Clinical Study on Fu’s Subcutaneous Needling with Laser for Postherpetic Neuralgia
2014-06-19GuoLihongChenXiong2HuangPingLiangYongcuiMuJingping
Guo Li-hong, Chen Xiong2, Huang Ping, Liang Yong-cui, Mu Jing-ping
1 Department of Acupuncture and Moxibustion, Taihe Hospital, Hubei University of Medicine, Shiyan 442000, China
2 Hubei University of Chinese Medicine, Wuhan 430065, China
CLINICAL STUDY
Clinical Study on Fu’s Subcutaneous Needling with Laser for Postherpetic Neuralgia
Guo Li-hong1, Chen Xiong2, Huang Ping1, Liang Yong-cui1, Mu Jing-ping1
1 Department of Acupuncture and Moxibustion, Taihe Hospital, Hubei University of Medicine, Shiyan 442000, China
2 Hubei University of Chinese Medicine, Wuhan 430065, China
Author: Guo Li-hong, associate chief nurse
Objective: To observe the therapeutic efficacy of Fu’s subcutaneous needling (FSN) with laser for postherpetic neuralgia and analyze its action mechanism.
Methods: A total of 102 cases with postherpetic neuralgia were randomly allocated into a treatment group and a control group, 51 in each group. FSN with laser was used for patients in the treatment group, whereas electroacupuncture was used for patients in the control group. After 6 months of treatment, the total effective rates, action time and cure courses in recovery cases were compared between the two groups. Three months after the treatment was completed, a follow-up was done to compare relapse rates between the two groups.
Results: The recovery and total effective rates in the treatment group were 56.9% and 94.1% respectively, versus 35.3% and 68.6% in the control group, showing statistical differences (P<0.05); the action time and cure courses in the observation group were significantly shorter than those in the control group (P<0.05); the relapse rate in the treatment group was 6.9%, versus 44.4% in the control group, showing a statistical difference (P<0.05).
Conclusion: FSN with laser can obtain better effect for postherpetic neuralgia than electroacupuncture and pose lower relapse risks.
Fu's Subcutaneous Needling; Lasers; Acupuncture Therapy; Herpes Zoster; Neuralgia, Postherpetic
Herpes zoster results from reactivation of varicella-zoster virus (VZV). After initial episode of chickenpox resolves, the virus remains latent in the neurons of spinal dorsal root ganglia. When immunity to VZV declines because of fatigue or infection, the virus reactivates and travels down the nerve axons to cause viral infection and pain in the affected region[1]. The spontaneous agonizing or tearing pain can interfere with the patients’ sleep and greatly affect their quality of life. We’ve used FSN with laser for postherpetic neuralgia (PSN). The results are now summarized as follows.
1 Clinical Materials
1.1 Diagnostic criteria
The diagnosis of PSN can be made according to the relevant literature[2]: a history of herpes zoster and persistent pain from 1 month to 2 years upon recovery; pain and paraesthesia according to nerve distributions, coupled with local pigmentation; the nature of pain is paroxysmal stabbing, electric shock, burning or binding; other discomfort following nerve injury such asitch, binding and formication; psychological stress and emotional depression.
1.2 Inclusion criteria[3]
Those who met the above diagnostic criteria with a duration of <3 years; aged between 15 and 75;having not received medication or other therapies during the last week; having no allergic constitution or history of drug allergy; and those who were willing to participate in the trial and sign the informed consent.
1.3 Exclusion criteria
Those with special types of herpes zoster, such as herpes zoster involving the eyes, ears, internal organs and meninges and generalized zoster; having acute herpes zoster with unhealed skin lesion; having complications of severe heart, brain, kidney and hematopoietic system diseases; having malignant cancer, diabetes and psychosis.
1.4 Statistical method
The SPSS 17.0 version statistical software was used for data analysis. The measurement data were expressed asusingt-test. The numeration data were expressed percentage, using Chi-square test. APvalue<0.05 indicates a statistical significance.
