Prevalence of corneal astigmatism before cataract surgery in northeast China
2016-05-17ZuoFengGuoQingChengShiYanWenZhouHaiJuanWuJingJingLi
Zuo-Feng Guo, Qing-Cheng Shi, Yan-Wen Zhou, Hai-Juan Wu, Jing-Jing Li
Aier Ophthalmolgy of Shenyang, Shenyang 110003, Liaoning Province, China
Correspondence to:Yan-Wen Zhou. Room 11, 11 Wei Road, Shenyang 110003, Liaoning Province,China
Received: 2015-03-30 Accepted: 2016-01-26
中国东北地区年龄相关性白内障患者角膜散光的分布情况调查
郭作锋, 史庆成, 周衍文, 吴海娟, 李晶晶
(作者单位:110003中国辽宁省沈阳市,沈阳爱尔视光医院)
Prevalence of corneal astigmatism before cataract surgery in northeast China
Zuo-Feng Guo, Qing-Cheng Shi, Yan-Wen Zhou, Hai-Juan Wu, Jing-Jing Li
Aier Ophthalmolgy of Shenyang, Shenyang 110003, Liaoning Province, China
Correspondence to:Yan-Wen Zhou. Room 11, 11 Wei Road, Shenyang 110003, Liaoning Province,China
Received: 2015-03-30Accepted: 2016-01-26
中国东北地区年龄相关性白内障患者角膜散光的分布情况调查
郭作锋, 史庆成, 周衍文, 吴海娟, 李晶晶
(作者单位:110003中国辽宁省沈阳市,沈阳爱尔视光医院)
Abstract
•AIM:To analyze the prevalence and presentation patterns of corneal astigmatism in cataract surgery candidates of Shenyang in northeast China.
•METHODS:A retrospective survey was used to study the corneal astigmatism which were measured by intraocular lens(IOL) Master optical biometer before cataract surgery between Jan. 1st, 2014 and Dec. 31st, 2014. Descriptive statistics of corneal astigmatism data were analyzed.
•RESULTS:The keratometric data from 4 543 eyes from 3821 patients with a mean age of 66.36±10.38y(SD). In 10.50% of eyes, corneal astigmatism was between 0.5 diopters(D) or less; in 30.05% of eyes, it was 0.5-1.0 D;in 23.60%, it was 1.0-1.5 D;in 13.19%, it was 1.5-2.0 D;in 7.68%, it was 2.0-2.5 D;in 6.41%, it was 2.5-3.0 D;in 8.58%, it was 3.0 D or higher. With-the-rule astigmatism was found in 27.69% of eyes, while against-the-rule was found in 53.84% of eyes.
•CONCLUSION:About 59.46% of eyes in this study had preoperative corneal astigmatism equal to or above 1.0 D. Findings indicated more surgical techniques or toric intraocular lenses to meet the potential demand of the cataract surgery candidates.
KEYWORDS:•cataract;corneal astigmatism;toric intraocular lens
Citation:Guo ZF, Shi QC, Zhou YW, Wu HJ, Li JJ. Prevalence of corneal astigmatism before cataract surgery in northeast China.GuojiYankeZazhi(IntEyeSci) 2016;16(5):798-800
INTRODUCTION
Phacoemulsification is one of the most successfully cataract surgeries worldwide. With the advanced in intraocular lens(IOL) calculations, the incidence of spherical refractive errors had significantly reduced. The residual astigmatism after surgery is a concern for both ophthalmologist and patients with the decreased visual function[1-3].
The prevalence of corneal astigmatism in the cataract surgery candidates have been reported in China[4]and other countries[5], but not been reported in the northeast China. The purpose of the presented study reviewed all of the cataract patients in one year in the Shenyang Aier Eye Hospital to investigate the prevalence of corneal astigmatism in the northeast China.
