辅助技术:终端用户与技术的桥梁
2011-02-27RenzoAndrichSerenellaBesio
Renzo Andrich,Serenella Besio
This document presents part of the research carried out during the Empowering Users Through Assistive Technology(EUSTAT)project,which studied the ways to render more efficient the use of Assistive Technologies by the user.
It is research which involved partners from different European countries and was coordinated in Italy,in particular by Renzo Andrich,director of Information Service and Aid Assessment(SIVA),Don C.Gnocchi Foundation,Milan,Italy,which is the most important Centre for Assistive Technologies in Italy and one of the most important in Europe.
The results of this research are representative of how Italy confronts the subject of the relationship between people and aids and they constitute an important key in understanding the care policies put into practice by the Italian Government.
Essential aids for the autonomy of disabled people in Italy are supplied free by the National Health System.But who decides what aids to provide?What goals does the state set itself by supplying aids for free? Through which processes can effective user empowerment be obtained?
The Italian care system relative to the free supply of aids to disabled people is based on three key points:
—The identification of a person's potential and needs to obtain the highest level of autonomy possible;
—The identification of efficient aids suitable to the particular and individual needs and potential of the person;
—The transfer of knowledge to the user;training,follow-up and the assessment of results reached;any necessary modification of the aid supplied in relation to the changing needs or capabilities of the person.
The whole process,from assessment of the person's needs to the choice of aid up to the follow up for the entire life of the person occurs within the scope of the rehabilitation path and responsibility for the choice of appropriate aids,as well as the obtainment of results,is entrusted to the rehabilitation doctor,employee of the National Health Service.It is the rehabilitation doctor who,assisted by a team of experts,plans an Individual Rehabilitation Project for each disabled person,within the framework of which aids are also prescribed(See previous article—Rehabilitation guidelines).In the Individual Rehabilitation Project the disabled person becomes as involved in the knowledge and choice of aid as in the training for that aid:the resources that the Government makes available for aids are managed through a process whereby choices are made by those who have specific competence with regards to identification of a person's potential and also with regards to the effective functionality and suitability of the chosen aid.
1 Introduction
1.1 Background
The main aim of the EUSTAT project is to develop training models and educational material that contribute to empower persons with disabilities and elderly people to make informed and effective choices of assistive technology.
Knowledge is one of the key factors for empowerment.The more the end-users are knowledgeable about assistive technology,the greater influence they can exert in the process of purchasing(or getting through a service delivery system)the right technology that compensate for their disabilities and help to achieve a more independent life,full participation in all aspects of their social life,and self determination.
The term"independent life",according to the most recent literature in the field,makes no reference to functional abilities:it does not mean"doing everything without any external human help".It is a dynamic concept continuously enriched by ongoing discussion at international level(see http://www.independentliving.org as Internet entry site).In general terms it is used to indicate that persons with disability take control over their lives,can access the same opportunities and face the same choices in everyday life that non-disabled persons take for granted.Depending on cultural contexts and individual expectations,that may include a variety of aspects like growing up in their families,going to the neighbourhood school,using the same bus,getting employment that is in line with their education and abilities,having equal access to the same services and establishments of social life,culture and leisure.Just like everyone else,persons with disabilities need to be in charge of their own lives,need to think and speak for themselves without interference from others.
In conjunction with other supports,like a barrier-free environment,personal assistance facilities etc.,assistive technology plays a substantial role in facilitating independent life.Having the end-users as main actors in the choice of the proper assistive device,as responsible,informed and demanding consumers,is consistent with the independent life approach,facilitates acceptance of technology,and can also result into better effectiveness and utility of technology.
In addition,providers of assistive technology can get a more comprehensive feed-back from their client,and learn useful elements for improving quality of products and services.It would not be wise to consider end-users simply as passive recipients of medical,technical,social and administrative services:they have the experience of disability,thus are in the position to evaluate aspects that only practical daily experience can reveal.
There are many arguments,both at individual an societal level,supporting the idea of promoting the empowerment of end-users.However,the achievement of this objective is not always so immediate.
There may be complex financial,organisational and cultural barriers in society;but even if we restrict our analysis to just the subject of this document,the transfer of the needed knowledge is not so simple.Identifying all aspects to be considered and addressed in the education of end-users was the challenge of this study.
First of all,the concept of end-users of assistive technology(AT)needs to be defined.In the context of this study,it refers primarily to people with disabilities and elderly people.However,it also encompassess their family members,helpers and personal assistants whenever assistive technology has an impact inside the whole primary network around the individual.The term end-user is adopted to distinguish them from other actors(e.g.rehabilitation professionals,assistive technology providers,etc.)who can be also considered"users"in a broader sense,in that they use AT as a tool for their professional activity in the field of disability.These will be identified in this paper as AT providers or AT advisers.
In the process leading from the expression of a need to the acquisition of AT by the individual end-user,a number of steps have to be overcome and several decision have to be taken.Some of them may extend also to the family or the primary network around the individual.
Knowledge helps to find the way through the various steps,and supports decisions.The needed knowledge may be in the hands of the concerned person,may be distributed inside the primary network,or may be sought from external advisers.
There is no fixed recipe where the specific component of knowledge has to be:factors related to age,culture,pathology and available social services have certainly an influence on the extent and on the deepness of technical information that can be transferred directly to the end-user.On the other hand,it is not necessary for the end-user to be a technical specialist in AT:rehabilitation professionals and technology providers are expected to be such.There are people who may be eager to achieve full command of technical topics,but the majority of end-users may be quite satisfied by just a basic background on the AT that can be useful with respect to their disability,provided they have the possibility to resort to qualified professional or peer advisers when needed.Again,empowerment does not mean"doing everything alone",but being actor and protagonist of the process.This may sometimes involve also acting in partnership with professionals,deciding to follow their advice,finding the most efficient compromise in case of unavoidable financial barriers:for sure it does not mean to completely depend on the decision of the professionals.
The guiding idea of this study is that each end-user should be provided with the maximum amount of sustainable and useful knowledge.This sentence may be smart,but opens a question around what is"sustainable and useful"for each individual and who is going to decide that.If the answer had been simple,there would be no reason for this study.In fact an ultimate answer doesn't seem possible.The transmission of knowledge is a dynamic process;it never ends because persons change in response to knowledge:new horizons opens,new needs arise,new challenges appear.So it cannot be solved through the provision of a simple set of information and notions.It requires an educational approach assisting the persons in their changes.