1.5 General data
A total of 102 PSN cases were treated in Acupuncture Department of our hospital between May 2010 and May 2013. They were randomly allocated into a treatment group and a control group according to the visit order, 51 cases in each group. Of 51 in the treatment group, there were 27 males and 24 females aged between 30 and 70, with a mean age of (40.3±4.5) years. Their durations were between 1 d and 24 months, with a mean duration of (11.3±3.4) months. Of 51 cases in the control group, there were 26 males and 25 females aged between 30 and 72, with a mean age of (41.4±5.6) years. Their durations were between 2 d and 12 months, with a mean duration of (11.8±3.8) months. Of 102 cases, there were 22 cases with postherpetic trigeminal neuralgia, 24 cases with thoracic neuralgia, 26 cases with lower abdominal neuralgia, 20 cases with lumbar neuralgia, 5 cases with ulnar neuralgia, and 5 cases with sciatica. There were no statistical significances (P>0.05) in gender, age and duration between the two groups, indicating that the two groups were comparable.
2 Treatment Methods
2.1 Treatment group
Points: Find the painful spots and mark them. Determine the number of needles according to the painful area and usually retain 1-2 needles. Insert needles to symmetrical spots along the border of painful area, 6-10 cm superior or inferior to the painful spots.
Method: The medium-sized disposable Fu’s subcutaneous needles were manufactured by Nanjing Paifu Medical Science & Technology Co., Ltd. (Appliance Permit Number 2270536 of 2007 by Food and Drug Administration of Jiangsu Province). The posture of the patient should be comfortable and adjusted to fully expose the painful area. After routine sterilization, the practitioner held the FSN needle using the right hand and tightened the skin using the left thumb and index finger, then applied a fast insertion subcutaneously at an angle of 15-25°. The needle tip directed to the nerve root. After this, conducted an even left-right swaying movement and kept communicating with the patient. After retaining the needle for 10 min, took out the needle core and connected with the optical fiber in SJ-L laser needle knife. As for the laser current, the wavelength of 670 nm, output of 60-80 mW, power density of 30 mW/mm2and energy density of 96 J/mm2were used for 20 min. After covering the needle holes with cotton balls, fixed the soft rubber tube using adhesive pastes, and removed the FSN needles after 24 h. The treatment was done once every other day, 7 d for 1 course of treatment. There was a 1-day interval between two courses. The treatment lasted for six months. The patients were asked to be careful about the immobilization of FSN needles, to keep the local area clean and avoid intense activities and shower.
2.2 Control group
Points: For herpes zoster on the head, use local painful spots plus Hegu (LI 4) and Taichong (LR 3); for herpes zoster on the shoulder, back, chest, low back or hypochondriac area, use distal painful spots plus Jiaji (EX-B 2) points of corresponding nerve segments on the affected side and Zhigou (TE 6); for herpes zoster on the four limbs, use distal painful spots plus Quchi (LI 11) for the upper limb and Zusanli (ST 36) for the lower limb.
Method: The posture of the patient was adjusted to expose the points. After routine sterilization, inserted about 1 cun perpendicularly to Hegu (LI 4), Taichong (LR 3), Zhigou (TE 6), Quchi (LI 11) and Zusanli (ST 36) using filiform needles of 0.25 mm in diameter and 40-50 mm in length; applied encircling method to local painful spots on the head; inserted from distal painful spots subcutaneously along the nerve root for pain in the shoulder, back, chest, low back and hypochondriac area; punctured Jiaji (EX-B 2) points obliquely towards the spine; inserted from distal painful spots subcutaneously towards the torso for pain in the four limbs. Four to six points were selected for each treatment. Even reinforcing-reducing manipulation was conducted upon arrival of qi. Then the needles were connected with G-6805 electric stimulator using sparse-dense wave, frequency of 4 Hz for sparse wave and 10 Hz for dense wave and tolerable current strength, and retained the needles for 30 min. The treatment was done once every day, 7 d made up a course of treatment. There was a 1-day interval between two courses. The treatment lasted for 6 months.
3 Treatment Effect
3.1 Evaluation on action time
The visual analogue scale (VAS) score was used to evaluate the action time[4]: VAS score ≤2 points indicates marked effect. After each treatment, every patient was graded and the action time was recorded.
3.2 Criteria for therapeutic efficacy
This was made according to theCriteria of Diagnosis and Therapeutic Effects of Diseases and Syndromes in Traditional Chinese Medicine[5].
Recovery: Absence of pain, and normal sleep, diet and daily living.
Improvement: Alleviated pain, paroxysmal pain upon fatigue or cold and improved sleep, diet and daily living.
Failure: Burning stabbing pain remains unalleviated, and poor sleep, diet and daily living.
