不同骨癌痛动物模型拟合临床特征的研究!
2013-05-16于世英
桂 琦, 陈 豫, 于世英
华中科技大学同济医学院附属同济医院肿瘤科,武汉 430030
大部分癌症患者在疾病晚期会出现骨转移,而骨骼的转移往往会并发疼痛。骨转移疼痛经常伴有爆发性疼痛,临床上较为难治[1]。临床医师们进行了大量的骨转移疼痛的临床调查和临床治疗的试验研究[2]。关于骨癌痛的分子和病理机制以及治疗药物的基础研究也是近来疼痛领域的研究热点[3-5]。但目前骨癌痛基础研究中通常使用的动物模型(小鼠和大鼠)与临床骨癌痛在疾病类型、骨转移部位、骨癌痛部位以及疼痛特点方面是否相符,常用的几种动物模型与临床骨癌痛有无区别尚不清楚[6-7]。此外,尚缺乏原发性骨肿瘤疼痛的临床特点报道。
为了明确上述问题,本研究总结了Pubmed数据库里骨癌痛基础研究文献中动物模型的特点。同时进行了骨肿瘤疼痛的临床调查和进一步的原发性骨肿瘤疼痛的临床研究。
1 资料与方法
1.1 文献检索
在Pubmed数据库里采用“骨癌痛”和“动物模型”的关键词检索了从1999年到2012年5月所有以英文发表的文献。并对所有文献进行筛查,合并完全相同的骨癌痛动物模型文章,对最后入组的文章进行分类和归纳。
1.2 研究对象
采用回顾性研究,纳入2010年5月至2011年3月在同济医院肿瘤科住院的恶性肿瘤骨转移患者,以及2010年5月至2012年5月在该院就诊的原发骨肿瘤患者。入选标准要求患者有明确的病理学诊断和/或骨转移的诊断(ECT全身骨扫描的基础上进行可疑部位X线、CT或 MRI检查确诊)[8]。
1.3 研究方法和观察指标
研究的基本信息包括年龄、性别、Karnofsky身体状态评分(KPS)、原发肿瘤部位和骨转移部位,骨疼痛相关信息包括是否出现疼痛、出现疼痛的时间、疼痛部位、疼痛评分、疼痛类型及疼痛性质描述。疼痛评分采用11点数字化疼痛评分量表(NRS),其中0分为无疼痛或疼痛没有造成任何影响,10分是能想象的最痛感或生活完全被疼痛干扰,患者选择与承受的最重程度疼痛相应的分数。
1.4 统计方法
采用SPSS 12.0统计学软件进行数据处理分析。结果以平均数±标准差(±s)或中位数(范围)进行统计学描述。骨转移患者和原发骨肿瘤患者临床资料比较采用Wilcoxon秩和检验和卡方检验,以P<0.05为差异有统计学意义。
2 结果
2.1 骨癌痛动物模型特征
共入组了26篇骨癌痛动物模型文献,进行肿瘤种植部位、肿瘤细胞类型、骨癌痛类型和测痛指标的归纳,可分为7种不同模型,见表1。
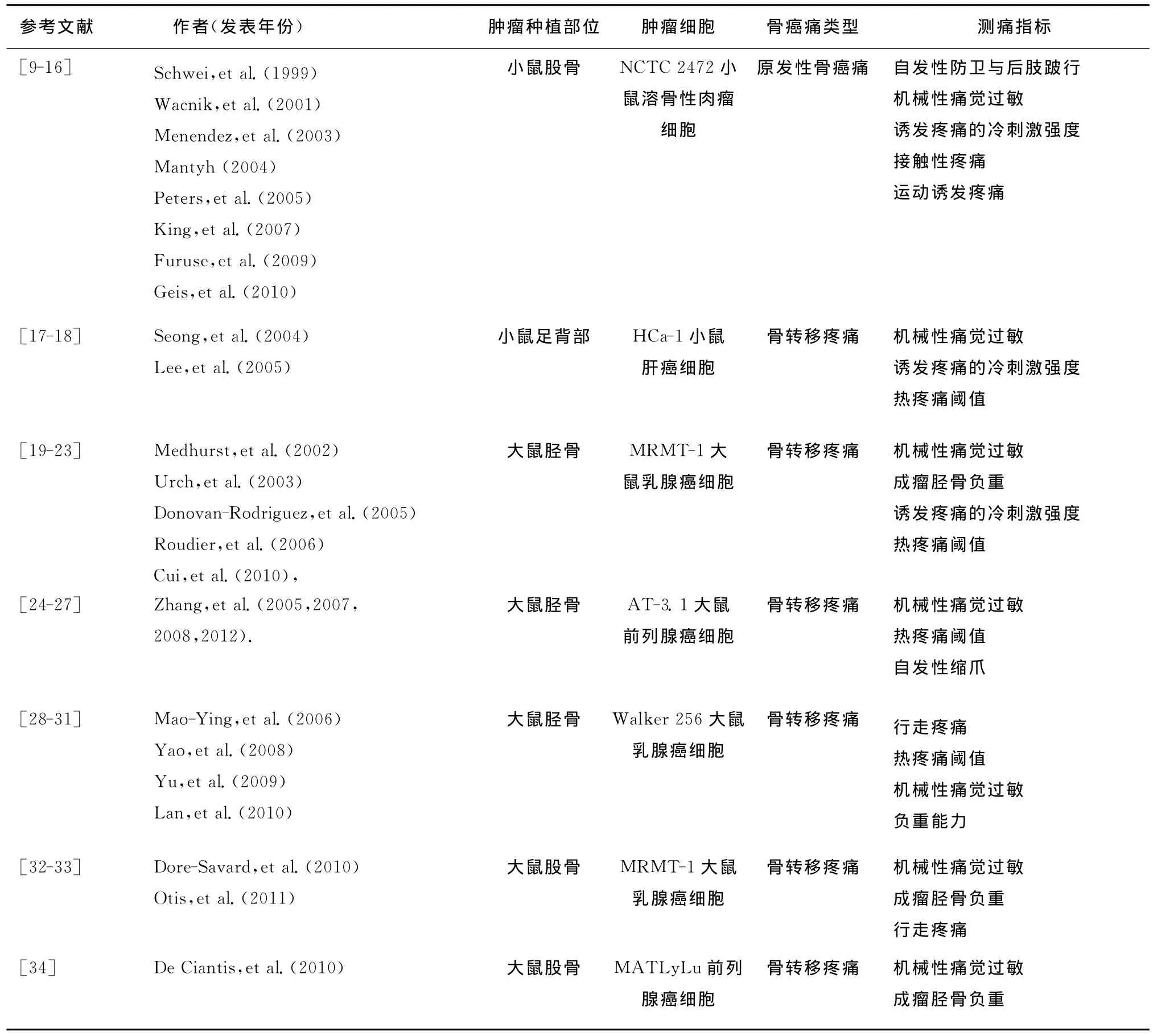
表1 骨癌痛动物模型文献总结Table 1 The literatures of animal models of bone cancer pain
2.2 骨肿瘤患者的一般资料