To design and carry out suitable educational processes,a number of critical factors need to be identified and addressed.The scope of this study covers first aspect,the identification of critical factors.Another study within the EUSTAT project(Guidelines for courses for user empowerment in relation to AT)will face the challenge of addressing critical factors.
In the following chapters a great deal of aspects will be analysed and weighted with regards to their possible influence on the process of user education in relation to AT.The main focus will be mainly the impact on the individual(personal growth towards autonomous life,copying better with disability in daily life etc.),although also some societal impacts can be expected as a direct consequence(e.g.exploiting the expertise that disabled and elderly persons can offer to other persons with disabilities,to rehabilitation professionals,manufacturers and providers as field-evaluators,etc.).
1.2 Basic Concepts
1.2.1 First keyword:Autonomy
The ultimate goal of assistive technology is often described in terms of social keywords like quality of life,social integration,independent living.However,these achievement should be seen as a result of a number of factors and circumstances,one of them being AT.Examples of other factors are environmental accessibility,personal assistance,social provisions,affirmative legislation(e.g.anti-discrimination laws as the American with Disabilities Act,1990),acceptance of diversity in the community,financial support,and so on.In the ongoing discussion around the concept of independent living,somebody argues that a person with disability who has deep knowledge of AT and full ability to make the best choice,but avails no financial mean,no funding,no public service delivery system respectful of his or her choice,very hardly could pursue a project of independent life.
On the other hand,the role played by the individual should not be underestimated in favour of just societal factors.Achievements in quality of life,social integration and self determination require the full participation of the individual person with disability,as main agent in defining his or her goals and projects,and main protagonist in carrying out actions for solution.Like a mechanic watch requires that all cogwheels be in place,but works only if the spring is loaded,likewise a"spring"is needed inside the person,that includes motivation,ability to identify and formulate needs,decision on goals,willingness to pursue projects.This"spring"will be described here with the term autonomy.While compensating for impairments or disabilities or removing handicapping barriers(effectiveness in doing that is easily measurable even by external observation),it is the authors'belief that the more AT is consistent with a project of autonomy,the more it will be beneficial and useful for the individual.
Within the professional community it is sometimes argued that a percentage of people with a disability is not able to be really active in the choice of their assistive technology:this may depend on factors like age,cultural level,psychological barriers towards the acceptance of an assistive device during the early onset of disability,unfamiliarity with technology,etc.However,it is not always clear to what extent such difficulty is a cause or rather a result of traditional organisation models in the provision of rehabilitation services.Difficulties should not be underestimated:it may be true that many disabled persons or elderly with a disability will be unwilling to act as"full partners"in the choice of AT;but it is also true that a lot can be done in promoting autonomy and thus facilitating their empowerment.
The concept of autonomy is not restricted to persons with full cognitive ability.Even in case of persons in the need of various kinds of support due to intellectual impairment,cognitive limitations,ageing,frailty,disease etc.,they can be led to be autonomous with respect to their expectations(even in this case AT exists that can help achieve such goal).
In the following a semantic clarification of the notion of autonomy is attempted,following its historical evolution.Such notion has changed greatly over time and is often described very differently by various author.
From a historical point of view,the concept and the importance of autonomy for the disabled arises from a social perspective of the handicap issue.
In a paper on this theme,V.Finkelstein(Finkelstein,1980)suggests a radical but interesting thought,according to which"disability is an oppressive social relationship"and he argues that"those who carry out research or social analysis of necessity participate in the disabling social relationship".He states that in our society almost every aspect of the life of a person who is disabled has its counterpart in a"profession"or voluntary organisation,and this resulted into the attitude that the disabled individual is obviously particularly dependent upon others for help.One result of that was the image of disabled people as passive objects of research and help.
He identifies three phases in the social and historical process of creating and"eliminating"handicaps.
First,since the beginning of the modern era,although people with physical impairments have always been present as"cripples",they were not segregated from society for the special treatments and services which we recognise today.Crippled people were clustered at the bottom end of the social scale together with other social strata;but they were socially active people,responsible for their actions.
The second phase was inaugurated with the growth of hospital-based medicine and the creation of large asylums:institutions provided the physical means for segregating disabled people from their communities.
Here,the characteristic attitude was to view disabled people as suffering from personal tragedies,unable to care for themselves and consequently in need of care and protection.At the same time the success of professional medical and para-medical help has contributed to the increasing numbers of disabled people able to achieve social independence and who thus question professional'domination'of their lives.
The third phase can be viewed as just beginning,setting the context for the generation of new attitudes.The move towards increasing independence in the community marks this change.For sure a major impetus for this development has been provided by the latest advancements in assistive technology:think e.g.what the appearance of the market of the first environmental control systems meant in term of increasing independence of the disabled and elderly persons.
Phase three heralds the"elimination"of handicap.
Within a social perspective of the concept of autonomy,some authors(Engelhardt,1992)consider a person as autonomous on one condition:that he or she can manage all mental faculties,acts as a rational person,without being subjected to external pressures.A weakness of this assumption is that it excludes anybody who experiences cognitive limitations(due to dementia,mental retardation,head injury etc.).
A different idea of autonomy comes from a more global approach to the person which emphasises social and relational aspects.This was due to a large,stable change in thoughts which occurred in the 40s,thanks to many authors from various disciplines who stressed the importance of the cultural and social environment.The Russian psychologist L.Vygotskij(whose works have been published in the western world in the seventies:Vygotskij 1978),underlined the role of the social context and the social actors in the individual's cognitive development.G.Bateson(Bateson 1972 and 1979)proposed the idea of the social construction of meanings and studied human communication as a circular process and not a linear one.This corresponds,in the world of medicine,to the great idea that it is the relationship between nature and culture that builds a person and cures him/her which brought to widespread ideas about the so-called"welfare-medicine"whose slogan was"from cure to care".
One of the pioneers in introducing such ideas in the domain of rehabilitation was the Italian physician A.Milani Comparetti(Milani Comparetti 1960,1981 and 1982),breaking the ground for the first experience of school integration of disabled children to be carried out in the world at a nation-wide scale(the Italian 1975 law on elimination of special schools).
