初诊伴有脊柱转移的前列腺癌生存相关因素分析
2015-12-21单露玲韩秀鑫张超任志午梁守磊王国文
单露玲 韩秀鑫 张超 任志午 梁守磊 王国文
·临床研究与应用·
初诊伴有脊柱转移的前列腺癌生存相关因素分析
单露玲 韩秀鑫 张超 任志午 梁守磊 王国文
目的:探讨初诊时伴有脊柱转移的前列腺癌患者与生存相关的因素。方法:收集2005年1月至2010年12月天津医科大学肿瘤医院接受内分泌治疗的前列腺癌脊柱转移患者49例,针对患者的碱性磷酸酶(ALP)、治疗前有无骨相关事件(SREs)、Gleason评分、治疗后PSA最低值、激素敏感持续时间、有无化疗行单因素分析,并对存在统计学意义者进行多因素分析。结果:平均随访时间64.1个月,死亡41例,中位生存时间为27个月,1、3、5年生存率分别是81.6%、40.8%、20.4%。单因素分析结果显示,有无联合化疗、ALP水平、治疗前是否出现SRE、Gleason评分、治疗后PSA最低值及激素敏感持续时间与总生存率(OS)有关(P<0.05)。Cox回归模型多因素分析显示,激素敏感持续时间≥19个月及联合化疗是较长生存时间的独立预后因素(P<0.05)。结论:激素敏感持续时间及进展为去势抵抗性前列腺癌(castration resistant prostate cancer,CRPC)后是否联合化疗是前列腺癌脊柱转移患者的预后独立因素。
前列腺癌 脊柱转移 化疗 内分泌治疗 预后因素
世界范围内,前列腺癌是男性中第二大常见恶性肿瘤[1],且发病率呈上升趋势。在西方国家,早期诊断未有远处转移的前列腺癌患者,其5年生存率可达100%,若诊断时即出现远处转移,5年生存率仅为33%[2]。在我国很多前列腺癌患者在就诊时即为晚期,并伴有脊柱转移,对这一患者群体缺乏统一规范的治疗策略。
对于转移性去势抵抗性前列腺癌(metastatic castration resistant prostate cancer,mCRPC)患者生存相关的预后因素的分析显示血清ALP水平、激素敏感持续时间、治疗前PSA值、首次骨转移出现时间、血红蛋白等是mCRPC的独立预后因素[3-4],但对于初诊即伴有脊柱转移的前列腺癌患者的预后因素分析报道较少。本研究回顾性分析初诊时伴有脊柱转移的前列腺癌患者的临床资料,探讨影响其生存时间的因素。
1 材料与方法
1.1 临床资料
收集2005年1月至2010年12月天津医科大学肿瘤医院初诊伴有脊柱转移的前列腺癌患者49例,年龄54~81岁,平均为(70.27±7.13)岁,其中年龄<60岁患者为5例,60~70岁患者为17例,年龄>70岁患者为27例。13例在进展为CRPC后给予多西他赛化疗,22例以剧烈疼痛就诊,20例行脊柱转移病灶放疗,2例行椎体穿刺活检+椎体成形术,本研究中未纳入病理性骨折或截瘫的患者。
确诊时ALP为53~1 141 U/L,中位数为179 U/L,治疗前即出现骨相关事件(SRE)的为17例,Gleason评分5~6分为14例,7分为8例,8~10分为27例,治疗后PSA最低值为0.03~5 328 μg/L,激素敏感持续时间为0~49个月,中位数为19个月。
1.2 方法
