SandersⅡ~Ⅲ型跟骨骨折术后完全负重练习开始时间与足部功能关系
2015-12-14付尧王金成贾云龙张汉阳钟专陈高扬刘贺常非
付尧 王金成 贾云龙 张汉阳 钟专 陈高扬 刘贺 常非
(吉林大学第二医院骨科,长春13.41)
SandersⅡ~Ⅲ型跟骨骨折术后完全负重练习开始时间与足部功能关系
付尧 王金成 贾云龙 张汉阳 钟专 陈高扬 刘贺 常非*
(吉林大学第二医院骨科,长春13.41)
背景:SandersⅡ~Ⅲ型跟骨骨折切开复位内固定术后患肢完全负重功能练习的开始时间尚存争议。
目的:探讨SandersⅡ~Ⅲ型跟骨骨折切开复位内固定术后患肢完全负重功能练习的开始时间与足部功能的关系。
方法:选取2010年1月至2013年10月收治的SandersⅡ~Ⅲ型跟骨骨折患者29例36足,按完全负重练习的开始时间分为:A组16例17足,术后6~8周开始部分负重功能锻炼,3个月内开始完全负重锻炼,平均完全负重时间2.8个月;B组13例19足,因个人因素(复合伤、工伤、心理因素等),术后开始完全负重时间大于3个月,平均完全负重时间5.5个月。
结果:随访根据Maryland足部评分标准,A组平均为(91.4±3.4)分,B组平均为(86.3±4.5)分,相比较有统计学差异(P<0.05)。A组切口愈合不良3足,经换药2周愈合;B组切口愈合不良1足,经换药2周愈合,骨髓炎1足,经抗生素骨水泥填充治疗后治愈,两组无明显差别(P>0.05)。A组平均Böhler角29.5°±3.3°,平均Gissan角130.1°±5.4°,骨折均已愈合;B组平均Böhler角31.1°±2.1°,平均Gissan角131.5°±3.9°,骨折均已愈合。两组统计学无明显差异(P>0.05)。
结论:SandersⅡ~Ⅲ型跟骨骨折术后3个月内开始完全负重锻炼患者的足部功能明显优于开始完全负重时间大于3个月的患者。
跟骨骨折;完全负重;锻炼
Background:ound:When to begin fullweight-bearing exercise after open reduction and internal fixation for SandersⅡ-Ⅲcalcaneal fractures is still in dispute.
Objective:tive:To investigate the relationship between joint function recovery and postoperative fullweight-bearing exercise afteropen reduction and internal fixation for treatmentof SandersⅡ-Ⅲcalcaneal fractures.
Methods:hods:A total of 29 patients(36 feet)w ith SandersⅡ-Ⅲcalcaneal fractures treated between January 2010 and October 2013 were enrolled in the retrospective study.According to the beginning time of fullweight-bearing exercise,the patients were divided into two groups.In group A,16 patients(17 feet)began partialweight-bearing exercise at6-8 w eeks postoperatively and fullweight-bearing exercisewithin 3monthspostoperatively(2.8monthson average).In group B,13 patients(19 feet)did fullweight-bearing exercisewith a delay(more than 3months,5.5monthson average)after surgery due to personal reasons,such as combined injury,industrial injury and psychological factors.
Results:ults:The Maryland foot scorewas 91.4±3.4 in group A and 86.3±4.5 in group B,and therewas significantdifference in the Maryland scorebetween groups(P<0.05).Three feet in group A and one foot in group B suffered from a poorhealing of incision and were cured after dressing change 2 weeks later.Osteomyelitis occurred in one foot in group B and were cured by antibiotic bone cement reconstruction.No significant differencewas observed in complications between two groups(P>0.05).A ll fractureswere healed.The average Böhler angle and Gissan angle w as 29.5°±3.3°and 130.1°±5.4°,respectively, in group A.And in group Bwas31.1°±2.1°and 131.5°±3.9°,respectively.Therewasno significantdifference in BöhlerangleorGissan anglebetween two groups(P>0.05).
Conclusions:ions:Foot function in the patientswho perform fullw eight-bearing exercise w ithin 3months postoperatively is superior to thosewith a delaying fullweight-bearing exercise(more than 3monthsaftersurgery).