2010年5月至2011年3月在同济医院肿瘤科住院的骨转移瘤患者共入组81例,其中男性为42例,女性39例,中位年龄为53岁(24~78岁),中位KPS评分为70分(50~80分)。原发肿瘤部位分别为:肺(41例)、乳腺(14例)、前列腺(5例)、鼻咽(5例)、结直肠(4例)、胃(3例)、原发灶不明(6例)、其他(4例),其中1例患者同时患有乳腺癌与肺癌2种原发癌。原发肿瘤以肺癌和乳腺癌较多。
2.3 原发骨肿瘤与骨转移瘤疼痛特征比较
入组2010年5月至2012年5月在同济医院肿瘤科就诊的原发骨肿瘤患者12例,其中10例为骨肉瘤,2例为软骨肉瘤,将临床特征与以上2010年5月至2011年3月入组的81例骨转移瘤患者进行特征比较。原发骨肿瘤患者中位年龄为17岁(11~48岁),较骨转移瘤患者(中位年龄53岁,24~78岁)年龄小。原发骨肿瘤患者均出现了骨疼痛,且骨疼痛均出现在确诊骨肿瘤之前,而仅有63例骨转移瘤患者(77.8%)出现了骨疼痛,骨疼痛出现在确诊骨肿瘤之前的患者仅有46例(56.8%),余18例骨转移瘤患者未出现骨疼痛。在疼痛程度(NRS评分)分布上,原发骨疼痛与骨转移疼痛无明显区别(P=0.184)。在疼痛类型方面,二者有明显差异(P<0.05),原发性骨肿瘤以持续性疼痛为主,骨转移瘤出现了更多的爆发痛或伴有爆发痛(36/63,57.1%)。患者对疼痛描述中,骨转移瘤患者更多表现为在胀痛或钝痛的同时伴有针刺样、放电或烧灼样疼痛,或仅表现为针刺样、放电样或烧灼样疼痛,与疼痛分类的结果一致。见表2。

表2 原发骨肿瘤与骨转移瘤疼痛特征比较Table 2 Comparison of the pains originating from primary bone tumors and bone metastases
2.4 骨转移及出现骨转移疼痛部位
2010年5月至2011年3月入组的81例骨转移瘤患者中单发部位骨转移为23例,多发部位骨转移为58例。如图1所示,骨转移多发于胸椎(33例)、腰椎(29例)、肋骨 (26例)、骨盆骨(22例)和股骨(9例)。各骨转移部位出现骨转移疼痛的比例不同,其中75.0%(3/4)上肢转移出现疼痛,下肢为70.0%(7/10),腰部为69.0%(20/29),胸背部为57.8%(37/64),髋骶部为54.5%(12/22),颈部为33.3%(3/9)和头部为16.7%(1/6)。

图1 出现骨肿瘤及发生骨疼痛部位分布Fig.1 The distribution of bone tumors and bone cancer pain locations
3 讨论
骨癌痛分为原发骨肿瘤疼痛和骨转移性疼痛。原发骨肿瘤属于罕见疾病,在美国仅占所有癌症的不到0.2%[35]。本研究绝大部分骨肿瘤患者亦为骨转移瘤。目前针对骨癌痛治疗的临床研究大部分也特指骨转移性疼痛。而在动物模型的总结里不难发现,广泛应用于骨癌痛基础研究的小鼠模型绝大部分注射的是溶骨性肉瘤细胞,即模拟的仅仅为原发性骨肿瘤。