1.2.1 纳入标准 1)前列腺或转移病灶病理结果确诊;2)影像学或组织活检确诊脊柱转移;3)经治疗后转变为CRPC。排除标准:1)伴有骨外远处转移;2)伴有全身其他影响生存的其他疾病,如心脏病、其他癌症等。
1.2.2 治疗 26例行双侧睾丸切除术,23例给予亮丙瑞林或戈舍瑞林,同时均辅助应用抗雄激素药物,其中13例在病情进展后给予多西他赛化疗。
1.3 统计学方法
应用SPSS 19.0统计软件对随访结果进行分析。采用Kaplan-Meier法行生存相关单因素分析,并行Log-rank检验,采用Cox模型行多因素分析。P<0.05为差异有统计学意义。
2 结果
2.1 生存分析
平均随访时间64.1个月,至随访截止。死亡41例,中位生存时间为27个月,1、3、5年生存率分别是81.6%、40.8%、20.4%。
2.2 单因素生存分析
合并化疗、确诊时ALP值<179 U/L、治疗前未出现SRE、Gleason评分<7分、PSA最低值<10 μg/L以及激素敏感持续时间≥19个月与较长OS有关(P<0.05,表1)。
2.3 多因素生存分析
Cox回归模型多因素生存分析结果显示,疾病进展后合并化疗及激素敏感持续时间≥19个月是较长生存时间的独立预后因素(P<0.05,表1,图1,2)。

表1 变量的生存相关分析Table 1 Survival-related analysis of the variables

图1 不同治疗方式的生存曲线Table 1 Survival curves of various treatment methods
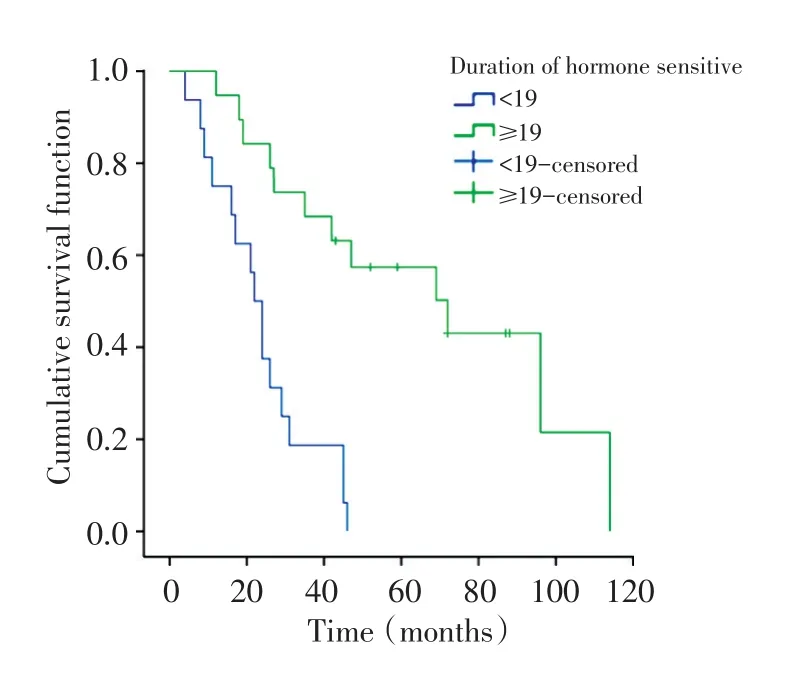
图2 PSA敏感时间相关生存曲线Table 2 PSA sensitization time-related survival curves
3 讨论
前列腺是骨转移瘤的第二大原发病灶,是男性骨转移瘤最常见的原发病,其中脊柱是骨转移的高发部位。与脊柱外骨转移相比,前列腺癌脊柱转移往往更早出现症状,且能够造成剧烈疼痛、麻木、瘫痪等不良后果,同时由于前列腺癌对内分泌治疗敏感,生存期相对较长,为改善患者生活质量,一部分患者需要外科干预,而脊柱外骨转移则多以前列腺癌综合治疗为主。在我国,很大一部分前列腺癌患者以脊柱转移症状起病,目前缺乏对这些患者的标准治疗,研究影响这一患者群的预后因素可以有效指导临床治疗。
脊柱转移瘤包括成骨型、溶骨型与混合型。溶骨型X线平片表现为椎体骨质破坏、变扁,但椎间隙多保持正常、椎弓根多受侵蚀;CT表现为低密度缺损区,常伴有软组织肿块。成骨型X线片表现为斑片状或结节样高密度影、椎体不压缩变扁,CT表现为松质骨内的高密度灶,一般无软组织肿块。MRI表现以T1加权像最为明显,表现为与正常骨髓脂肪高信号高度对比的低信号。混合型兼有成骨型与溶骨型的表现。