3.3 Follow-up
The follow-up started three months after the treatment was over. The long-term effect including signs, symptoms and adverse reactions were all recorded.
3.4 Treatment results
3.4.1 Between-group comparison on clinical effect
The recovery and total effective rates in the treatment group were 56.9% and 94.1% respectively, versus 35.3% and 68.6% in the control group, showing statistical differences in recovery rate (P<0.05) and total effective rate (P<0.05), (Table 1).
3.4.2 Between-group comparison on clinical action time and treatment courses
VAS score comparison showed that the average action time in the treatment group was significantly shorter than that in the control group (P<0.01); and the recovery treatment courses in the treatment group were significantly less than those in the control group (P<0.01), (Table 2).
3.4.3 Between-group comparison on relapse rates among recovery cases
The follow-up 3 months after the treatment was over showed that the relapse rate in the treatment group was 6.9%, versus 44.4% in the control group, showing a statistical significant difference (P<0.05), (Table 3).

Table 1.Between-group comparison on clinical effect (case)
Table 2. Between-group comparison on action time and recovery treatment courses
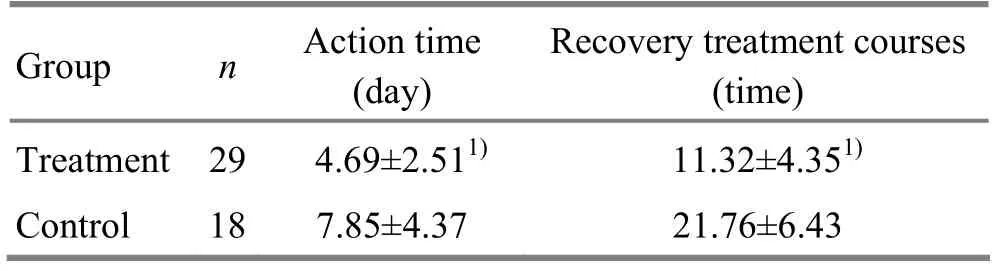
Table 2. Between-group comparison on action time and recovery treatment courses
Note: Compared with the control group, 1) P<0.01
?

Table 3. Between-group comparison on relapse rates in recovery cases (case)
4 Discussion
In Chinese medicine, PSN falls under the category of ‘Bi-Impediment syndrome’. It refers to persistent burning or stabbing pain after the skin lesion heals. Generally, 9%-13% of herpes zoster patients may develop PSN. The risk of developing PSN increases with age. It’s estimated that 15%-75% individuals over age 50 who develop the herpes zoster also develop PSN and the pain may last for longer than 1 year[5]. This condition is characterized by a girdle-like unilateral pain along the affected nerves[6]. In modern medicine, the virus enters the host via the respiratory system and remains latent in nerve cells of the spinal dorsal root ganglion or other afflicted regions[7]. The immunity to VZV declines because of fatigue or infection may trigger this condition. Conventionaltherapies include prescription narcotic analgesics, antidepressants, anticonvulsants and nerve block injections, albeit with mild or moderate success[8].
FSN is a novel therapy developed over the last decade. It is a modern form of acupuncture based on cutaneous region theory, principle of treating the local area, using painful area as points and classical needling techniques inHuang DiNei Jing(Yellow Emperor’s Classic of Internal Medicine)[9].
The FSN inserts the local area surrounding the pain, stops at the subcutaneous layer and the needle tip directs to the painful region. Clinical practice has proven that FSN can obtain immediate pain-relief and long-term effectiveness during needle retaining, which might be related to its regulation on nervous system and humoral factors[10]. Low-intensity laser irradiation can produce significant bio-stimulation and regulation via biochemical reaction of light. On one hand, it stimulates the defense and immune system to enhance the role of phagocytic white blood cells, increases immunoglobulins, boosts adrenal cortex function and exerts antiviral, anti-inflammatory and pain-relief effects in the local area. On the other hand, it dilates capillaries to improve local blood circulation, increases exchange of nutrients and oxygen, accelerates discharge of metabolic products and algesic substance and thus increases the pain threshold and relieves pain. Some patients may still experience swelling and limited movement after alleviation of pain, this is mainly associated with local inflammation, edema, adhesion or subluxation or derangement of facet joints[11]. Consequently, we added laser irradiation on top of FSN and found a better effect when compared with traditional electroacupuncture. FSN with laser can obtain FSN effects coupled with thermal effect, mechanical effect, photochemical effect and electromagnetic effect. This can further dilate blood vessels, increase metabolism and improve circulation to eliminate inflammation, stop pain and resolve swelling. As for the affected area, laser irradiation plays an active role in regulating physiological functions, improving pathological state, increasing blood circulation, accelerating metabolism, and recovering from tissue injury[12]. However, it is important to prevent needle faint during treatment, especially for first-visit patients. Preventive measures include helping the patients to relax, choosing an appropriate position, using mild manipulation, communicating with the patients and managing immediately once warning signs are present[13].
