家族聚集性慢性乙型肝炎病毒感染者自然病程与相关因素的研究
2016-06-01郭素娟李智伟
郭素娟,李 娟,李智伟
1.宝鸡市中心医院感染科,陕西 宝鸡 721008;2.中国医科大学附属盛京医院感染科
家族聚集性慢性乙型肝炎病毒感染者自然病程与相关因素的研究
郭素娟1,李 娟1,李智伟2
1.宝鸡市中心医院感染科,陕西 宝鸡 721008;2.中国医科大学附属盛京医院感染科
目的 明确慢性乙型肝炎病毒(hepatitis B virus,HBV)感染者自然病程进展规律与感染持续时间、年龄、性别、血清ALT水平及肝组织病理学的关系。方法 收集2007年1月-2010年8月就诊于中国医科大学附属盛京医院感染科的家族聚集性慢性HBV感染患者,排除其他肝脏疾病,未应用干扰素或核苷类似物抗病毒治疗,肝脏组织病理切片采用Knodell评分系统读取,统计学方法采用描述统计学评价,卡方检验及线性回归分析,只有与单变量分析(P<0.05)密切相关的因素才进入多因素分析模式。结果 132例患者中年龄>30岁组炎症评分≥5分及纤维化评分≥3分所占频率明显高于年龄≤30岁组(P<0.05);肝功正常组肝组织炎症评分≤4分及纤维化评分≤2分所占频率高于肝功异常组(P<0.05);肝功反复异常>1年组肝组织炎症评分≥5分及纤维化评分≥3分所占频率高于肝功反复异常≤1年组(P<0.05)。血清ALT水平正常组肝组织炎症评分≤4分及纤维化评分≤2分所占频率高于ALT水平异常组(P<0.05);ALT>2×ULN组肝组织炎症评分≥5分及纤维化评分≥3分所占频率高于ALT≤2×ULN组(P<0.05)。结论 家族聚集性慢性HBV感染者肝组织炎症及纤维化程度与感染持续时间呈正相关;尤其年龄>30岁时更易出现肝脏疾病的进展;持续肝功异常时间越长肝脏炎症及纤维化改变越显著;血清ALT异常的慢性HBV感染者肝组织炎症及纤维化程度较血清ALT正常者重,而血清ALT异常者血清ALT水平越高,肝组织炎症及纤维化改变越显著。
慢性乙型肝炎病毒感染;炎症;纤维化
目前慢性乙型肝炎病毒(heptatitis B virus,HBV)感染仍然是世界公共卫生所面临的一个严峻问题[1-3]。慢性HBV感染的病程进展复杂多变,同样是慢性HBV感染者,其临床结局却往往不同,有的可表现为终身携带状态,有的却表现出慢性肝炎,甚至进展为肝硬化或肝癌[4-6]。慢性HBV感染的病程进展与多种因素有关,目前关于慢性HBV感染病程进展的研究很多,但多数是与某种单一因素之间的关系,而在临床上影响病程进展的因素往往很多。