前列腺癌脊柱转移以成骨型病变为主,临床上晚期前列腺癌脊柱转移以混合型病变为主。而其他来源的脊柱转移,如肺癌、肾癌、肝癌等多以溶骨型病变为主,且相对于前列腺癌脊柱转移,局灶病变进展较快。内分泌治疗是激素依赖型前列腺癌骨转移患者主要的治疗手段,内分泌治疗引起的骨丢失会促进转移性前列腺癌细胞在骨内生长[5],这会加速引起SRE的发生,增加死亡风险并降低生活质量,因此需要对骨转移病灶行针对性治疗。作为重要的骨保护剂,唑来膦酸可降低SREs的发生率[6-7],地诺单抗被证实可延缓非转移性去势抵抗性前列腺癌(non-metastatic castration resistant prostate cancer, nm-CRPC)患者发生骨转移[8]。对于出现顽固性疼痛、骨折及脊髓压迫症状的患者可选择局部放疗或手术,放疗可缓解骨转移引起的骨痛,手术可缓解疼痛、预防/固定骨折、提高生存质量等[9]。20世纪80年代以前手术治疗脊柱转移瘤尚未得到认可,放疗是脊柱转移的标准治疗。Nguyen等[10]研究显示传统的放疗可以在治疗3个月后有效缓解疼痛,并对患者的心理变化有积极影响。最新研究显示单纯立体定向放疗或联合开放手术可有效控制局灶病变,改善神经功能[11]。本研究中20例患者进行了转移病灶放疗,2例患者行姑息性手术,但均与OS无关。临床上部分伴有截瘫的前列腺癌脊柱转移患者经手术治疗后可恢复或改善神经功能,同时可明显缓解疼痛。
自2004年以来多西他赛联合泼尼松已成为转移性CRPC的标准一线治疗方案[12],但临床中转移性前列腺癌的治疗仍不规范。本研究显示初诊伴有脊柱转移的前列腺癌患者经综合治疗后中位生存期为27个月,内分泌治疗后约19个月进展为去势抵抗性前列腺癌,进展为mCRPC后给予多西他赛化疗可有效延长患者生存期,对于多西他赛治疗失败的mCRPC患者,多项临床试验进行相关研究证实卡巴他赛可延长多西他赛耐药患者的总生存期(OS)及无进展生存期(PFS),阿比特龙可延长OS及增加PSA反应率[13-14]。此外,转移性前列腺癌经一线内分泌治疗进展后可选择二线内分泌治疗,包括更换/暂停抗雄激素药物,使用雌激素等。Narimoto等[15]的研究指出CRPC患者治疗时,将抗雄激素药物由比卡鲁胺更换为氟他胺后,PSA反应率达87.5%。本研究中单纯内分泌治疗相对于内分泌治疗联合化疗死亡风险增加了3.9倍。
骨是前列腺癌最常见转移部位,90%以上的CRPC患者会出现骨转移[6,16],一部分患者在内分泌治疗之前即出现骨转移。前列腺癌骨转移引起成骨与破骨活性紊乱,造成血清ALP升高。本研究认为Gleason评分、ALP水平、治疗前有无合并SRE、经内分泌治疗后PSA达到的最低值均与患者生存时间相关,但仅是否联合化疗及激素敏感持续时间是与OS相关的独立预后因素。Fizazi等[3]对1 901例mCRPC患者进行分析,结果显示ALP、骨特异性碱性磷酸酶(BSAP)、有无疼痛、既往SRE、首次骨转移出现时间与生存时间相关。对于mCRPC患者化疗后生存相关因素的多因素分析中,化疗前ALP浓度、Hb浓度、激素敏感时间及化疗周期是与生存相关的独立预后因素[17]。有研究显示内分泌治疗后PSA最低值是转移性前列腺癌预后独立因素[18]。
[1] Ferlay J,Shin HR,Bray F,et al.Estimates of worldwide burden of cancer in 2008:GLOBOCAN 2008[J].Int J Cancer,2010,127 (12):2893-2917.