SUBJECTS AND METHODS
This retrospective study comprised 4543 eyes from 3821 patients. The study was conducted between Jan. 1st, 2014 and Dec. 31st, 2014 in Shenyang Aier Eye Hospital. Inclusion criteria included presence of cataract and age between 37 and 91y. Exclusion criteria included corneal disease, precious corneal or intraocular surgery, and history of ocular inflammation. All eyes were examined, including a complete ophthalmological examination, slitlamp examination, noncontact tonometry, IOL Master, and ophthalmoscopy through dilated pupils.To find the type of the corneal astigmatism the sample was divided into 7 age groups:less than 40y,40 to 49y, 50 to 59y, 60 to 69y, 70 to 79y, and 80 to 89y, 90y or older.
The analysis of corneal astigmatism was performed using the IOL Master optical biometer. This system performs an automatic measurement of the central astigmatism and the steep K’s axis.
The research followed the tenets of the Declaration of Helsinki after approval for the study protocol from The Scientific Research Committee of The Aier Eye Hospital. Informed consent was obtained from all patients enrolled in the study after the nature and possible consequences of the procedures had been explained.
RESULTS
This study was composed of 4543 eyes from 3821 patients. The patients’ demographics are shown in Table 1.
Table 2 and Figure 1 list the prevalence of corneal astigmatism stratified by amount of astigmatism. The most corneal astigmatism was in 0.5 D to 1.0D(1 365 eyes);and the corneal astigmatism more than 3.5 D was merely 13 eyes. Figure 1 is a histogram with frequency distribution of corneal astigmatism values for the entire sample.
Table 3 shows the with-the-rule(WTR) corneal astigmatism was found in 1258 eyes(27.69%), against-the-rule(ATR) corneal astigmatism was found in 2446 eyes(53.84%), and the oblique corneal astigmatism was found in 839 eyes (18.47%). Figure 2 showed the ATR astigmatism proportion increased with age and the WTR astigmatism proportion decreased with age.
DISCUSSION
Accurate measurement of corneal power is essential for refractive surgery, orthokeratology, contact lens fitting, and IOL power. The reliability of the keratometry depends on the repeatability, reproducibility and on the validity of the keratometry measurements. The manual keratometry, corneal topographers, IOL Master, and Pentacam are the main common devices for the measurement of the corneal power. The difference between these devices is depend on the measuring principles[6]. Manual keratometer uses two keratometry mires along the main meridians of the cornea. The corneal power is determined using the reflection from these illuminated mires from the central 3.4 mm of the cornea. The device uses a refraction index of 1.3375[7]. In topography, to estimate the central 3 mm curvature, 7-8 Placido rings are used. In the IOL Master, six light spots are projected onto the cornea in a hexagonal pattern, and measurement is performed in a 2.3 mm radius[7]. The Pentacam is a Scheimpflug camera used for corneal imaging[7]. Equivalent keratometry values from the Pentacam are generated using measurements of the anterior and posterior corneal values in the central 3 mm. It has been well demonstrated that the IOL Master is highly precise, accurate, and reproducible[8]. Kimetal[9]have demonstrated that the IOL Master has fairly good results in
Table 1Patients’ demographics

CharacteristicValueNumberofeyes/patients4543/3821Meanage(a)±SD66.36±10.38Rangeofage(a)37-91M/F1213/4494Meancornealastigmatism(D)±SD0-6.75
Table 2Prevalence of corneal astigmatism stratified by amount of astigmatism

Cornealastigmatism(D)Prevalence(%)Eyesnumber≤0.510.50477>0.5and<1.030.051365>1.0and≤1.523.601072>1.5and≤2.013.19599>2.0and≤2.57.68349>2.5and≤3.06.41291>3.08.58390
Table 3The distribution of WTR, ATR, and oblique corneal astigmatism

Agegroup(a)WTRATRObliqueEyes<40431166040-49132433420950-5926828512968260-69385741251137770-79343986319164880-898235293527≥90528740
WTR:With-the-rule;ATR:Against-the-rule.

Figure 1Histogram of the corneal astigmatism distribution in the entire sample(4 543 eyes).
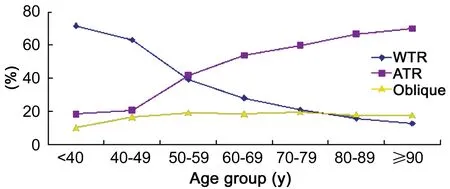
Figure 2Percentages of the type of the corneal astigmatism in the 7 groups.
refractive prediction for cataract surgery. The IOL Master was often used to evaluate the preoperative keratometry, which may have indirectly validate that the IOL Master is both reliable and accurate.