跟骨骨折约占跗骨骨折的65%,全身骨折的2%[1]。对于累及关节面的跟骨骨折的治疗方法已经争论了近150年[2],随着近年来对跟骨骨折的深入研究,通过外侧入路的切开复位内固定术治疗跟骨骨折已被广泛接受[3]。许多患者手术复位良好,但由于术后缺少早期完全负重锻炼而未获得相应的良好功能[4]。术后何时开始完全负重锻炼是个值得探讨的问题,本研究对跟骨骨折术后完全负重锻炼的开始时间进行了分组比较,结果如下。
1 资料与方法
1.1 临床资料
选取2010年1月至2013年10月收治的跟骨骨折患者52例,均由同一医疗组治疗且术后功能锻炼方法相同,其中12例开放性骨折和6例SandersⅣ型骨折患者均不纳入本研究;除5例失随访外,共29例36足纳入本研究。将其按开始完全负重锻炼的时间分为A、B两组:A组遵循医嘱,术后6~8周开始部分负重功能锻炼(患肢适当用力,必要时需使用助行工具),3个月内开始完全负重功能锻炼(患肢完全着力,不借助任何助行工具),平均完全功能锻炼时间为2.8个月;B组因个人因素(复合伤、工伤、心理因素等),开始完全负重功能锻炼时间大于3个月,平均完全功能锻炼时间为5.5个月。
A组16例17足,年龄17~60岁,平均38.8岁,平均BM I为20.1,随访时间7~28个月,平均15.6个月;B组13例19足,年龄17~51岁,平均38.8岁,平均BM I为23.3,随访时间7~24个月,平均14.8个月,两组比较均无统计学差异(P>0.05)。按Sanders分型[5]均为Ⅱ~Ⅲ型骨折,其中Ⅱ型8足,Ⅲ型28足(表1)。所有患者术前均行跟骨轴、侧位X线片,三维重建CT扫描。
1.2 治疗方法
本组所有患者入院后要求绝对卧床,抬高患肢,使患肢高于右心室水平[6];直至患肢皮肤肿胀消退,张力水泡消失、出现皱褶后给予手术治疗。
两组患者均由同一组医师进行手术,采用连续硬膜外麻醉,取外侧“L”型切口,直视下恢复跟骨高度、长度、后关节面的解剖结构。选取适合的可塑性钛合金跟骨接骨板进行外固定。两组患者早期康复锻炼方法相同,术后给予患肢外固定,术后1周内鼓励患者行足趾及踝关节的主动锻炼,随后逐步进行简单功能锻炼,但两组患者完全负重功能锻炼的开始时间不同:A组患者遵循医嘱,于术后6~8周开始行部分负重功能锻炼,3个月内开始完全负重功能锻炼;B组患者因个人因素(复合伤、工伤、心理因素等),开始完全负重功能锻炼时间大于3个月。
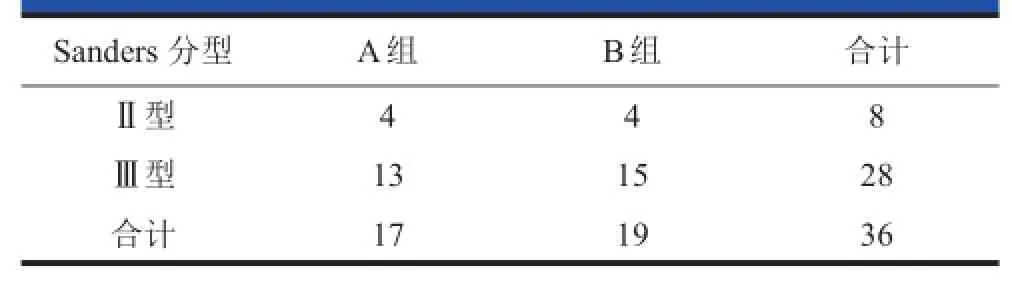
表1 两组病例Sanders nders分型情况(足)
1.3 随访计划及评估指标
所有患者术后6个月和12个月进行随访,以后每年随访一次。术后随访复查跟骨侧、轴位X线片,由未参加手术的医师按照Maryland足部评分标准[3]评价术后患足关节功能(优,90~100分;良,75~89分;中,50~74分;差,<50分)。
1.4 统计学处理
采用SPSS 17.0软件进行统计学分析,两组性别和骨折类型采用Fisher检验,术后Böhler角、Gissane角、平均随访时间、Maryland足部功能评分采用t检验,P<0.05为有统计学差异。
2 结果