[2] Muralidharan A,Smith MT.Pathobiology and management of prostate cancer-induced bone pain:recent insights and future treatments[J].Inflammopharmacology,2013,21(5):339-363.
[3] Fizazi K,Massard C,Smith M,et al.Bone-related Parameters are the Main Prognostic Factors for Overall Survival in Men with Bone Metastases from Castration-resistant Prostate Cancer[J]. Eur Urol,2014,68(1):42-50.
[4] Halabi S,Lin CY,Small EJ,et al.Prognostic model predicting metastatic castration-resistant prostate cancer survival in men treated with second-line chemotherapy[J].J Natl Cancer Inst, 2013,105(22):1729-1737.
[5] Ottewell PD,Wang N,Meek J,et al.Castration-induced bone loss triggers growth of disseminated prostate cancer cells in bone[J]. Endocr Relat Cancer,2014,21(5):769-781.
[6] Nilsson S,Franzen L,Parker C,et al.Bone-targeted radium-223 in symptomatic,hormone-refractory prostate cancer:a ran⁃domised,multicentre,placebo-controlled phaseⅡstudy[J].Lan⁃cet Oncol,2007,8(7):587-594.
[7] Ryan CJ,Saylor PJ,Everly JJ,et al.Bone-targeting radiopharma⁃ceuticals for the treatment of bone-metastatic castration-resis⁃tant prostate cancer:exploring the implications of new data[J].On⁃cologist,2014,19(10):1012-1018.
[8] Smith MR,Saad F,Coleman R,et al.Denosumab and bone-me⁃tastasis-free survival in men with castration-resistant prostate cancer:results of a phase 3,randomised,placebo-controlled trial [J].Lancet,2012,379(9810):39-46.
[9] Han XX,Wang GW,Zhang C,et al.Survival analysis of 121 pa⁃tients with spinal metastases accepted spinal surgery[J].Chinese Journal of Orthopaedics,2014,34(11):1127-1133.[韩秀鑫,王国文,张 超,等.121例脊柱转移瘤手术治疗的疗效分析[J].中华骨科杂志,2014,34(11):1127-1133]
[10]Nguyen J,Chow E,Zeng L,et al.Palliative response and func⁃tional interference outcomes using the Brief Pain Inventory for spinal bony metastases treated with conventional radiotherapy[J]. Clin Oncol(R Coll Radiol),2011,23(7):485-491.
[11]Bate BG,Khan NR,Kimball BY,et al.Stereotactic radiosurgery for spinal metastases with or without separation surgery[J].Neuro⁃surg Spine,2015,22(4):409-415.
[12]Horwich A,Hugosson J,de Reijke T,et al.Prostate cancer:ES⁃MO Consensus Conference Guidelines 2012[J].Ann Oncol,2013, 24(5):1141-1162.
[13]de Bono JS,Oudard S,Ozguroglu M,et al.Prednisone plus caba⁃zitaxel or mitoxantrone for metastatic castration-resistant pros⁃tate cancer progressing after docetaxel treatment:a randomised open-label trial[J].Lancet,2010,376(9747):1147-1154.
[14]de Bono JS,Logothetis CJ,Molina A,et al.Abiraterone and in⁃creased survival in metastatic prostate cancer[J].N Engl J Med, 2011,364(21):1995-2005.