Astigmatism is one of the main types of correct refractive error, and it was due to the different refractive power in different meridians, and it formed two main focal lines and minimum diffuse form spot.Significant corneal astigmatism was one of the major obstacle to obtain satisfactory postoperative visual outcome. Corneal astigmatism can be managed surgically using limbal relaxing incisions(LRI)[10], opposite clear corneal incisions[11], femtosecond laser-assisted astigmatic keratotomy[12-13]. But a 2.2 mm clear corneal incision may result in a surgically induced corneal astigmatism(SIA) about 0.5 D[14-15]. In our study only 10.50% of eyes had a corneal astigmatism of 0.5 D or less. However, the results of LRI and the femtosecond laser-assisted astigmatic keratotomy were unpredictable and were associated with complications[16]. The limitations, advantages, and disadvantages have been fully discussed. The use of toric IOLs to correct corneal astigmatism is a growing surgical option, with encouraging results[17]. The present study attempted to determine the prevalence of different amounts of corneal astigmatism, as such dates of the northeast of China were not available in the literature surveyed by the authors. As previously said, the descriptive analysis provided is valuable information for cataract surgeons and IOL manufacturers.
This study investigated the prevalence of corneal astigmatism using IOL Master, which could afford the measurement of corneal status reliably[18-20]. The results showed that the mean age and the distribution were similar to previously reported data. Most cataract surgery candidates in the present cohort were women, following a trend in previous studies[4]. The mean corneal astigmatism was 1.33±1.03 D, which is slightly higher than that in other published studies[5]. Our study demonstrated that about 59.46% of cataract candidates had corneal astigmatism of 1.0 D or greater. Ten point forty-nine percent(10.50%) of candidates had corneal astigmatism of 0.5 D or less, and 8.58% of candidates had corneal astigmatism of more than 3.0 D. Our results were different from other groups[4]. Results revealed that the corneal astigmatism axis was mainly ATR(53.84%), and the prevalence increased with age. And the WTR was 27.69%, by contrast the percentage of WTR astigmatism decreased with age. These findings are generally consistent with those of previous studies[4].
There is a wide area and multitude population in our country, more and more people accepted the cataract surgery, so the multi-center study of the corneal astigmatism is significant job. We just had a rough and preliminary research, then it requires further study for the clinical work.
REFERENCES
2 Lockwood JC, Randleman JB. Toric intraocular lens rotation to optimize refractive outcome despite appropriate intraoperative positioning.JCataractRefractSurg2015;41(4):878-883
3 Koch DD, Ali SF, Weikert MP, Shirayama M, Jenkins R, Wang L. Contribution of posterior corneal astigmatism to total corneal astigmatism.JCataractRefractSurg2012;38(12):2080-2087
4 Chen W, Zuo C, Chen C, Su J, Luo L, Congdon N, Liu Y. Prevalence of corneal astigmatism before cataract surgery in Chinese patients.JCataractRefractSurg2013;39(2):188-192
5 Ercegovic A, Brajkovic J, Surac IK, Haluzan MB. Prevalence, distribution and types of corneal astigmatism in cataract surgery patients in Sibenik County.ActaClinCroat2012;51(2):275-278