Within the HELIOS I(1988-91)and HELIOS II(1992-96)(the Action Programmes of the European Commission to promote equal opportunities and the integration of disabled people)such global approach was further developed.Autonomy was considered as a dynamic process which includes the individual point of view,the family's point of view,the immediate outer circle,and society.
Consequently,four domains of autonomy were described:
1)body and mind,
2)home and family,
3)community,and
4)society.
Consistent with this approach is the relational definition of autonomy as ability to plan one's own life,to enter into relation with the others and,together with them,to actively participate in the construction of society(Andrich and Porqueddu,1990).This definition establishes a kind of equation like autonomy=relation,which in turn includes three types of relations:with self,with others,and with the environment.It is apparent that such concept applies to any person,independently on their health or physical or mental status.An able-bodied person may be non-autonomous if he or she experiences difficulties in one or more domains of relation;conversely a person with severe disabilities who depends heavily on personal assistance may feel comfortable at all of the above relational levels.The onset of a disability brings about a change in life;so in order to resume a situation of autonomy he or she needs a personal restructuring,that means to build a new relation with self,with the others and with the environment.In this view,AT is instrumental to such goal:it is a tool for relation.The following scheme synthesises the concept.

1.2.2 Second keyword:Assistive Technology
There are at least two different perspectives,technological and a social/cultural,from which AT can be looked at.Both are dynamic and evolved over time,and should be seen as integrated in a modern approach to AT.
The international ISO-9999 standard(along with the corresponding European standard EN 29999)offers a technical definition of assistive technology:any product,instrument,equipment or technical system used by a disabled or elderly person,made specially or existing on the market,aimed to prevent,compensate,relieve or neutralise the deficiency,the inability or the handicap.It is a device-oriented definition,placed before the well-known ISO/EN classification of assistive devices that is used by almost all existing databases in the field.
A.Cook and S.Hussey(Cook and Hussey,1995)suggest a broader approach,stating that strategies,practices and services don't have to be separated from technology.In that sense,they define AT as a broad range of devices,technical aids,strategies,services,practices,with the main objective of improving the quality of life of the disabled and the elderly.
The European TIDE/HEART study looks at AT from the perspective of its outcome,by saying that the ultimate objective of AT is to contribute to the effective enhancement of the lives of people with disabilities and elderly people,helping to overcome and solve their functional problems,reducing dependence on others,and contributing to the integration into their families and society......It also suggests that assistive technology cannot be considered as a specific type of technology in itself,but as the implementation of a particular,and generally well-known,technology(e.g.Electronics,telecommunications,informatics etc.)for a clearly defined applica-tion by people with disabilities.By this sentence HEART means that not always AT coincides with a technological device specially developed for disabled persons(e.g.special interfaces),but often results from the assembly of consolidated technologies that are implemented according to the user needs.
While it is quite clear that AT yields enormous potential for the benefit of people with disability,it is not yet clear how to measure its impact on both the individual and society,so as to be able to make comparison between the impact of different kinds of technologies.When investigating the issue of AT outcomes,a report of the European TIDE/CERTAIN Study(Lorentsen and Hem,1995)offered an interesting insight of the domains where AT has an impact with respect to the expectations of the individual:
1)the inner relations,
2)the activities of daily life,and
3)the outer relations:
1.Inner relations relate to self esteem,self confidence,coping and acceptance of disability.
It reflects the individual state of comfort,satisfaction,safety,contentment.Pain,discomfort,anxiety,insecurity and destructive elements are factorsthat of course should be eliminated.
2.Activities of daily life includes all tasks/activities in all facets of life.
These have to be identified by each individual user according to one's own preferences,priorities and values.
3.Outer relations concern social aspects,social integration and social networking,again defined on an individual basis according to one's own priorities.
The authors also suggest that the expectations of other actors should be investigated,namely
1)the family or primary network,
2)the professionals and
3)the community.
In the whole,this view looks interesting in the context of this papers,being it consistent with the relational definition of autonomy that is given in the previouschapter.
Some authors point out that AT might hide some risks and even restrain autonomy(Brunelles,1992).Based on accounts of occupational therapists and of disabled people about the design,utilisation and perceptions of AT,Brunelles emphasises the dangers of looking at AT just as a compensatory technical object,without considering the project of life of the individual user.He support his comments with cases where aspects related to the return at home after discharge from hospital were underestimated,leading to failure of AT.
The public image of AT as offered by mass-media often reflects the level of disability awareness in the community.On the one hand,sometimes the assistive device is presented as negative symbol of the disabled person's confinement,putting emphasis on the impairment(medical view)and thus reducing the image of the disabled person to his/her limits.This image has been often used by associations working in the field of disability to raise emotions for improving fund raising(financial view).On the other hand,there are good example of AT(even in commercial advertisements)presented as a tool for independence and relation,where users appear to be engaged in activities together with other non-disabled people,on an equal foot.
Conveying a correct and positive image of AT yields a great educational value for the community,and can give a powerful contribution to public awareness and acceptance of disability.
1.2.3 The third keyword:Critical Factors
Success or failure of AT depends on several factors.There are factors related to the disabling impairment,to the end-user's situation,to the role of intermediaries,to the environment,to the attitude and knowledge of the surrounding helpers and professionals.The individual medical and psycho-social condition,the personal past experience in AT,the person's current expectations may generate a variety of perceptions of AT in relation to the problems to be solved.Clarifying these processes is substantial to understand to what extent knowledge can contribute to empower end-users to reach the needed autonomy so as to make responsible,effective and useful choices.The objective of this study is to identify,classify and describe the body of AT knowledge to be transferred to the end-users:now,being the concept of autonomy so dependent on the individual,it is clear that the process of knowledge transfer should be tailored to the needs,personality and environment of each individual.The"critical factors"analysed in the following chapters are the keys to understanding how such a process can be customised.
The term"critical factors"refers to all those aspects influencing the transfer of knowledge on Assistive Technology to the end-users,and in turn influencing the ability of the person with a disability and/or the elderly to make informed,effective and satisfactory choices.There may be critical factors that have a negative influence,others that yield a positive influence,others that may act positively or negatively when cross-related with other critical factors.The adjective"critical"is not used as a synonym of"positive"or"negative";it just means deserving careful consideration.