In summary, FSN with laser is easy to operate, pain-free and effective for PSN and deserves further clinical application.
Conflict of Interest
The authors declared that there was no conflict of interest.
Acknowledgments
This work was supported by Taihe Hospital, Hubei University of Medicine.
Statement of Informed Consent
All of the patients signed the informed consent.
[1] Ni JX, Fan BF, Xue FS. Clinical Pain Management Technique. Beijing: Scientific and Technical Documentation Press, 2003: 91.
回眸“青海盐湖”的创业史,万千人、万千事、万千成就、万千精彩、万千辉煌纷至沓来。蓦然回首风雨历程,有许多所思、所想、所悟和所行。六十年时间,无疑是一段值得凝练、铭记和怀想的时光,更是一份精神传承!
[2] Chen HP, Chen J, Yang YK, Lu YH, Xiang DL. Clinical observation on different oblique needling methods for postherpetic neuralgia. Zhenjiu Linchuang Zazhi, 2009, 25(4): 31-33.
[3] Chen PF, Zheng CY. Clinical observations of electroacupuncture and bleeding cupping therapy in treating postherpetic neuralgia of herpes zoster. Xiandai Linchuang Yixue, 2010, 36(1): 45-46.
[4] Liao HS, Zhu YL. Rehabilitation Assessment and Treatment of Cerebral Apoplexy. Beijing: Huaxia Press, 1996: 79-83.
[5] State Administration of Traditional Chinese Medicine. Criteria of Diagnosis and Therapeutic Effects of Diseases and Syndromes in Traditional Chinese Medicine. Nanjing: Nanjing University Press, 1994: 259-260.
[6] Peng WW. Lemology. 6th Edition. Beijing: People’s Medical Publishing House, 2005: 50-53.
[7] Liang D, Dai LY, Shen W. Gabapentin and transcutaneous electrical nerve stimulation for the treatment of postherpetic neuralgia. Zhongguo Xiandai Yiyao Zazhi, 2011, 13(2): 61-63.
[9] Fu ZH. Fu’s Subcutaneous Needling. Beijing: People's Military Medical Press, 2000: 9-12.
[10] Fu ZH, Huang Y, Xia DB, Deng Y. Characteristics of Fu’s subcutaneous needling, question and answer. Zhenjiu Linchuang Zazhi, 1997, 13(2): 1.
[11] Zhang YP. Fu’s subcutaneous needling: a novel needling analgesic method. Zhenjiu Linchuang Zazhi, 1998, 14(12): 37-40.
[12] Chen JM, Mu JP, Peng L, Ao JB, Chen JM. Laser acuknife for degenerative knee: a clinical observation. Zhongguo Jiguang Yixue Zazhi, 2007, 16(5): 16-21.
[13] Liu BH, Zhu XW. About Fu’s subcutaneous needling. Zhenjiu Linchuang Zazhi, 1998, 14(4): 290-291.
Translator:Han Chou-ping
Mu Jing-ping, M.D., associated professor.
E-mail: cdscds1226@126.com
R246.6
: A
Date:February 20, 2014
猜你喜欢
杂志排行

Journal of Acupuncture and Tuina Science的其它文章
- Observation on Clinical Effects of Tuina plus Hot Compress for Infantile Diarrhea Due to Spleen-kidney Yang Deficiency
- Clinical Study on Point Application Using Chinese Herbal Medicine for Pediatric Chronic Cough
- Therapeutic Effect Observation on Combining Electroacupuncture and Tuina for Migraine
- Therapeutic Efficacy Observation on Combined Taijiquan and Auricular Point Sticking for Perimenopausal Insomnia
- Blood Perfusion Effect of Acupuncture on Acute Facial Paralysis Observed by Laser Speckle Technique
- Therapeutic Efficacy of Tuina in Treating 48 Cases with Knee Osteoarthritis