1 资料与方法
1.1 一般资料 选取2007年1月-2010年8月就诊于中国医科大学盛京医院感染科家族聚集性的慢性HBV感染者132例。男83例(62.9%),女49例(37.1%),年龄8~62岁,平均年龄(33.81±11.61)岁。入选标准:(1)有乙肝家族聚集史,即:有1位以上家庭成员为慢性HBV感染者;(2)HBsAg阳性>6个月,肝功能异常或正常;(3)已行肝穿组织活检病理检查;(4)除外合并有甲丙戊型肝炎病毒重叠感染和其他肝脏疾病,如自身免疫性肝病、肝豆状核变性、酒精或药物性肝损伤等。
1.2 数据收集及整理 回顾性分析患者资料包括年龄、性别、饮酒史、吸烟史。临床数据包括ALT、反复肝功能异常时间、HBV DNA载量、HBeAg、HBsAg、HBeAb、脾脏厚度及肝组织炎症及纤维化评分,收集的ALT为已知最高值,其他数据为最新的实验室检测数据。相关检测方法:肝功能采用雅培全自动生化分析仪ARCIECT Ci8000,HBV血清学指标应用雅培ARCHITECT Ci8000,化学发光法进行定量检测,部分应用上海科华生物公司试剂盒,通过酶联免疫吸附法(ELISA)监测,监测项目包括:乙肝表面抗原、乙肝e抗原、乙肝e抗体,HBV DNA定量采用BIOER Line-gene Ⅱ荧光定量PCR检测系统,ABI 7300 Real Time PCR系统,应用深圳凯杰生物工程公司的(HBV)核酸扩增(PCR)荧光定量检测试剂盒。ALT水平的上限值定义为40 U/L。脾脏厚度由空腹超声检查测量所得;肝脏组织病理是在超声引导下用14 G肝穿针穿刺取2个位点的肝组织,由同一名资深病理专家统一用1995年版的Knodell评分系统进行肝组织炎症及纤维化评分[7]。肝脏疾病状态由肝穿组织炎症及纤维化程度来评价。
1.3 统计学处理 采用SPSS 17.0软件进行分析。数据的误差及常态用描述统计学评价,χ2检验用于决定变量的比较,多因素分析用线性回归分析,与单变量分析密切相关的因素进入多因素分析。P<0.05为差异有统计学意义。
2 结果
2.1 研究资料描述性评价 132例患者中,19.7%(26/132)有长期吸烟史,25.0%(33/132)有长期饮酒史。68.2%(90/132)出现ALT升高。入选病例中肝组织活检炎症评分≤4分者98例(74.2%),5~10分者29例(22.0%),>10分者5例(3.8%);肝组织活检病理纤维化程度评分≤2者94例(71.2%),3~4分者21例(15.9%),≥5分者17例(12.9%)。所有入选病例HBV DNA载量、血清HBeAg状态、肝功能情况、ALT水平等指标的分布情况如表1所示。

