腹腔镜下保留胆囊的毗邻胆囊肝细胞癌一次性完全射频消融治疗
2013-09-12姜凯苏明刘洋赵向前陈永卫张文智王敬董家鸿黄志强
姜凯,苏明,刘洋,赵向前,陈永卫,张文智,王敬,董家鸿,黄志强
腹腔镜下保留胆囊的毗邻胆囊肝细胞癌一次性完全射频消融治疗
姜凯,苏明,刘洋,赵向前,陈永卫,张文智,王敬,董家鸿,黄志强
目的评估腹腔镜下对毗邻胆囊的肝细胞癌进行一次性完全射频消融(RFA)治疗的可行性与安全性。方法选取毗邻胆囊周边不同部位的肝细胞癌患者5例,肿瘤直径2.5~4.2cm,采用腹腔镜辅助射频消融治疗,腹腔镜下对胆囊不作分离与切除,射频消融过程保中持胆囊壁的连续完整。术后通过B超及CT了解肿瘤有无复发,并观察患者生存状况。结果术后3d行B超检查见胆囊壁近消融区处边缘增厚,厚度0.3~0.5cm,CT显示胆囊壁密度增高。术后6个月增强CT显示5例患者肿瘤边缘均无强化,胆囊完整,达到肿瘤一次性完全消融。随访18~36个月,所有患者均生存良好。结论腹腔镜下对毗邻胆囊的肝细胞癌达到一次性完全消融并保持胆囊壁的连续与完整在技术上是安全可行的。
癌,肝细胞;射频消融术;腹腔镜
射频消融(radiofrequency ablation,RFA)是治疗某些肝细胞癌(hepatocellular carcinoma,HCC)的有效手段[1]。对于肝脏特殊部位的肿瘤,射频消融治疗可引起出血、胆汁漏、胆囊穿孔等严重并发症[2-4],需要联合酒精注射进行补充治疗[5]。对于毗邻胆囊的HCC,切除胆囊后再进行射频消融是安全的,但是,当肿瘤与胆囊密切相连无法分离,或因重度肝硬化而无法进行胆囊切除时,在保留胆囊的情况下能否达到肿瘤的一次性完全射频消融目前尚未见文献报道。本文对5例此类典型患者进行射频消融治疗,探讨保留胆囊、腹腔镜下毗邻胆囊HCC一次性完全射频消融治疗的理论基础、技术要点及并发症情况。
1 资料与方法
1.1一般资料 选取肿瘤毗邻胆囊0~0.5cm的 HCC典型病例5例,均为男性,年龄43~70岁,肿瘤直径2.5~4.2cm,具体资料见表1。
1.2射频消融治疗过程 射频消融设备使用Ra-dionics Cool-tipTMRF Ablation System(Valleylab,USA),采用内置的水冷系统保持射频电极尖端温度低于20℃。5例患者均全身麻醉,射频消融治疗过程如下:①腹腔镜探查腹腔内有无腹水和(或)肿瘤转移,肝脏硬化程度,胆囊壁表现(有无水肿),以及胆囊与肿瘤表面之间的血管联系(病例1、2、4肿瘤与胆囊壁之间有多支血管交通支,直径0.2~0.3cm,图1C);②分离胆囊与大网膜或结肠之间的粘连,使胆囊与结肠完全隔离;根据术前CT或MRI影像评估结果,确定置入电极的方向及深度,避免穿刺损伤胆囊下后方右侧的门静脉及胆管;③自肿瘤远离胆囊壁的一侧边缘,将单射频电极(3cm active-tip cooled)准确斜穿置于肿瘤底部,使电极与胆囊壁距离1.5~2.0cm;避免电极直接穿入胆囊脏面的任何部位;④射频消融初始能量输送90W,预热10min后,将设备能量增至最大值(200W),自动反馈平衡调节,能量变化范围96~142W,持续至20min时,腹腔镜实时监测肿瘤表面血管内气体流动方向,若气泡沿肿瘤与胆囊间的血管流向胆囊底部,则以腹腔镜吸引器适当加压阻断血管,避免河流效应对胆囊的整体损伤作用;⑤肿瘤消融过程中,以吸引器对肿瘤向远离胆囊的方向适当加压,使电极与肿瘤组织密切接触,提高输出功率的有效作用时间;⑥若腹腔镜观察发现肿瘤所在肝段表面颜色与周围肝脏差别较大,则以集束射频电极(2.5cm active-tip