原发骨肿瘤与骨转移瘤的病理学机制目前仍不十分清楚,前者可能与某些特殊基因的改变相关,如p53基因突变可能与家族性肉瘤相关,而后者可能与肿瘤免疫以及骨的微环境相关[36-38]。在临床表现方面,本研究显示二者在发病年龄、疼痛是否为首发症状以及疼痛类型上均有显著差异,由于原发骨肿瘤中骨肉瘤患者居多(本研究中为10/12),而骨肉瘤多发于青少年,这与多发于中老年的骨转移瘤在发病年龄上有明显区别。本研究中的原发骨肿瘤患者均因骨疼痛就诊,即骨疼痛全部发生在疾病确诊之前,而在骨转移的患者中,近半数的患者确诊骨转移时并未出现骨疼痛。这提示二者在导致疼痛的机制上可能存在区别。而在疼痛类型方面,原发骨肿瘤多表现为持续性疼痛,少数伴有爆发痛(2/12),而骨转移瘤中表现为爆发痛或伴有爆发痛的患者比例明显升高(57.1%)。这在患者的疼痛描述中得到进一步验证,骨转移患者表现为针刺样、放电样或烧灼样疼痛或合并有上述疼痛的比例明显多于原发骨肿瘤患者。这些均提示以溶骨性骨肉瘤细胞注射造模的骨癌痛小鼠模型在模拟骨转移疼痛分子机制和爆发痛的治疗方面拟合度较差。
骨转移患者临床资料统计显示,骨转移部位发生骨转移疼痛的比例并不相同。其中四肢转移出现骨疼痛的比例大于腰部,腰部大于胸背部和髋骶部,颈部和头部相对而言最不易发生骨转移疼痛。这在一定程度上支持了目前常将四肢骨用于骨转移疼痛治疗的研究,但四肢骨是否适合作为骨转移疼痛的机制研究尚需在今后研究中进一步探讨。
在骨癌痛动物模型里,常用的注射部位为大鼠或小鼠的股骨或胫骨,以及少量足背部。而本研究中骨肿瘤疼痛患者资料统计显示,除了1例黑色素瘤骨转移至踝骨,并无转移至胫骨或足背部病例,在四肢的骨转移部位常见为近端骨(如股骨和肱骨),远端骨(如胫骨和尺桡骨)罕见。这与已发表的其他骨转移患者临床资料统计结果一致。其机制尚不清楚,可能与转移骨的血供及局部微环境相关。而对骨转移疼痛而言,胫骨模型可能对足底测痛(如von Frey纤丝测机械痛阈、热痛阈)较股骨模型更为敏感,这会不会对骨转移疼痛及治疗的结果判定造成一定的偏移误差,尚需要进一步的对照研究证实。
综上所述,并不是所有骨癌痛动物模型都能很好模拟临床资料。本研究显示注射转移性肿瘤细胞造模、股骨为成瘤点、测量方法中包含爆发痛测量的动物模型相对而言能够较好地模拟骨癌痛临床情况,其研究结果能较为有效地为临床研究和治疗提供参考。
[1] Coleman R E.Clinical features of metastatic bone disease and risk of skeletal morbidity[J].Clin Cancer Res,2006,12(20Pt 2):6243s-6249s.