表1 研究资料的描述性评价[例数(%)]Tab 1 Descriptive evaluation of research data [n(%)]
2.2 单因素分析
2.2.1 宿主因素:将132例患者按年龄分为>30岁组及≤30岁组,>30岁组炎症评分≥5分及纤维化评分≥3分所占频率分别为33.3%和38.4%;年龄≤30岁组炎症评分≥5分及纤维化评分≥3分所占频率分别为14.9%和14.8%。慢性HBV感染者的性别、饮酒史及吸烟史对肝组织炎症及纤维化的影响相比,差异无统计学意义(P>0.05,见表2~3)。
2.2.2 生化指标:肝功能正常组肝组织炎症评分≤4分及纤维化评分≤2分所占频率明显高于肝功异常组;肝功反复异常>1年组肝组织炎症评分≥5分及纤维化评分≥3分所占频率高于肝功反复异常≤1年组;血清ALT水平正常组肝组织炎症评分≤4分及纤维化评分≤2分所占频率高于血清ALT水平异常组;ALT>2×ULN组肝组织炎症评分≥5分及纤维化评分≥3分所占频率高于ALT≤2×ULN组(见表2、4)。
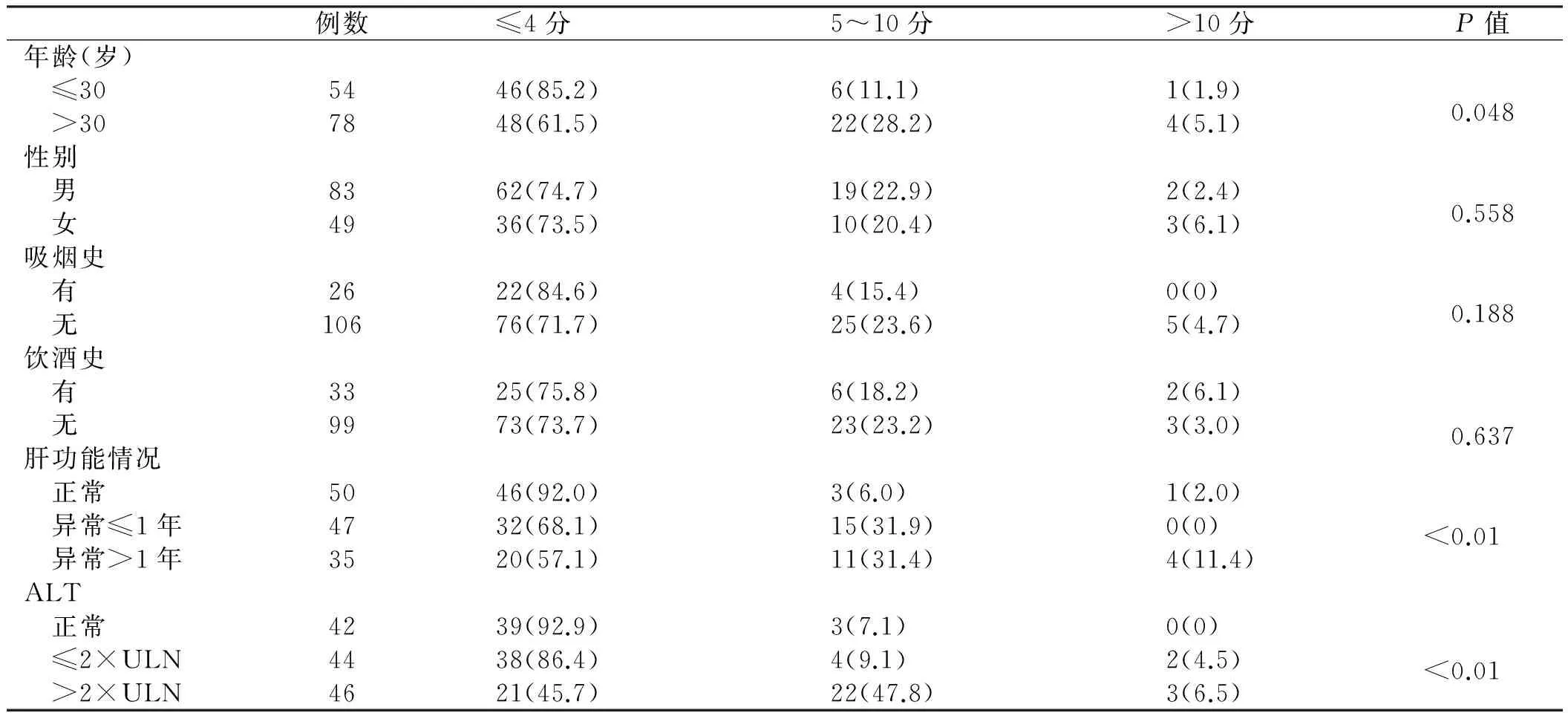
表2 肝组织炎症与各因素之间单变量分析[例数(%)]Tab 2 Univariate analysis between liver inflammation and different factors [n(%)]
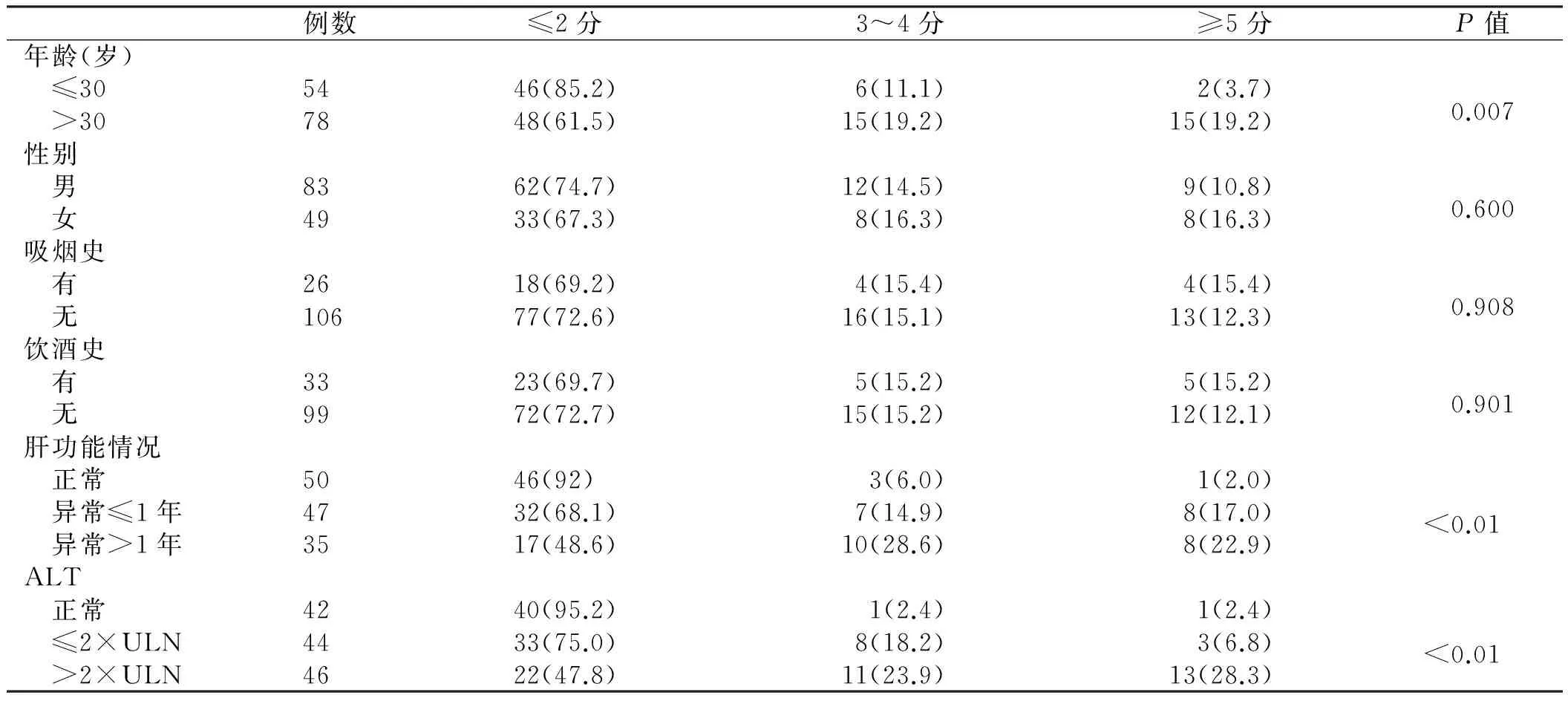
表3 肝组织纤维化程度与各因素之间单变量分析[例数(%)]Tab 3 Univariate analysis between liver fibrosis and different factors[n(%)]
2.3 多因素分析 将以上单因素分析中差异有统计学意义因素进行多因素分析。ALT水平与肝组织炎症及纤维化程度呈显著独立正相关性。而肝功能情况及感染者的年龄对肝组织炎症及纤维化的影响则无独立相关性(P>0.05,见表4~5)。
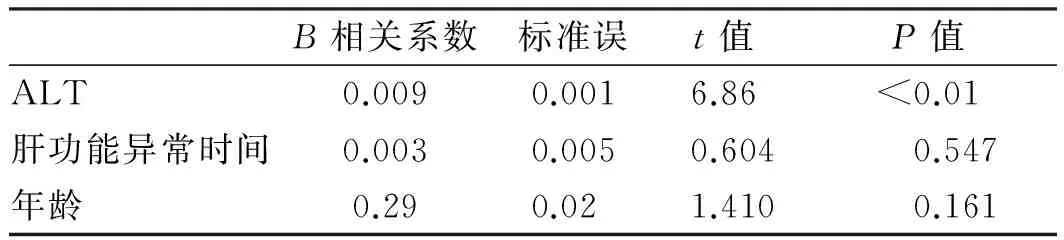
表4 与肝组织炎症程度相关因素的多因素分析Tab 4 Multivariate analysis of factors related to the degree of liver inflammation