cooled)继续以最高能量持续消融12~24min,直至将该颜色变暗区域肝段完全消融;⑦治疗过程中应始终密切观察胆囊壁的颜色变化,避免突然的高温使受损胆囊壁破裂;应对胆囊底部及体部靠近肝脏或肿瘤的一侧进行射频消融使之产生热损伤(颜色变为浅黑色或深褐色),胆囊壁的损伤距肿瘤<1.5cm(图1D);⑧当肿瘤表面与周围血管内气体流动的现象消失后,肿瘤组织色泽变为浅褐色或深褐色,此时停止消融及冷循环,测得射频电极尖端温度范围76~82℃;⑨仔细检查穿刺针道有无出血及胆汁漏,并及时进行压迫、电凝或封堵处理;⑩将大网膜以氰基丙烯酸盐黏合胶(α-cyanoacrylate,广州白云医用生物胶有限公司)粘连于胆囊热损伤的创面;观察15min,确认无胆汁漏。术后禁食水并胃肠减压3d。
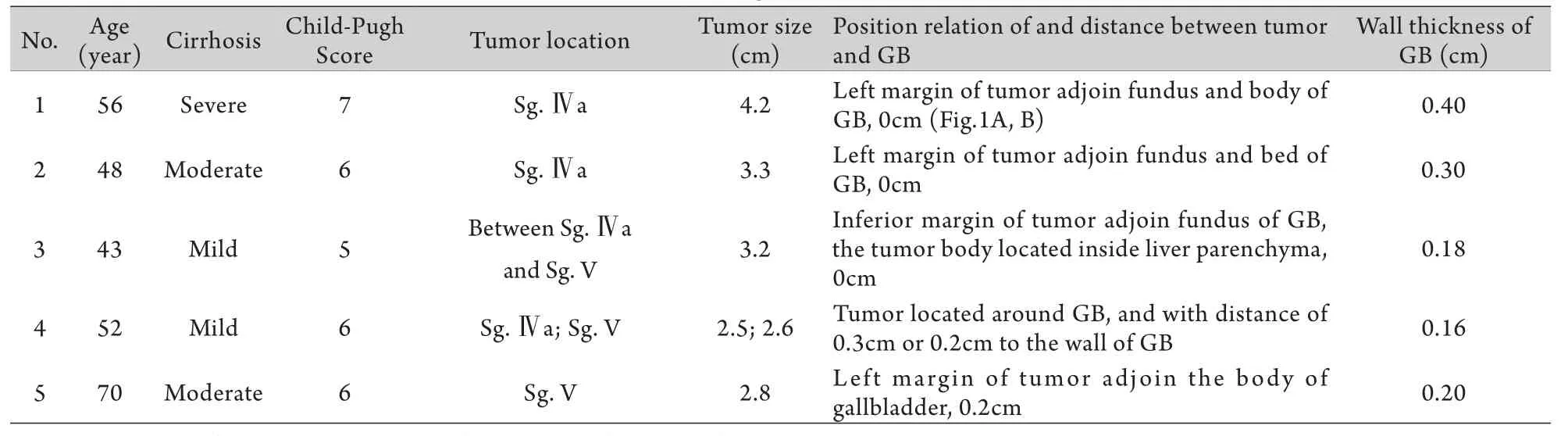
表1 5例患者的临床与影像学表现Tab. 1 Clinical and image characteristics of 5 patients
2 结 果
5例患者均采用射频消融对胆囊壁毗邻肿瘤的局部进行完全或不完全损伤(胆囊壁距肝脏损伤1.0~1.5cm)。射频消融术后7d,复查肝功能指标均接近术前水平。病例2、4术后1d出现右上腹部轻度疼痛,2~3d后症状消失。所有患者术后3d复查B超均提示胆囊壁近消融区处水肿增厚,厚度0.3~0.5cm,周围无积液,同时增强CT见消融范围完全覆盖病变,胆囊壁密度增高、连续完整。
5例患者术后1个月复查B超及CT,结果显示靠近肿瘤处的胆囊壁回声增强、密度增高,周围无积液;术后6个月肝脏增强CT显示无肿瘤复发,胆囊壁连续完整,达到肿瘤一次性完全消融。随访18~36个月,所有患者均生存良好,病例2术后36个月Ⅵ段与Ⅶ段交界处发现新生肿瘤(大小1.9cm×1.8cm)。病例1术后不同时间CT复查肿瘤与胆囊表现见图1E-H。
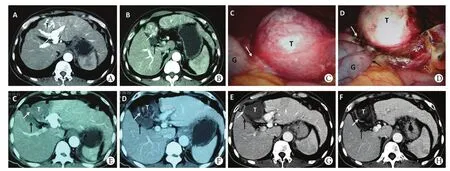
图1 毗邻胆囊Ⅳa段HCC的射频消融治疗与复查表现Fig. 1 Manifestation of RFA treatment to HCC in Segment Ⅳa adjoining to gallbladderA. Contrast enhanced CT: The tumor (T) with complete capsule was showed enhanced in arterial phase (white hollow arrow), and arteriovenous fistula was indicated by white solid arrow; B. Left margin of tumor (T) adjoined to body and fundus of GB (white solid arrow), and thickening of GB wall was seen (black solid arrow); C. Tumor (T) and gallbladder (G) connected closely, and serosa of G and capsule of T stretched with visible communicating vessel (white solid arrow); D. At the end of RFA, the tumor (T) turned into dark yellow among ablated region (2.0cm in range, white hollow arrow); and fundus of gallbladder (G, white