[2] Zeppetella G.Impact and management of breakthrough pain in cancer[J].Curr Opin Support Palliat Care,2009,3(1):1-6.
[3] Gater A,Abetz-Webb L,Battersby C,et al.Pain in castrationresistant prostate cancer with bone metastases:aqualitative study[J].Health Qual Life Outcomes,2011,9:88-99.
[4] Laird B J,Walley J,Murray G D,et al.Characterization of cancer-induced bone pain:an exploratory study[J].Support Care Cancer,2011,19(9):1393-1401.
[5] 刘青,于世英,席青松,等 .恶性肿瘤骨转移住院患者生活质量及其影响因素现况调查[J].中华物理医学与康复杂志,2012,34(3):220-224.
[6] King T E,Pawar S C,Majuta L,et al.The role of alpha 6integrin in prostate cancer migration and bone pain in a novel xenograft model[J].PLoS One,2008,3(10):e3535.
[7] Shih M H,Kao S C,Wang W,et al.Spinal cord NMDA receptor-mediated activation of mammalian target of rapamycin is required for the development and maintenance of bone cancerinduced pain hypersensitivities in rats[J].J Pain,2012,13(4):338-349.
[8] 于世英 .恶性肿瘤骨转移的诊断与治疗[M].北京:中国协和医科大学出版社,2006.
[9] Schwei M J,Honore P,Rogers S D,et al.Neurochemical and cellular reorganization of the spinal cord in a murine model of bone cancer pain[J].J Neurosci,1999,19(24):10886-10897.
[10] Wacnik P W,Eikmeier L J,Ruggles T R,et al.Functional interactions between tumor and peripheral nerve:morphology,algogen identification,and behavioral characterization of a new murine model of cancer pain[J].J Neurosci,2001,21(23):9355-9366.
[11] Menendez L,Lastra A,Fresno M F,et al.Initial thermal heat hypoalgesia and delayed hyperalgesia in a murine model of bone cancer pain[J].Brain Res,2003,969(1/2):102-109.
[12] Mantyh P W.A mechanism-based understanding of bone cancer pain[J].Novartis Found Symp,2004,261:194-219,256-161.
[13] Peters C M,Ghilardi J R,Keyser C P,et al.Tumor-induced injury of primary afferent sensory nerve fibers in bone cancer pain[J].Exp Neurol,2005,193(1):85-100.
[14] King T,Vardanyan A,Majuta L,et al.Morphine treatment accelerates sarcoma-induced bone pain,bone loss,and spontaneous fracture in a murine model of bone cancer[J].Pain,2007,132(1/2):154-168.
[15] Furuse S,Kawamata T,Yamamoto J,et al.Reduction of bone cancer pain by activation of spinal cannabinoid receptor 1and its expression in the superficial dorsal horn of the spinal cord in a murine model of bone cancer pain[J].Anesthesiology,2009,111(1):173-186.
[16] Geis C,Graulich M,Wissmann A,et al.Evoked pain behavior and spinal glia activation is dependent on tumor necrosis factor receptor 1and 2in a mouse model of bone cancer pain[J].Neuroscience,2010,169(1):463-474.
[17] Seong J,Park H C,Kim J,et al.Radiation-induced alteration of pain-related signals in an animal model with bone invasion from cancer[J].Ann N Y Acad Sci,2004,1030:179-186.