按照Maryland足部评分标准评价术后患足功能:A组优10足,良7足,平均(91.4±3.4)分;B组优7足,良11足,中1足,平均(86.3±4.5)分(表2),两组评分有统计学差异(P<0.05)。A组切口愈合不良3足,经换药2周愈合;B组切口愈合不良1足,经换药2周愈合,骨髓炎1足,经含抗生素骨水泥填充治疗后愈合,两组比较无统计学差别。A组平均Böhler角29.5°± 3.3°、平均Gissane角130.1°±5.4°,骨折均已愈合;B组平均Böhler角31.1°±2.1°,平均Gissane角131.5°± 3.9°,骨折均已愈合,两组比较无统计学差异。典型病例见图1、2。
3 讨论
跟骨的重要性、复杂性使跟骨骨折一直受到临床的重视,但仍有许多尚未解决的问题[7]。SandersⅡ~Ⅲ型跟骨骨折的手术治疗中,跟骨解剖复位及患肢制动外固定对骨折的预后及功能有较大影响[8],然而由于术后缺少早期的、正确的完全负重锻炼,许多患者虽然得到了良好的手术复位,却未获得相应的良好功能。许多文献认为早期负重功能锻炼会加大距下关节面塌陷的风险[9,10],而Kienast等[4]通过对136例跟骨骨折患者的随访,提出骨折术后早期完全负重功能锻炼是可行的。Hyer等[11]报导了跟骨骨折内固定术后早期完全负重功能锻炼对固定效果以及跟骨形态无影响。本研究随访A、B两组平均Böhler角分别为29.5°±3.3°和31.1°±2.1°,平均Gissane角分别为130.1°±5.4°和131.5°±3.9°,均无统计学差异,早期负重功能锻炼不会导致骨折移位,亦不影响骨折固定的稳定性[12,13]。反之,早期负重功能锻炼可以降低骨质疏松的发生率,并在一定程度上提高足部功能评分[4]。
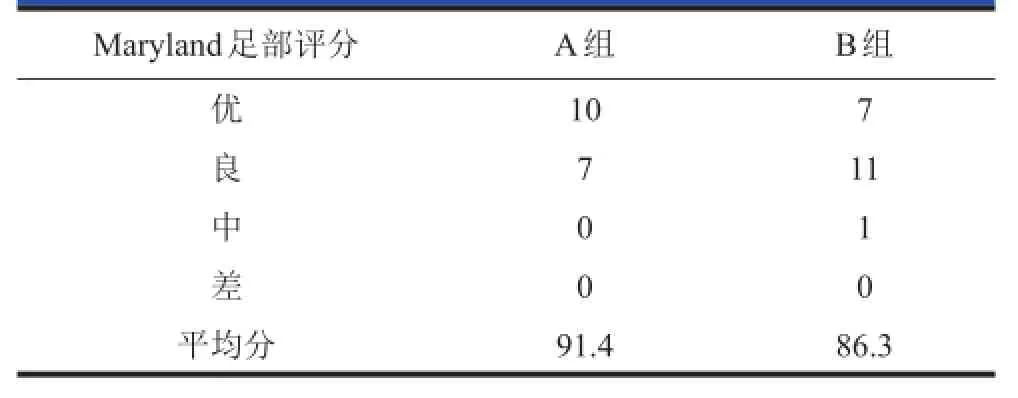
表2 术后随访Maryland yland足部评分结果(足)
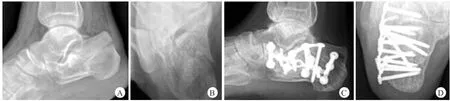
图1 患者,男,37岁,高处坠落伤至右跟骨骨折,术后3个月内开始完全负重锻炼
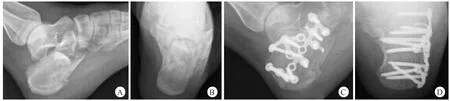
图2 患者,女,24岁,坠落伤致左跟骨骨折,术后完全负重锻炼开始时间超过3个月
本研究中A、B组术后Maryland足部功能评分有显著差异,证明跟骨骨折不但需要恢复跟骨解剖结构,还需要注意恢复患肢功能,尽可能提高患者的生活质量。正确时机的完全负重锻炼,有利于加快患肢循环,减少静脉血栓的形成,有利于关节活动与肌肉力量的恢复;增加了患者恢复患肢功能的信心[14,15]。本研究除完全负重锻炼的开始时间不同,手术团队、治疗方法、初期功能锻炼方法均相同,术后随访由未参加手术的医师按照Maryland足部评分标准进行评测,降低了出错的可能性并增加了结果的可信度。但患者受伤至入院治疗期间的处置方式、出院后患者自身功能锻炼正确与否、患者保险、患者心理等相关不确定因素,以及随访时间较短等,可能对本研究结果产生影响。
本研究证明SandersⅡ~Ⅲ型跟骨骨折术后3个月内开始完全负重功能锻炼在恢复足部功能与提高患者生活质量方面有更好的临床效果。
[1]Sanders R.Displaced intra-articular fractures of the calcaneus.JBone Joint Surg,2000,82(2):225-250.