solid arrow) changed into dark brown, 1.5cm away from T, meanwhile, G wall near the ablated region swollen slightly (black solid arrow); capsule of T and wall of G kept continuing and complete; E. Contrast enhanced CT 3 days after RFA: The ablated region (5.6×5.3cm) completely covered the tumor (T), and stretched to Sg. Ⅳa (white hollow arrow); thickened GB wall with enhanced density in arterial phase was seen in boundary (white solid arrow) and right GB wall was intact (black solid arrow); F. 1.5cm inferior layer of C: High density and thickening of GB wall (white solid arrow) adjoined to tumor was visible and the rest part of GB wall showed no change (black solid arrow); G. 18 months after RFA: Complete ablation and decreased tumor (T) with no obvious recurrence. The higher density of boundary of GB wall adjoined to previous tumor which was prominent inside GB bed, showing the continuity and completeness of GB wall (brown solid arrow); H. 1.5cm inferior layer of E: The continuity and completeness of GB wall (white solid arrow) was indicated by higher density than the other side of GB wall (black solid arrow)
3 讨 论
毗邻胆囊(距离<0.5cm)部位被认为是HCC经皮穿刺射频消融治疗中危险的特殊位置之一[1,5]。关于特殊位置的肿瘤,一般认为是指毗邻肝内主要胆管与血管,或位于肝脏表面且毗邻重要器官的肿瘤,以及消融治疗可能引起严重并发症部位的肿瘤[1,6-8]。但这一概念是相对而言的,比如对于非外科条件来说,肝脏脏面与膈面的位置是特殊的,但在外科条件下,借助腹腔镜的辅助,这些部位的消融又是相对简单安全的[2,9];同时,假如不能达到肿瘤完全消融的目的,这些部位的肿瘤也不能称为真正意义上的特殊位置肿瘤。
因此,基于外科手术局部切除肿瘤的原则,我们认为,特殊位置应该定义为位于肝内或肝表面,毗邻重要血管与胆管,或与脏器关系密切且无法隔离治疗,在进行一次性完全消融时可能引起严重并发症的部位。对于毗邻胆囊的肿瘤来说,剥离或切除胆囊后再进行肿瘤射频消融治疗是安全的,因为这一做法使肿瘤的特殊位置变为普通位置。然而,Levit等[2]对距胆囊<1cm的肿瘤在术前进行经皮穿刺胆囊内胆汁引流,术中采用腹腔镜辅助射频消融联合病灶剥离,但仍有部分患者存在肿瘤残留,需要再次行射频消融治疗。