2 End-users And Tecnology
2.1 The Users Demand
2.1.1 User involvement
In a report dealing with AT education of professionals,the TIDE/HEART study recommends that"......The first characteristic of an European curriculum is user focus.User focus means that in all training programmes and courses in assistive technology,the ultimate objective is to enable the elderly and the people with disabilities to reach the optimum level of capability by,for instance,reducing the demands of the environment through assistive devices.User focus also means that all demands of different groups of disabled and elderly should be taken in account when planning training in assistive technology.Users should also participate in training programmes and courses giving lectures,and sharing their knowledge and experiences with the participants......"(HEART E.2.1,1994).As yet it seems that this seldom happens in current professional education programmes;however,the issue of user involvement is more and more taking shape in research findings and policy discussion.The above recommendation is one of the many examples of statements that point out ways to make such involvement concrete.
The HELIOS II thematic group 6("Elimination of technical barriers",in the Network of Social Integration and Independent Living")discussed extensively the role of technological aids in promoting autonomy.Several report(HELIOS II,1994,1995,1996)pointed out that the end-users should take active part in all stages of the ideal circuit they sought to identify,like manufacturing,marketing,distribution of information.They also stated that the involvement of users in the process should not be limited to technical aspects,it should also extend to educational,social,financial and legal aspects.
However,they recognised that this cannot be done by simply having a random person with disabilities consulted,but requires that the users are educated to be active partners.Paramount to this purpose is to provide independent and objective information or advice on assistive technology,but also to increase one's awareness and consciousness about autonomy and AT.In other words information is substantial,but on condition that the person undertakes a personal process of change.
However,the user influence is an interactive process that requires not only the users prepared to do that.J.Wesemann(DG V and DG XIII,1995)writes"......there is often too little interaction between scientists and consumers.The development of prototypes must be tested with the help of the disabled people for whom they are meant,to make sure that the final products can be used properly".Consistent with this thought,one year later the USERfit methodology was published by the TIDE/USER project of the European Commission providing concrete models and tools for users involvement in products development.It greatly contributed to spread out the concept of user centred design for AT(Poulson et al.,1996).
Some years before,a proposal of L.A.Edwards(Edwards,1992)appeared on the Internet in which he coined the expression prosumer approach from the two words producer and consumer,mainly referring to the production and utilisation of information and thoughts.
He wanted to stress the need to spread a new way of thinking about the roles and relationships in the rehabilitation field:the right to self-determination of the disabled must also concern their participation in the entire rehabilitation process,including the use and the production of knowledge and products,and their involvement in the research projects themselves.
Again Line E the HEART study depicts the involvement of end-users in professionals educational curricula as"......guest speaker or lecturer"for case studies and demonstrations.So the consumer's knowledge and experience should be utilised to make the technological solutions acceptable to consumers and tailored to their needs.Other professionals stress the involvement of consumers in training,like showing students how they use technologies,and the pros and cons of the technologies"(HEART Line E.2.1.,1994).
Many other ideas can be found in literature about models of user involvement at various levels,like design of policies and programmes,feed-back methods embedded in products development of products,participation in the standardisation process.Looking at findings of a number of local pilot projects in the European Union,the HELIOSthematic Group observed that:
·the disabled and the elderly are able to draw the attention to problems that are often hidden to the eyes of professionals,so the contribution of experts with disabilities improves dramatically the process of identification of needs and requirements;
·the influence of users leads to improved standards;
·user involvement should constitute a systematic part of the rehabilitation process,in order to improve its effectiveness.
A closely related issue is the user involvement in service delivery of assistive technology,on which topic Line C(Service Delivery systems)of the HEART study(HEART C.5.1.,1994)worked out a number of recommendations:
·users are the best judges of products and services directed to them;
·a good service delivery system is designed in a way that empowers users to make their own choices;
·good service needs feedback and user involvement.
·the rights of disabled persons to access appropriate assistive technology should be ensured through adequate legislation and financial support schemes;
·financial resources should be allocated to facilitate users influence at various levels(committees,reference groups etc.);
In conclusion,as underlined by HELIOS II,three main keywords can be identified as component of user involvement:choice,control and feed-back.
Interesting indicators of the relevance of the user involvement issue can be drawn from studies on assistive technology abandonment.Low utilisation and early abandonment(abandonment before the normal technical life-cycle of the device)may suggest that the technology provided was poor or wrong,or for some reason resulted ineffective,useless or unsatisfactory for the client.In such a study carried out in the United States over a sample of 200 users(Phillips and Zhao,1993),four factors were identified as the main reasons for abandonment of assistive technologies:
1)failure of providers to take consumer's opinions into account,
2)easy device procurement,
3)poor device performance and
4)changes in consumer needs or priorities.
These findings suggest that technology-related policies and services need to emphasise consumer involvement and understanding of longterm needs of consumers.If not,there is high risk that the needs of people are not properly met,and public funds are wasted.
2.1.2 Identification of the users'needs
A clear understanding of needs is the first step to start any user focused process.Identifying user needs means searching for satisfied or unsatisfied needs,at both individual or collective level(Conte,1984).
To ensure that this is done appropriately in all relevant domains(lifestyle,products,services,initiatives etc.),a consistent approach should be found and methods should be designed.
It seems that the needs identification is often the weak point of several studies,which overcome this problem by simplistic assumptions(e.g.that a real need corresponds to the immediate personal perception of the need;or,conversely,a pre-defined table of needs that all people with disabilities are supposed to have).
A study done by DHDO,Développement des Hommes et Des Organisations(Conte,1984)explored this issue,taking into account the differences among people with motor,visual or hearing impairments,and elderly people.The questions were about psychological approach,daily difficulties,limitations to autonomy,human resources available,expectations etc.It found that many surveys in the field lack attention to user needs and assumption made by service planners often lack scientific ground.They also highlighted that needs of elderly people living in an institution appear quite different with respect to those living at home.As a background for a further study,CTNERHI(Observatoire Régional de Santéd'Ile de France and CTNERHI,1985)carried out a survey in two French departments about the needs for assistive equipment for adult disabled people.The results were almost total absence of information about disabled people,their numbers,the nature of their disability and the related needs.