表5 与肝组织纤维化程度相关因素的多因素分析Tab 5 Multivariate analysis of factors related to the degree of liver fibrosis
3 讨论
肝组织炎症及纤维化改变与机体的免疫状态及病毒自身的状态密切相关,并可引起ALT、病毒状态等一系列的改变[8-9]。本研究单因素分析结果表明,肝组织炎症及纤维化程度与感染持续时间呈正相关:此132例者中有78例年龄>30岁,其中有33.3%肝组织炎症评分>5分,38.4%肝组织纤维化评分>3分,相对于年龄≤30岁患者频率显著增加。ALT水平是反映肝细胞损伤的灵敏指标,有研究表明ALT水平越高,其发生肝硬化或肝细胞癌的可能性越高[10]。本研究中,ALT正常组在肝组织炎症评分≥5分及纤维化评分≥3分所占频率依次递减,这也证实了以上结论。这一规律也适用于持续肝功能异常时间与肝组织炎症及纤维化改变之间的关系,即肝功持续异常时间越长,肝脏疾病进展的可能性越高[11-12]。另外,在本研究的单一因素分析中,肝脏炎症及纤维化程度与患者吸烟史、饮酒史及性别均无明显相关性。
进一步的多因素分析结果表明,ALT水平与肝组织炎症及纤维化程度独立正相关性,而其他因素如年龄、肝功情况对肝组织炎症及纤维化程度的影响则是与其他因素共同作用的结果。
[1]National Center for HIV/AIDs,Viral Hepatitis,STD & TB Prevention. Viral hepatitis surveillance [C].United States,2010.
[2]Mitchell AE,Colvin HM,Palmer Beasley R. Institute of medicine recommendations for the prevention and control of hepatitis B and C [J]. Hepatology,2010,51(3): 729-733.
[3]Chen CJ,Yang HI,Su J,et al. Risk of hepatocellular carcinoma across a biological gradient of serum hepatitis B virus DNA level [J]. JAMA,2006,295(1): 65-73.