重度肝硬化时胆囊的病理生理学改变具有特殊性。一方面,作为门静脉高压症的侧支循环代偿,胆囊与肝脏之间的静脉代偿性增粗、压力升高;另一方面,因门静脉高压及低蛋白血症,胆囊壁出现明显的水肿、增厚。前者因存在术中大出血的可能,不利于腹腔镜下胆囊的分离及切除[8],而后者为射频消融治疗提供了更大的消融范围,且可降低胆囊壁被完全毁损的可能。本组中病例1、2合并有重度肝硬化,胆囊壁水肿明显,同时胆囊与肝脏肿瘤之间出现增生代偿的静脉回流血管,在对肿瘤进行射频消融的过程中,热量随增粗的血管流向胆囊壁的浆膜外层,持续高热可能对整个胆囊壁造成损伤,因此,术中以吸引器头端对存在明显气泡流动的血管给予加压阻断[10],使胆囊壁的损害限于游离胆囊壁1.5cm以内,确保肿瘤周围组织的消融范围达到1.0cm以上(图1D)。当合并轻到中度肝硬化时,胆囊壁正常或稍增厚。因不存在胆囊壁的血管代偿性增粗,射频消融容易毁损胆囊壁浆膜层的血管,胆囊壁完全毁损后形成硬痂,因胆囊未破裂而保持了胆囊壁与血管壁的连续完整;同时,受损胆囊壁神经末梢被完全毁损,因神经反射导致的临床症状可减轻或消失。本组病例3、4、5的胆囊壁及血管完全毁损,术后未出现相应的急性胆囊炎症状。病例3肿瘤位于胆囊床的后方肝脏实质之内,由于胆囊与肝脏接合处保持完整,即使胆囊床处的胆囊壁完全消融坏死,胆汁也不会进入腹腔。病例2、4之所以术后第1天出现右上腹轻度疼痛症状,可能与胆囊周围组织广泛毁损,高热量对胆囊处腹膜的刺激有关。
大网膜在胆囊炎性穿孔时具有积极的保护性粘连反应,因此,我们将这种反应提前至术中用于即时保护,以氰基丙烯酸盐黏合胶将大网膜粘连于受损的胆囊壁处,使胆囊壁损伤后可能发生的胆囊穿孔急性过程变为受保护后的慢性过程。本组消融术后3~5d行B超检查发现除消融边缘胆囊壁水肿增厚(0.3~0.5cm)外,未发现胆囊周围的渗出表现。术后1个月B超及CT检查显示靠近肿瘤处的胆囊壁回声增强、密度增高,与胆囊壁完全消融凝固有关。术后6个月复查肝脏CT,5例患者肿瘤消融处未发现任何复发征象,胆囊整体完整性良好,表明毗邻胆囊(0~0.5cm)的HCC达到了一次性完全消融。
综上所述,本组结果显示,射频消融过程中保持胆囊壁的连续及完整性,不进行胆囊分离,在腹腔镜下对毗邻胆囊的肝细胞癌进行一次性完全消融是安全可行的。
[1] Ansari D, Andersson R. Radiofrequency ablation or percutaneous ethanol injection for the treatment of liver tumors[J]. World J Gastroenterol, 2012, 18(10): 1003-1008.
[2] Levit E, Bruners P, Günther RW, et al. Bile aspiration and hydrodissection to prevent complications in hepatic RFA close to the gallbladder[J]. Acta Radiol, 2012, 53(9): 1045-1048.
[3] Pua U, Merkle EM. Case report. Spontaneous cholecystocolic fistula and locoregional liver tumour ablation: a cautionary tale[J]. Br J Radiol, 2011, 84(1008): e243-e245.