In another survey carried out in Norway(Lorentsen and Hem,1995)through brainstorming sessions with users,family members,user organisations and professionals,the issue of correspondence between AT and the user needs was discussed on the basis of the participants'experience.Questions were asked like:"What are the critical factors in providing assistive technology?","What characterises a good solution and a good provision process?","What expectations do you have concerning an assistive technology solution?"etc.It was found that the outcome of assistive technology depends not only on factors related to the individual disability,but also on the performance of the assistive devices,on the processes and the methods through which the national service delivery system relate to individual users,on the coherence of AT with the overall habilitation and rehabilitation strategies.So fixed tables like disability—need—solution cannot be established a priori,all the above factors should be considered case by case(depending on the person and social setting)without any implicit hierarchy.
Only recently the issue of users-needs analysis with respect to AT was raised in rehabilitation science studies,especially in conjunction with AT outcome analysis.Instruments have been designed like e.g.the"Matching Persons and Technology"(Scherer 1994)for assisting technical aids advisers to better identify(in partnership with their client)the areas of individual needs that could be solved through AT,and the individual predisposition to adopt technological solutions.
Such issue should be central in the context of the EUSTAT project,being it quite obvious that any initiative of end-users education should respond primarily to their needs,and not to the needs of other actors in the field.
2.1.3 Assessment of user needs
In current rehabilitation practice,especially in occupational therapy,there are several approaches to the assessment of clients'needs with respect to daily life functioning.Several instruments have been developed to measure the outcomes of rehabilitation processes,although none of them still seem to be sufficiently responsive to AT(Andrich and Ferrario,1996).Such assessment instruments can help a lot to explore the extension of needs,but they often tell little about the individual perception,priority,dynamics and emergence of needs.One need that is such for the majority of people may be not felt as a need by an individual.In other words each need is weighted differently by various individuals.
For the EUSTAT purpose it seems important to distinguish between two possible approaches in the analysis of end-users'needs.The first can be defined as an external observer analysis,the second as an internal/systemic analysis.The choice of either approach yields important consequences for the design of educational initiatives for end-users.
The first approach is based on"inventories"or"compendia"of needs,designed on the basis of studies carried out over populations of people with disabilities.In this manner problems or needs are classified and thus can be treated as objective(and sometimes measurable)data.
Classifications exist with respect to the impairment,disability and handicap dimensions(see WHO definition in chapter 1.2.1)as well to other medical or psychological dimensions(rehabilitation medicine instruments).Following this approach,the handicap(or social disadvantage)dimension seems the most useful for the EUSTAT purpose,since in the end-user view it is clearly related to technological support.Since handicap can be seen as generated by:
·disturbance of the ability to act in the environment(dependence or inability to carry out a certain number of fundamental acts,due to impairments or disability,and not due to choice);
·a physical or human environment generating difficulties or impossibilities for disabled or elderly people to carry out activities related to those fundamental needs;
This involves thinking about:
·means of compensation that take charge of dependence(human help)or lessen it(technical devices);
· means of adapting and humanising the environment through better design,technical standards and normative conceptions.
Although useful as a conceptual framework and for providing an overall picture of the needs,the classificatory approach doen not seem sufficient for the understanding of the individual needs.Every person is different from the other,so the standard disabled person or the standard elderly having a standard need as felt by the majority of their peers does not exist anywhere.One indicator of that is the different response by each person to the same problem,in terms of motivation to act or resistance to change.
For the EUSTAT objectives the second approach is preferred.This does not attempt to assess needs by external observation.It relies on the supposed ability of the individual(and the system around him or her)to define and elaborate them.It is based on a systemic vision,where the system composed of the person and(where applicable)his or her primary network(spouse,family etc.)is helped to identify,express and weight needs(Hierbert and Smallwood,1987).Such approach is often used in counselling practice,but seems also interesting in an educational context(training end-users to express needs and set goals).Details are given below.
2.1.4 The expression of needs
According to a constructivist view,the need(in terms of something to be satisfied or a problem to be solved)is not placed in the nature,as an objective attribute of the world around the person.It is an individual or social construction of reality.Something is perceived as a need when a gap is felt between the present situation and a possible"better"situation,and there is a feeling that some actions could be done to move towards that"better"status.
The expression of a need is therefore a multidimensional event that integrates three distinct,but closely bound,perceptual data:the representation of a present situation,the representation of an expected situation,and a perspective of action(Burgeois,1991):

Each of the above three"poles"interact with each other.The perception of the present situation is influenced by the aspirations and the expectations of which the individual is the holder.Inversely,his or her aspirations are conditioned extensively by the life experiences the individual has now.The perspective of action concerns the ideas on the means that can transform the present situation into the expected one:these are substantially determined by his or her representation of the present situation and of the expected situation.Despite such three poles are always interacting,this doesn't mean that each of these representations is necessarily conscious or explicit nor that it has to be necessarily elaborated at the same time.It is sufficient that at least one of the three poles is salient in the perceptual field.
For example,one individual may at first express a need solely in terms of a problem to be solved,even though,at that time,he/she is unable to express the aspirations which are behind his/her mental construction of the present reality,nor yields he/she any ideas of means of action that meet such unexpressed aspirations.Similarly,some persons may express a need at first under the form of desires,of expectations,of aspirations to achieve,even if,at that time,they do not make any analysis of the present situation and have just some vague intuition that something could be done.In other cases the salient pole could at first be only a perspective of action without discerning what the present situation is like nor the achievements that can be expected.
In this perspective,the analysis of needs is nothing else than a process which leads the end-user to solve the three poles in interaction.At each point in time,the salient pole(s)represents the"entrance door"of the needs analysis.According to this approach,the transfer of knowledge should not be a mere transmission of notions,but an injection of ability to
1)better clarify each of the three poles,and
2)better solve their interaction.
Under this assumption it is possible to say that it facilitates empowerment.

Information and knowledge help each user to produce new mental constructions and therefore new expressions of needs.The clarification of the three poles will thus culminate in a point when the user feels he or she has produced the most applicable representations.So the expression of needs is person-specific,is different from one user to another;different users with different psychological attitudes,life experience,social status and contexts may feel comfortable with quite different choices with respect to the same situation they may encounter in daily life,at school,at work,in social relationship.