6 Módis L Jr, Szalai E, Kolozsvári B, Németh G, Vajas A, Berta A. Keratometry evaluations with the Pentacam high resolution in comparison with the automated keratometry and conventional corneal topography.Cornea2012;31:36-41
7 Visser N, Berendschot TT, Verbakel F, de Brabander J, Nuijts RM. Comparability and repeatability of corneal astigmatism measurements using different measurement technologies.JCataractRefractSurg2012;38:1764-1770
8 Choi JH, Roh GH. The reproducibility and accuracy of biometry parameter measurement from IOL Master(R).JKoreanOphthalmolSoc2004;45:1665-1673
9 Kim SM, Choi J, Choi S. Refractive predictability of partial coherence interferometry and factors that can affect it.KoreanJOphthalmol2009;23(1):6-12
10 Ouchi M, Kinoshita S. AcrySof IQ toric IOL implantation combined with limbal relaxing incision during cataract surgery for eyes with astigmatism >2.50 D.JRefractSurg2011;27(9):643-647
11 Nemeth G, Kolozsvari B, Berta A, Laszlo M. Paired opposite clear corneal incision:time-related changes of its effect and factors on which those changes depend.EurJOphthalmol2014;24(5):676-681
12 Rückl T, Dexl AK, Bachernegg A, Reischl V, Riha W, Ruckhofer J, Binder PS, Grabner G. Femtosecond laser-assisted intrastromal arcuate keratotomy to reduce corneal astigmatism.JCataractRefractSurg2013;39(4):528-538
13 Dick HB, Schultz T. Femtosecond laser-assisted cataract surgery.Ophthalmologe2014;111(7):614-623
14 Chang SW, Su TY, Chen YL. Influence of ocular features and incision width on surgically induced astigmatism after cataract surgery.JRefractSurg2015;31(2):82-88
15 Denoyer A, Ricaud X, Van Went C, Labbé A, Baudouin C. Influence of corneal biomechanical properties on surgically induced astigmatism in cataract surgery.JCataractRefractSurg2013;39(8):1204-1210
16 Kumar NL, Kaiserman I, Shehadeh-Mashor R, Sansanayudh W, Ritenour R, Rootman DS. IntraLase-enabled astigmatic keratotomy for post-keratoplasty astigmatism:on-axis vector analysis.Ophthalmology2010;117(6):1228-1235.e1
17 Toto L, Vecchiarino L, D’Ugo E, Cardone D, Mastropasqua A, Mastropasqua R, Di Nicola M. Astigmatism correction with toric IOL:analysis of visual performance, position, and wavefront error.JRefractSurg2013;29(7):476-483
18 Yong Park C, Do JR, Chuck RS. Predicting postoperative astigmatism using Scheimpflug keratometry(Pentacam) and automated keratometry(IOLMaster).CurrEyeRes2012;37(12):1091-1098
19 Nemeth G, Szalai E, Berta A, Modis L Jr. Astigmatism prevalence and biometric analysis in normal population.EurJOphthalmol2013;23(6):779-783
20 De Bernardo M, Zeppa L, Cennamo M, Iaccarino S, Zeppa L, Rosa N. Prevalence of corneal astigmatism before cataract surgery in Caucasian patients.EurJOphthalmol2014;24(4):494-500
摘要
关键词:白内障,角膜散光,Toric人工晶体
DOI:10.3980/j.issn.1672-5123.2016.5.02
通讯作者:周衍文,毕业于上海第二军医大学,本科,主任医师,研究方向:白内障. zhouyanwen@vip.163.com
作者简介:郭作锋,毕业于辽宁医学院,硕士研究生,主治医师,研究方向:白内障。
目的:观察和分析中国东北沈阳地区的白内障患者角膜散光的分布情况。
方法:利用回顾性研究方法观察2014年1月1日至2014年12月31日行白内障手术患者的术前角膜散光分布规律(利用IOL Master测量)。通过描述性方法分析角膜散光数据。
结果:研究包含3 821名患者(平均年龄为66.36 ±10.38岁)4 543眼。角膜散光<0.5D占10.50%,0.5D~1.0D占30.05%,1.0D~1.5D占23.60%,1.5D~2.0D占13.19%,2.0~2.5D占7.68%,2.5~3.0D占6.41%,>3.0D占8.58%。其中27.69%为顺规散光,53.84%为逆规散光。
结论:约59.46%患者的角膜散光≥1.0D。观察结果提示在白内障手术中,需要一些具有矫正散光功能的人工晶状体或特殊的手术技巧来矫正角膜散光,以保证患者术后视觉质量。
引用:郭作锋, 史庆成, 周衍文, 吴海娟, 李晶晶. 中国东北地区年龄相关性白内障患者角膜散光的分布情况调查. 国际眼科杂志2016;16(5):798-800
·Original article·