[4]Yuen MF,Tanaka Y,Mizokami M,et al. Role of hepatitis B virus genotypes Ba and C,core promoter and precore mutations on hepatocellular carcinoma: a case control study [J]. Carcinogenesis,2004,25(9): 153-159.
[5]The Chinese National Workshop on Fatty Liver and Alcoholic Liver Disease for the Chinese Liver Disease Association. Guidelines for management of alcoholic liver disease: an updated and revised edition [J]. Chin J Hepatol,2010,18(3): 167-170. 中华医学会肝病学分会脂肪肝和酒精性肝病学组. 酒精性肝病诊疗指南(2010年修订版)[J]. 中华肝脏病杂志,2010,18(3): 167-170.
[6]Manno M,Cammà C,Schepis F,et al. Natural history of chronic HBV carriers in northern Italy: morbidity and mortality after 30 years [J]. Gastroenterology,2004,127(3): 756-763.
[7]Ishak K,Baptista A,Bianchi L,et al. Histological grading and staging of chronic hepatitis [J]. J Hepatol,1995,22(6): 696-699.
[8]Anna SF,Lok Brian J. McMahon. Chronic Hepatitis B: Update 2009. AASLD practice guidelines [J]. Hepatology,2009,9(50): 1-36.
[9]European Association for the Study of the Liver. EASL clinical practice guidelines: management of chronic hepatitis B [J]. J Hepatol,2009,50(2): 227-242.
[10]Yuen MF,Yuan HJ,Wong DK,et al. Prognostic determinants for chronic hepatitis B in Asians: therapeutic implications [J]. Gut,2005,54(11): 1610-1614.
[11]Thompson AJ,Nguyen T,Iser D,et al. Serum hepatitis B surface antigen and hepatitis B e antigen titers: disease phase influences correlation with viral load and intrahepatic hepatitis B virus markers [J]. Hepatology,2010,51(6): 1933-1944.
[12]Kim HC,Nam CM,Jee SH,et al. Normal serum aminotransferase concentration and risk of mortality from liver diseases: prospective cohort study [J]. BMJ,2004,328(7446): 983.
(责任编辑:王全楚)
Study on natural progressive course and relative factors of chronic hepatitis B virus infection with family cluster
GUO Sujuan1,LI Juan1,LI Zhiwei2
1.Department of Infectious Diseases,Baoji Municipal Center Hospital,Baoji 721008; 2.Department of Infectious Diseases,Shengjing Hospital of China Medical University,China
Objective To investigate the relationship between natural progressive course of chronic hepatitis B virus (HBV) infection and the factors such as the time length of infection,age,sex,ALT level and liver biopsy.Methods Chronic HBV infection with family cluster who were treated in Shengjing Hospital of China Medical University from Jan. 2007 to Aug. 2010. without other liver diseases,without treatment of interferon or analogues antiretroviral were collected. Liver tissue pathological slices were read with Knodell score system; statistical methods were descriptive statistics,Chi-square test and linear regression analysis,only univariate analysis (P<0.05) closely related factors could enter multiple factors analysis model.Results Among the 132 patients,the frequencies of group in the inflammation score≥5 and fibrosis score ≥3 when age>30 years old,which was higher than the group of age≤30 years old. The frequencies in inflammation score≤4 and fibrosis score≤2 in liver function normal group,which was higher than the liver function abnormal group. The liver function kept on abnormal>1 year had higher frequencies than the liver function kept on abnormal≤1 year,in the inflammation score≥5 and fibrosis score≥3 group. The frequencies in inflammation score≤4 and fibrosis score≤2 in serum ALT normal group,which was higher than that in serum ALT abnormal group. And the frequencies in the group inflammation score≥5 and fibrosis score≥3 when serum ALT>2×ULN,which was higher than the group of ALT≤2×ULN.Conclusion The time length of infection have positive correlation to the severity of liver inflammation and fibrosis of chronic HBV infection with family cluster. It shows that progress of liver disease appear easily when age>30 years old. The longer of liver function abnormal,the liver inflammation and fibrosis are more serious.
Chronic hepatitis B virus infection; Inflammation; Fibrosis
郭素娟,硕士,主治医师,研究方向:感染性疾病。E-mail:22255467@qq.com
李智伟,教授,主任医师,研究方向:感染性疾病。E-mail:lizw@sjhospital.org
10.3969/j.issn.1006-5709.2016.04.015
R512.6+2
A
1006-5709(2016)04-0419-04
2015-05-12