Knowledge can be injected from the outside through a lot of means:information on the mass-media,visiting an exhibition,advice from a professional of by a peer,informal information from others,role modelling(seeing other people with disabilities living a independent and resourceful life),etc.
The EUSTAT study will look at formal education as a means to transfer knowledge.
2.1.5 Role of the primary network around the individual
However,knowledge can be generated also within the primary network.It should be observed that very often the members of the primary network have an influence and a role in the process of clarification of the three poles.There are aspects of the individual life project that can be hardly separated from the family life project;for instance,there may be a range of expectations originating from the relationship with the spouse,who may have in turn other needs and aspiration which are then shared with the partner.The introduction of AT in a family has an impact at various levels and(maybe with the exception of strictly body-related technology)it may require personal changes in other family members.It may also require modifications in the organisation of personal assistance,and thus a change in attitudes and habits of personal assistants.So the analysis of the end-users'needs cannot ignore the point of view of the helpers,and their influence in the expression of needs.
Again resorting to a systemic view,all the"system"composed of the individual and his or her primary network should be looked at in this analysis.A kind of"subsidiarity principle"could be defined:since such"system"is supposed to have internal resources to find solutions to its needs and problems,external actions should aim at
1)empower it to better understand needs,set goals,make projects,take good decisions,and
2)set up the societal conditions that allow such decisions to be actually implemented.
Internal to the system,the role and the weight of the various members with respect to disability problems and assistive technology is different from one case to another,and can even vary in the time.There are cases in which the individual with disability is in fact the only and unique person dealing with such topics,with no influence from others;there are cases where he or she,on own choice,shares these aspects of life with others;cases where a wider group is involved;and even cases where the real end-users of AT are in fact the helpers.
The term"helpers"refers to those members of the network who provide the practical help in assistance or in carrying out the activities of daily life.Depending on case these people can be:
·family members,like parents,partner,children,etc.;· friends:who come occasionally or regularly to help;·personal assistant:persons from the outside,paid for this help.
In other words,the clarification of the poles is a circular process by which the user reviews his/her representation of needs,sometimes together with other members of his/her network;and this clarification can be enhanced by formal or informal information.
2.2 Processes of knowledge transfer
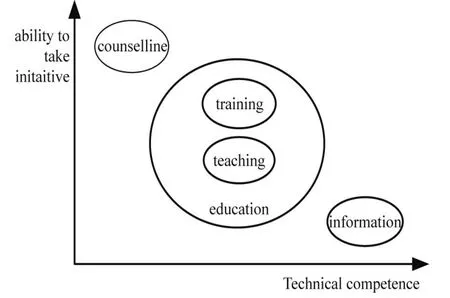
Five different processes have been identified in the knowledge transfer in the field of AT:counselling,training,teaching,information,awareness campaigns.
1.Counselling can be defined as the process through which a person,on the basis of his/her professional expertise(professional counselling)or own personal experience of a similar situation(peer counselling),helps the individual end-user to make choices and take initiatives by giving information,helping to better understand one's own situation,favouring motivation.Professional counselling is now a well-studied technique in the field of psychology where the relationship between the actors is established as well as the objectives and the subjects'roles.
2.Training is first the process through which a trainer teaches an individual trainee or a group of trainees practical knowledge about specific categories of Assistive Technology.Training also has a second and more complex meaning,which concerns the special kind of educational activities that can be organised by an industry or a business in order to modify its employees'competence and attitudes towards any aspect of work.Some of the educational activities set up by organisations in the field of disability to help or favour the participants'empowerment towards autonomy can have the character of a training.
3.Teaching is the process through which a higher level of understanding,competence and problem-solving ability is provided to a group of users.Teaching activities may be less or more complex in content,extent,duration,organisation and may be carried out through lessons,seminars,conferences,courses......
As explained above,within the EUSTAT study we will refer to the two processes with the more comprehensive term education,except when the situation needs a more detailed reference.
4.Information is the process through which notions pertaining to the field are given to users.Information is generally addressed to a large audience aiming at increasing general competence.
EUSTAT 33.
5.Awareness campaign is the process through which attention is raised on specific issues with the intention of shaping the attitude towards.
For effective empowerment all five processes above should take place.AT users(persons with disabilities,elderly and their helpers)may need education,training,information or counselling at different times and for different purposes.
Awareness campaigns,although important,will be not considered further in the EUSTAT study.It can be seen as a background process addresses towards large and undetermined population rather than the individual end-users;awareness campaigns may be needed to remove prejudice or bring to light neglected opportunities to pave the way for other kinds of empowerment initiatives.
Concerning their main aim,any of the remaining four processes(counselling,training,teaching,information)can be"positioned"differently with regard to the stress it puts on supporting initiatives or providing technical competence to the end-users.
In the following diagram the four processes are illustrated as regards their main objective.The two opposite poles are occupied by information and counselling.Information plays a great role in the notions and competence dissemination and isn't directly addressed to raising the individual's ability to take initiative;counselling is a well defined set of actions aiming at changing something in a person's life.
Education is here the mid process,with a balanced interest in both objectives(raising competence and initiative),having training a little stronger accent towards initiative,because of its more practical and concrete structure(basis).
......
Acknowledgements
This study is the result of a co-operative effort carried out by the researchers of the
EUSTATConsortium:
SIVA(co-ordinating contractor)
Fondazione Pro Juventute Don Carlo Gnocchi,Milano Italy
Mr.Renzo Andrich(project leader)
Ms.Serenella Besio
ANLH(partner)
Association Nationale pour le Logement des personnes handicapées,Bruxelles Belgium
Mr.Cleon Angelo
Ms.Anne-Catherine Jooris
Mr.Franco Cortesi
GIHP(partner)
Groupement pour l'insertion des personnes handicapees physiques,Bordeaux,France
Mr.Christian Berard
DC(partner)
Danish Centre for Technical Aids for Rehabilitation and education,Taastrup Danmark
Ms.Suzette Thegler
Ms.Lilly Jensen
CAPS(partner)
Centro Analise e Procesamento de Sinais,Instituto Superior Tecnico,Lisboa Portugal
Mr.Luis Azevedo
Ms.Margarida Nunes
PRIS(partner)
Centro Studi Prisma,Belluno Italy
Mr.Beppe Porqueddu
Mr.Angelo Paganin
Main contributors to the compilation of this documents were Anne-Catherine Jooris,Cleon Angelo,Franco Cortesi,Renzo Andrich and Serenella Besio.Christian Berard,Luis Azevedo and Margarida Nunes also contributed in several sections of the document.All other partners provided valuable input and views,and helped to complete the literature review.