[15]Narimoto K,Mizokami A,Izumi K,et al.Adrenal androgen lev⁃els as predictors of outcome in castration-resistant prostate can⁃cer patients treated with combined androgen blockade using fluta⁃mide as a second-line anti-androgen[J].Int J Urol,2010,17(4): 337-345.
[16]Hotte SJ,Saad F.Current management of castrate-resistant pros⁃tate cancer[J].Curr Oncol,2010,17(Suppl 2):S72-S79.
[17]Qu YY,Dai B,Kong YY,et al.Survival analysis of patients with metastatic castration-resistant prostate cancer treated with docetaxel plus prednisone[J].Chinese Journal of Urology,2013,34(7):505-509.[瞿元元,戴 波,孔蕴毅,等.多西他赛联合泼尼松治疗转移性去势抵抗性前列腺癌的临床分析[J].中华泌尿外科杂志,2013,34(7):505-509.]
[18]Miyamoto S,Ito K,Miyakubo M,et al.Impact of pretreatment factors,biopsy Gleason grade volume indices and post-treatment nadir PSA on overall survival in patients with metastatic prostate cancer treated with step-up hormonal therapy[J].Prostate Can⁃cer Prostatic Dis,2012,15(1):75-86.
(2015-05-07收稿)
(2015-07-13修回)
(编辑:杨红欣)
Analysis of prognostic factors associated with survival in men with prostate cancer accompanied by spinal metastases at first diagnosis
Luling SHAN,Xiuxin HAN,Chao ZHANG,Zhiwu REN,Shoulei LIANG,Guowen WANG
Department of Bone and Soft Tissue Oncology,Tianjin Medical University Cancer Institute and Hospital,National Clinical Research Center for Cancer,Key Laboratory of Cancer Prevention and Therapy,Tianjin 300060,China
Objective:Prostate cancer frequently metastasizes to the spine.In this study,we investigate the prognostic factors associated with survival in patients with prostate cancer accompanied by spinal metastases at their preliminary diagnosis.Methods:Clinical data of 49 patients who were diagnosed with spinal metastasis from prostate cancer between January 2005 and December 2010 were analyzed.Variables including alkaline phosphatase(ALP),previous skeletal-related event,Gleason score,prostate-specific antigen(PSA)nadir,and time to castration resistance were obtained.Moreover,the relationship between these variables and overall survival(OS)was analyzed.Survival analysis was performed by using Kaplan-Meier curves.Furthermore,the differences among the OS rates were assessed by using the log rank test.The variables were statistically significant in the univariate analysis(P<0.05)and were included in the multivariate model.Results:The average follow-up time was 64.1 months among the 49 patients.By the end of the follow-up,41 of these patients were dead;the mean survival was 27 months.The 1-,3-,and 5-year survival rate was 81.6%,40.8%, and 20.4%,respectively.Univariate analysis identified that 6 variables were statistically significant prognostic factors of OS:with or without chemotherapy,ALP,previous skeletal-related event,Gleason score,PSA nadir,and time to castration resistance.The multivariate analysis showed that the time to castration resistance of≥19 months and the addition of chemotherapy after disease progression are independent prognostic factors for a high OS.Conclusion:With or without chemotherapy and the time to castration resistance are the independent prognostic factors associated with survival in patients with prostate cancer accompanied by spinal metastases at first diagnosis.
prostate cancer,spinal metastasis,chemotherapy,endocrine therapy,prognosis

10.3969/j.issn.1000-8179.2015.17.515
天津医科大学肿瘤医院骨与软组织肿瘤科,国家肿瘤临床医学研究中心,天津市肿瘤防治重点实验室(天津市300060)
王国文 wgwhrb@163.com
单露玲 专业方向为骨与软组织肿瘤临床治疗与基础研究。
E-mail:945490577@qq.com