[4] Tang Z, Fang H, Kang M, et al. Percutaneous radiofrequency ablation for liver tumors: Is it safer and more effective in low-risk areas than in high-risk areas[J]? Hepatol Res, 2011, 41(7): 635-640.
[5] Kurokohchi K, Watanabe S, Masaki T, et al. Combination therapy of percutaneous ethanol injection and radiofrequency ablation against hepatocellular carcinomas difficult to treat[J]. Int J Oncol, 2002, 21(3): 611-615.
[6] Yamamoto T, Kubo S, Hirohashi K, et al. Secondary hemocholecyst after radiofrequency ablation therapy for hepatocellular carcinoma[J]. J Gastroenterol, 2003, 38(4): 399-403.
[7] Hildebrand P, Kleemann M, Roblick U, et al. Laparoscopic radiofrequency ablation of unresectable hepatic malignancies: indication, limitation and results[J]. Hepatogastroenterology, 2007, 54(79): 2069-2072.
[8] Laurence JM, Tran PD, Richardson AJ, et al. Laparoscopic or open cholecystectomy in cirrhosis: a systematic review of outcomes and meta-analysis of randomized trials[J]. HPB (Oxford), 2012, 14(3): 153-161.
[9] Yi B, Somasundar P, Espat NJ. Novel laparoscopic bipolar radiofrequency energy technology for expedited hepatic tumour ablation[J]. HPB (Oxford), 2009, 11(2): 135-139.
[10] Kai J, Ming S, Yang L, et al. Complete radio frequency ablation of hepatocellular carcinoma adjacent to the main bile duct and blood vessels between the first and the second hepatic portal[J]. Cell Biochem Biophys, 2012 [Epub ahead of print].
Laparoscopy-assisted and gallbladder-preserved one-off radiofrequency ablation for hepatocellular carcinoma adjoining gallbladder
JIANG Kai, SU Ming, LIU Yang, ZHAO Xiang-qian, CHEN Yong-wei, ZHANG Wen-zhi, WANG Jing, DONG Jiahong*, HUANG Zhi-qiang
Department of Hepatobiliary Surgery, General Hospital of PLA, Beijing 100853, China
*Corresponding author, E-mail: dongjh301@163.com
This work was supported by the National Key Technology Research and Development Program of China (2012BAI06B01)
ObjectiveTo evaluate the feasibility and safety of laparoscopy-assisted one-off complete radiofrequency ablation (RFA) for hepatocellular carcinoma (HCC) adjoining gallbladder.MethodsFive cases of HCC adjacent to different location of gallbladder were involved in present study. The tumor diameter ranged from 2.5 to 4.2cm. Laparoscopy-assisted radiofrequency ablation was performed without isolation or resection of gallbladder so as to maintain its anatomical integrity. The patients were followed up with the aid of ultrasonography and computed tomography postoperatively, at the same time the surviving quality was assessed.ResultsThree days after the operation, ultrasound examination showed that the gallbladder wall close to the ablated area was increased by 0.3-0.4cm, and the CT images showed that the density of gallbladder wall was increased. Six months after the operation, the contrast enhanced CT images showed that the gallbladder was intact and no high density area was observed in every patient, implying that the tumor was one-off ablated completely. All the patients lived a life with good quality during the follow-up period of 18-36 months.ConclusionLaparoscopy-assisted one stage radiofrequency ablation for hepatocellular carcinoma adjoining gallbladder with maintenance of the anatomical integrity of gallbladder is technically safe and feasible.
carcinoma, hepatocellular; radiofrequency ablation; laparoscopy
R735.7
A
0577-7402(2013)05-0359-04
2013-02-26;
2013-03-22)
(责任编辑:熊晓然)
国家科技支撑计划项目(2012BAI06B01)
姜凯,医学博士,副主任医师。主要从事肝癌的外科临床与基础研究工作以及射频消融的临床治疗
100853 北京 解放军总医院肝胆外科(姜凯、苏明、刘洋、赵向前、陈永卫、张文智、王敬、董家鸿、黄志强)
董家鸿,E-mail:dongjh301@163.com