Reference
ALLIANCE FOR TECHNOLOGY ACCESS.Computer resources for people with disabilities.Hunter House Publishing,1994.
ANDRICH R.Ausili per l'autonomia.Milano:Pro Juventute,1988.
ANDRICH R,FERRARIO M.Cost outcome analysis for assistive technology:case studies.European Commission,Deliverable 3 of the TIDE/CERTAIN Study.Bruxelles,1996.
ANDRICH R,PORQUEDDU B.Educazione all'autonomia:esperienze,strumenti,proposte metodologiche.Europa Medicophyisica Vol.26 n.3/1990 pp.121-145.Torino:Minerva Medica,1990
ANTICO L.,CARETTA F.,PETRINI M.Vivere con le persone anziane.Regione Molise:UniversitàCattolica del Sacro Cuore,1990.
BAILY M.Les aides technologiques en Belgique:enjeux et besoins.Bruxelles:CEPIATH(Croix-Rouge de Belgique),1987.
BATESON G.Steps to an Ecology of Mind.New York:Ballantine,1972.
BATESON G.Mind and Nature.A Necessary Unit.New York:E.D.Dutton,1979.
BOULONGNE D.Classification et financement des Aides Techniques.Le domicile:espace de vie,de confort et de soins.Proceedings of the"8èmes Journées d'Etudes Nationales d'Ergothérapie",1991.
BOURGEOIS E.L'analyse des besoins de formation dans les organisations.Mesure et Evaluation en éducation,1991,14:1.
BOZIC N.,MURDOCH H.(Ed.).Learning Through Interaction-Technology and Children with Multiple Disabilities.London:David Fulton Publishers,1996.
BRIGHTMAN A.,GREEN P.Independence Day-Designing Computer Solutions for Individuals With Disabilities.Allen,Texas:DLM Publisher,1990.
BRUNELLES P.Ergothérapeuths et relations thérapeuthiques-Handicaps et Inadaptations.Paris:Les Cahiers du CTNRHI,1992,60:51-67.
BRUNELLES P.Histoires d'Aides Techniques—Handicaps et Inadaptations.Paris:Les Cahiers du CTNRHI,1994,62:45-60.
CENTRE INTERDISCIPLINAIRE SUR LE VIEILLISSEMENT.Repers-Senior.Bruxelles,1995.
CHARLEBOIS-MAROIS C.Everybody's Technology—a Sharing of Ideas in Augmentative Communication.Montreal:Charlecoms,1985.
CHURCH G.,GLENNEN S.The Handbook of Assistive Technology.San Diego:Singular Publishing Company,1992.
CNFLRH.Guide des Aides techniques pour le bien-être des personnesâgées.Paris:CNFLRH,1991.
EUSTAT 62.
CONTE M.Les produits pour mieux vivre:un nouveau marché:Propositions pour l'avenir du handicap.RapportàJean Gatel.Paris:public pamphlet,1984.
COOK A.M.,HUSSEY S.M.Assistive Technologies:Principles and Practice.Saint Louis:Mosby,1995.
CRESSON E.Enseigner et apprendre.Vers la societécognitive.Livre blanc sur l'éducation et la formation.Bruxelles:European Commission,1996.
CULLEN K.,MORAN R.Technology and the Elderly:the role of technology in prolonging the independence of the elderly in the community care context.Dublin:Work Research Center and EKOS,1991.
DANISH CENTRE FOR TECHNICAL AIDS FOR REHABILITATIONAND EDUCATION:
El-kørestolen 1989;Min kørestol.1985;Gørdagligdagen nemmere.1995;Det handler om velvære,1996;
En kreativ udfordring,1991;Ufrivillig vandladning,1991;Smart Home,forældre og handicappede,1994,Mobile Telephones,1996.,Telehjælpemidler,1993.
DE LA BELLACASA R.,GARCIA VISO M.(Eds.).Empleo,Discapacidad e Innovaciòn Tecnològica.Madrid:FUNDESCO Collecion Estudios y Documentos,1987.
EDWARDS L.A.Using knowledge and technology to improve the quality of life of people who have disabilities:a Prosumer Approach.Cornucopia of Disability Information(CODI):http://codi.buffalo.edu,1992.
ENDERBY P.(Ed.)Assistive Communication Aids for the Speech Impaired.Edinburgh:Churchill Livingstone.1987.
ENGELHARDT T.Jr.The Foundations of Bioethics.New York:Oxford University Press,1985.
EQUAL OPPORTUNITIES CENTRE FOR DISABLED PERSONS.Bygningsrelementet 1995 omtilgængeligheds kravene.Copenhagen:Equal Opportunities Centre For Disabled Persons,1996.
FALISE F.,LEBRUN T.,SAILLY J.-C.,PIDOU L.,DEMAN M.Les besoins des personnes âgées en accessoires de la vie courante.Lille:Cresge,1986.
EUSTAT 63.
FINKELSTEIN V.Attitudes and disabled people:Issues for discussion.World Rehabilitation Fund,Inc.,Monograph n.5,(published also on"International Exchange of Experts and Information in Rehabilitation"(IEEIR),gopher ieeir.unh.edu).
FLIPPO K.F.,INGE K.J.,BARCUS M.Assistive Technology:A resource for school,work,and community:Paul H.Brookes,1995.
FLOYD M.,Information Technology Training for People with Disabilities.Disability&Rehabilitation Series,v.4.London:Jessica Kingsley Publishers,1993.
GALVIN J.C.,SCHERER M.J.(Ed.).Evaluating,Selecting and Using Appropriate Technology.Maryland:Aspen Publication,1996.
HACKEN V.Ph.Des structures de travail pour construire du sens.Analyse de pratique et modélisation en formation d'adulte.Louvain-La-Neuve:Mémoire UCL,1966.
HANIN P.-Y.Les personnes âgées et leur autonomie:étude des besoins,de l'offre,et projet de création d'entreprise.Namur:Mémoire en Sciences Economiques et Sociales,1994.