[2]Rammelt S,Zw ipp H.Calcaneus fractures:facts,controversiesand recentdevelopments.Injury,2004,35(5):443-461.
[3]Veltman ES,Doornberg JN,Stufkens SA,et al.Long-term Outcomes of 1,730 Calcaneal Fractures:Systematic Review of the Literature.JFootAnkle Surg,2013,52(4):486-490.
[4]Kienast B,Gille J,Queitsch C,etal.Early weight bearing of calcaneal fractures treated by intraoperative 3D-fluoroscopy and locked-screw plate fixation.Open Orthop J,2009,3:69-74.
[5]SandersR,Fortin P,Dipasquale T,etal.Operation treatment in 120 displaced intraarticular calcaneal fractures.Results using a prognostic computed tomography scan classification.Clin Orthop RelatRes,1993,(290):87-95.
[6]Bergin PF,Psaradellis T,K rosin MT,etal.Inpatient Soft Tis-
sue Protocol and Wound Complications in Calcaneus Fractures.FootAnk le Int,2012,33(6):492-497.
[7]Stapleton JJ,ZgonisT.SurgicalTreatmentof Intra-articular calcaneal fractures.Clin PodiatrMed Surg,2014,3.4):539-546.
[8]Shen Yi,WangWeili,Han Xiaofeng.Effect of early dirigation on the recovery of foot function after the operation of the fracture of calcaneus:the blind evaluation based on 6-month follow-up.Chinese Journal of Clinical Rehabilitation,2005,9(18):220-221.
[9]Ishikawa SN.Fractures and dislocations of the foot.In:Canale ST,Beaty JH,editors Cam pbell’s Operative Orthopaedics.12th ed.Canada:Mosby.2013:413.4146.
[10]Sanders RW,Clare MP.Calcaneus fractures.In:Bucholz RW,Court-Brown CM,Heckman JD,TornettaⅢP,editors. Rockwood and Green's Fractures in Adults.7th ed.Vol 2. Philadelphia:Lippincott,Williams and Wilkins.2010:2065-2110.
[11]Hyer CF,A tw ay S,Berlet GC,etal.Early w eight bearing of calcaneal fractures fixated w ith locked plates:a radiographic review.FootAnkle Spec,2010,3(6):320-323.
[12]K line AJ,Anderson RB,DavisWH,et al.M inimally invasive technique versus an extensile lateral approach for intraarticular calcaneal fractures.Foot Ankle Int,2013.4(6): 773-780.
[13]Nosew icz T,Knupp M,Barg A,et al.M ini-open sinus tarsi approach w ith percutaneous screw fixation of displaced calcaneal fractures:a prospective computed tomography-based study.FootAnkle Int,2012,33(11):925-933.
[14]GeelCW,Flemister AS Jr.Standardized treat-mentof intraarticular calcaneal fractures using an oblique lateral incision and no bone graft.JTrauma,2001,50(6):1083-1089.
[15]孙宏慧,王强,唐农轩.跟骨骨折的手术治疗.中国矫形外科杂志,2001,8(12):1232-1236.
Relationship between fullweight-bearing exerciseand joint function in postoperative Sanders ndersⅡ--Ⅲcalcaneal fractures
FUYao,WANGJincheng,JIAYunlong,ZHANGHanyang,ZHONGZhuan,CHENGaoyang,LIUHe,CHANGFei*
(Departmentof Orthopedics,The Second Hospitalof Jilin University,Changchun 13.41,China)
ords:Calcaneal fracture;Fullweight-bearing;Exercise
2095-9958(2015)02-0 062-04
10.3969/j.issn.2095-9958.2015.01-012
*通信作者:常非,E-mail:759273996@qq.com
