalmol 2013;61(9):497-501
19 Xiang H,Stallones L,Chen G,Smith GA.Work-related eye injuries treated in hospital emergency departments in the US.Am J Ind Med 2005;48(1):57-62
20 Alexander MM,MacLeod JD,Hall NF,Elkington AR.More than meets the eye:a study of the time lost from work by patients who incurred injuries from corneal foreign bodies.Br J Ophthalmol 1991;75(12):740-742
21 Bouchard CS,Morno K,Perkins J,McDonnell JF,Dicken R.Ocular complications of thermal injury:a 3-year retrospective.J Trauma 2001;50(1):79-82
22 Bauza AM,Emami P,Son JH,Langer P,Zarbin M,Bhagat N.Work-relatedopen-globeinjuries:demographicsandclinical characteristics.Eur J Ophthalmol 2013;23(2):242-248
23 Vasu U,Vasnaik A,Battu RR,Kurian M,George S.Occupational open globe injuries.Indian J Ophthalmol 2001;49:43-47
24 Karaman K,Gverovic-Antunica A,Rogosic V,Lakos-Krzelj V,Rozga A,Radocaj-Perko S.Epidemiology of adult eye injuries in Split-Dalmatian county.Croat Med J 2004;45(3):304-309
25 Qi Y,Zhang FY,Peng GH,Zhu Y,Wan GM,Wang WZ,Ma J,Ren SJ.Characteristics and visual outcomes of patients hospitalized for ocular trauma in central China:2006-2011.Int J Ophthalmol 2015;8(1):162-168
26 Pandita A,Merriman M.Ocular trauma epidemiology:10-year retrospective study.N Z Med J 2012;125(1348):61-69
27 Forrest KY,Cali JM,Cavill WJ.Use of protective eyewear in U.S. adults:resultsfromthe2002nationalhealthinterviewsurvey. Ophthalmic Epidemiol 2008;15(1):37-41
28 Dannenberg AL,Parver LM,Brechner RJ,Khoo L.Penetration eye injuries in the workplace.The National Eye Trauma System Registry. Arch Ophthlmol 1992;110:843-848
29 Lipscomb HJ.Effectiveness of interventions to prevent work-related eye injuries.Am J Prev Med 2000;18(4Suppl):27-33
30 Mancini G,Baldasseroni A,Laffi G,Curti S,Mattioli S,Violante FS.Prevention of work related eye injuries:long term assessment of the effectiveness of a multicomponent intervention among metal workers. Occup Environ Med 2005;62(12):830-835
31 Chen SY,Fong PC,Lin SF,Chang CH,Chan CC.A case-crossover study on transient risk factors of work-related eye injuries.Occup Environ Med 2009;66(8):517-522
32 LombardiDA,VermaSK,BrennanMJ,PerryMJ.Factors influencing worker use of personal protective eyewear.Accid Anal Prev 2009;41(4):755-762
33 Adams JS,Raju R,Solomon V,Samuel P,Dutta AK,Rose JS,Tharyan P.Increasing compliance with protective eyewear to reduce ocular injuries in stone-quarry workers in Tamil Nadu,India:a pragmatic,cluster randomised trial of a single education session versus an enhanced education package delivered over six months.Injury 2013;44(1):118-125
34 McCall BP,Horwitz IB.Assessment of occupational eye injury risk and severity:an analysis of Rhode Island workers'compensation data 1998-2002.Am J Ind Med 2006;49(1):45-53
马来西亚新山市工作相关眼外伤调查分析
Nyo Nyo Min1,Suresh Kumar Vasudevan2,Azlyn Azwabinti Jasman1,Aisyahbinti Ali3,Kay Thi Myint4
(1马来西亚,新山81110,Sultan Ismail医院,眼科;2马来西亚,新山80100,Sultanah Aminah医院,眼科;3马来西亚,新山81110,Sultan Ismail医院,临床研究中心;4马来西亚,沙捞越,诗巫96000,诗巫大学城,马来西亚世纪大学,医学院)
Kay Thi Myint.kaythimyint.eye@gmail.com
工作相关;眼外伤;保护装置;视力情况
10.3980/j.issn.1672-5123.2016.3.04
Min NN,Vasudevan SK,Azlyn AJ,Aisyah A,Myint KT.Work-related ocular injuries in Johor Bahru,Malaysia.Guoji Yanke Zazhi(Int Eye Sci)2016;16(3):416-422
2015-04-15 Accepted:2015-11-10
猜你喜欢
杂志排行

国际眼科杂志的其它文章
- Glaucomatous changes in macular ganglion cell detected byspectraldomainopticalcoherencetomography: comparison with peripapillary retinal nerve fiber layer
- 个性化人工晶状体选择方案治疗年龄相关性白内障的临床研究
- BMP-2在C57BL/6小鼠形觉剥夺性近视眼巩膜中表达的变化
- Research of serum total and high-molecular-weight adiponectin levels in patients with type 2diabetic retinopathy
- 玻璃酸钠滴眼液治疗青少年近视患者配戴硬性透气性角膜接触镜相关性干眼
- PSP对STZ诱导的糖尿病大鼠眼保护作用的临床动态观察