HEART.Assistive Technology training in Europe,Bruxelles:European Commission,1995.
HEART.Coherence between rehabilitation and mainstream industries in the field of new media,Bruxelles:European Commission,1994.
HEART.Coherence between and among rehabilitation technology industrial sectors-Overview.Bruxelles:European Commission,1994.
HEART.European service delivery systems in rehabilitation technology.Hoensbroek:IRV,1994.HEART.Improving service delivery systems for assistive technology-a European strategy,Bruxelles:European Commission,1995.
HEART.Line A.2.3.:condensed version.New and more efficient standardization for users with disabilities.Bruxelles:European Commission,1994.
HEART.Line A.Standards,Testing,Certification.Specification of rehabilitation technology-A.3.4.A model for user influence on standardization.Bruxelles:European Commission,1994.
HEART.Line C.Rehabilitation technology service delivery-C.4.Report 2.Rehabilitation technology service delivery systems in Europe.Bruxelles:European Commission,1994.
HEART.Line C.Rehabilitation technology service delivery-C.5.1.Final Report on service delivery.Bruxelles:European Commission,1994.
HEART.Line E.Rehabilitation Technology Training-E.1.Report and assessment of existing programmes in rehabilitation technology.Bruxelles:European Commission,1994.
HEART.Line E.Rehabilitation Technology Training-E.1.1.Existing programmes in Europe and North America.Bruxelles:European Commission,1994.
HEART.Line E.Rehabilitation Technology Training-E.2.1.Report on job profile and training requirements for rehabilitation technology specialists and other related professions.Bruxelles:European Commission,1994.
HEART.Technology assisting disabled and older people in Europe.Bruxelles:European Commission,1995.
HELIOS II.Social Integration and Independent Living.Rapport d'activités.Bruxelles:European Commission,1994.
EUSTAT 64.
HELIOS II.Social Integration and Independent Living.Rapport d'activités.Bruxelles:European Commission,1995.
HELIOSII.Séminaire final du programme européen:groupes thématiques,Alava:European Commission,1996.
HIEBERT M.B.,SMALLWOOD W.N.Now for a completely different look at need analysis.Training and Development Journal,1987;41;(5):75-79.
JAY P.Coping with disability.London:DLF,1981.
LAZZARO J.Adaptive technologies for learning and work environments.American Library Association,1993.
LAZZARO J.Adapting PCs for disabilities.Addison-Wesley,1996.
LECONTE BEAUPORT M.-F.Intégration des savoirs,des savoirs-faire et des savoirs-être par le biais des
représentations véhiculées par les formateurs dans la relation éducative.Mesure etévaluation en éducation,
1995;18(1):3-35.
LESNE M.Travail pédagogique et formation d'adultes.Paris:PUF,1977.
LEWIS R.B.Special Education technology:Classroom applications.Pacific Grove:Brooks/Cole,1993.
LIGHT J.Toward a definition of comunicative competence for individuals using augmentative and
alternative communication systems.Augmentative and Alternative Communication,1989,5(2):137-144.
LORENTSEN O.,HEM K.G.(SINTEF REHAB).Critical factors and general outcomes of assistive
technology.Oslo:TIDEHorizontal Study.Certain,1995.
MAC FEE S.Choisir une aide technique.Déficiences motrices et handicaps,1996:400-410.
MALE M.Technology for inclusion:Meeting the special needs of all students,1994.
MALGLAIVE G.Enseigneràdes adultes.Paris:PUF,1990.
MANDELSTAM M.How to Get Equipment for Disability.London:The Disabled Living Foundation,1993.
MILANI COMPARETTI A.The basic criteria for prognosis and assessment of results in rehabilitationL.ittle
Club Clinics in Development Medicine 1960,2:13-24.
MILANI COMPARETTIA.Dalla medicina della malattia alla medicina della salute.In:Caffo E.(Ed.)Abusi e violenze all'infanzia.Milano:Unicopli,1982:78-92.
MILANI COMPARETTI A.,ROSER L.O.Forderung der Normalität und der Gesundheit in der Rehabilitation:Voraussetzung fur die reale Anpassung Behinderter.Behinderte in Familie,Schule,und Gesellschaft 1981:4.
PERETTIA.Organiser des formations.Paris:PUF,1993.
PETIT B.,MARTEAU D.Ajoutez de l'aplomb aux années.Guide pratique.,IEIAS,1993.
PHILIPS B.,ZHAO H.Predictors of assistive technology abandonment.Assistive Technology,1993,5:36-45.
POULSON D.,ASHBY M.,RICHARDSON S.USERfit.A practical handbook on user-centered design for Assistive Technology.TIDE,Bruxelles:European Commission,1966.
QUIVY R.,RUQUOY D.,VAN CAMPENHOUDT L.Malaise dans l'école.Bruxelles:Fac St Louis,1989.
EUSTAT 65.
RANCIERE P.Le maître ignorant:cinq leçons sur l'émancipation intellectuelle.Paris:Fayard,1987.
RICA.Evaluating aids for disabled people,London:Research Institute for Consumer Affair,1984.
SCHERER M.J.The Matching Person&Technology(MPT)Model,Copyright 1991,486 Lake Rd.Webster,NY 14580,1994 Version.
SIMON L.Polyarthrite rheumatoïde et économie articulaire.Geigy,1982.
STIEFEL R.,Trends of development in managers'learning.Lehman,R.G.Planung,Praxis,Fallbeispiele der betrieblichen Schulung.Stuttgart:Didacta,1989.
THE NORDIC COMMITTEE ON DISABILITY.Nordic guidelines for computer accessibility.Bromma:The Nordic Committee on Disability,1993.
TRACE RESOURCE BOOK 1996/97.Assistive Technology for Communication,Control and Computer Access.Madison:Trace Research and Development Center,1996.
VILLALTA M.F.(Ed.).Tecnologias de la Informacion y Discapacidad.Madrid:FUNDESCO Collecion Estudios y Documentos,1988.
VLICHT,Lustrumboek:Integratie door Hulpmiddelen.Leuven:VLICHT,1994.
VYGOTSKIJ L.Mind in society.Cambridge:Harvard University Press,1978.