[18] Lee B H,Seong J,Kim U J,et al.Behavioral characteristics of a mouse model of cancer pain[J].Yonsei Med J,2005,46(2):252-259.
[19] Medhurst S J,Walker K,Bowes M,et al.A rat model of bone cancer pain[J].Pain,2002,96(1/2):129-140.
[20] Urch C E,Donovan-Rodriguez T,Dickenson A H.Alterations in dorsal horn neurones in a rat model of cancer-induced bone pain[J].Pain,2003,106(3):347-356.
[21] Donovan-Rodriguez T,Dickenson A H,Urch C E.Gabapentin normalizes spinal neuronal responses that correlate with behavior in a rat model of cancer-induced bone pain[J].Anes-thesiology,2005,102(1):132-140.
[22] Roudier M P,Bain S D,Dougall W C.Effects of the RANKL inhibitor,osteoprotegerin,on the pain and histopathology of bone cancer in rats[J].Clin Exp Metastasis,2006,23(3/4):167-175.
[23] Cui J H,Kim W M,Lee H G,et al.Antinociceptive effect of intrathecal cannabinoid receptor agonist WIN 55,212-2in a rat bone tumor pain model[J].Neurosci Lett,2011,493(3):67-71.
[24] Zhang R X,Liu B,Wang L,et al.Spinal glial activation in a new rat model of bone cancer pain produced by prostate cancer cell inoculation of the tibia[J].Pain,2005,118(1/2):125-136.
[25] Zhang R X,Li A,Liu B,et al.Electroacupuncture attenuates bone cancer pain and inhibits spinal interleukin-1beta expression in a rat model[J].Anesth Analg,2007,105(5):1482-1488.
[26] Zhang R X,Li A,Liu B,et al.Electroacupuncture attenuates bone-cancer-induced hyperalgesia and inhibits spinal preprodynorphin expression in a rat model[J].Eur J Pain,2008,12(7):870-878.
[27] Zhang R,Lao L.A new rat model of bone cancer pain[J].Methods Mol Biol,2012,851:261-273.
[28] Mao-Ying Q L,Zhao J,Dong Z Q,et al.A rat model of bone cancer pain induced by intra-tibia inoculation of Walker 256 mammary gland carcinoma cells[J].Biochem Biophys Res Commun,2006,345(4):1292-1298.
[29] Yao M,Yang J P,Wang L N,et al.Feasibility of establishment of rat model of bone cancer pain by using Walker 256 cells culturedinvitroorinvivo[J].Zhonghua Yi Xue Za Zhi,2008,88(13):880-884.
[30] Yu S,Peng H D,Ju D W,et al.Mechanisms of treatment of cancer pain with a topical Chinese herbal formula in rats[J].Chin Med J(Engl),2009,122(17):2027-2031.
[31] Lan L S,Ping Y J,Na W L,et al.Down-regulation of Toll-like receptor 4gene expression by short interfering RNA attenuates bone cancer pain in a rat model[J].Mol Pain,2010,6:2-14.
[32] Dore-Savard L,Otis V,Belleville K,et al.Behavioral,medical imaging and histopathological features of a new rat model of bone cancer pain[J].PLoS One,2010,5(10):e13774.
[33] Otis V,Sarret P,Gendron L.Spinal activation of delta opioid receptors alleviates cancer-related bone pain[J].Neuroscience,2011,183:221-229.
[34] De Ciantis P D,Yashpal K,Henry J,et al.Characterization of a rat model of metastatic prostate cancer bone pain[J].J Pain Res,2010,3:213-221.
[35] Dorfman H D,Czerniak B.Bone cancers[J].Cancer,1995,75(1Suppl):203-210.
[36] McIntyre J F,Smith-Sorensen B,Friend S H,et al.Germline mutations of the p53tumor suppressor gene in children with osteosarcoma[J].J Clin Oncol,1994,12(5):925-930.
[37] Miller C W,Aslo A,Won A,et al.Alterations of the p53,Rb and MDM2genes in osteosarcoma[J].J Cancer Res Clin Oncol,1996,122(9):559-565.
[38] 邓春春,李晓燕,李柏华,等 .髓系来源抑制细胞及其在肿瘤免疫耐受中的作用[J].华中科技大学学报:医学版,2011,40(2):236-241.