Clinical application of reserved gastric tube in neuroendoscopic endonasal surgery for pituitary tumor
2024-05-06XiChenLongYaoZhangZhiFengWangYiZhangYuHuaYinXueJianWang
Xi Chen,Long-Yao Zhang,Zhi-Feng Wang,Yi Zhang,Yu-Hua Yin,Xue-Jian Wang
Abstract BACKGROUND The neuroendoscopic approach has the advantages of a clear operative field,convenient tumor removal,and less damage,and is the development direction of modern neurosurgery.At present,transnasal surgery for sphenoidal pituitary tumor is widely used.But it has been found in clinical practice that some patients with this type of surgery may experience post-operative nausea and vomiting and other discomforts.AIM To explore the effect of reserved gastric tube application in the neuroendoscopic endonasal resection of pituitary tumors.METHODS A total of 60 patients who underwent pituitary adenoma resection via the endoscopic endonasal approach were selected and randomly divided into the experimental and control groups,with 30 in each group.Experimental group:After anesthesia,a gastric tube was placed through the mouth under direct vision using a visual laryngoscope,and the fluid accumulated in the oropharynx was suctioned intermittently with low negative pressure throughout the whole process after nasal disinfection,during the operation,and when the patient recovered from anesthesia.Control group: Given the routine intraoperative care,no gastric tube was left.The number of cases of nausea/vomiting/aspiration within 24 h post-operation was counted and compared between the two groups;the scores of pharyngalgia after waking up,6 h post-operation,and 24 h postoperation.The frequency of postoperative cerebrospinal fluid leakage and intracranial infection were compared.The hospitalization days of the two groups were statistically compared.RESULTS The times of postoperative nausea and vomiting in the experimental group were lower than that in the control group,and the difference in the incidence of nausea was statistically significant (P <0.05).After the patient woke up,the scores of sore throat 6 h after the operation and 24 h after operation were lower than those in the control group,and the difference was statistically significant (P <0.05).The number of cases of postoperative cerebrospinal fluid leakage and intracranial infection was higher than that of the control group,but there was no statistically significant difference from the control group (P >0.05).The hospitalization days of the experimental group was lower than that of the control group,and the difference was statistically significant (P <0.05).CONCLUSION Reserving a gastric tube in the endoscopic endonasal resection of pituitary tumors,combined with intraoperative and postoperative gastrointestinal decompression,can effectively reduce the incidence of nausea,reduce the number of vomiting and aspiration in patients,and reduce the complications of sore throat The incidence rate shortened the hospitalization days of the patients.
Key Words: Neuroendoscopy;Endonasal approach;Pituitary tumor;Reserved gastric tube;Nausea;Vomiting;Aspiration;Complications
INTRODUCTION
Pituitary tumors are primary intracranial tumors commonly encountered in clinical practice,accounting for about 10% of intracranial tumors and second only to neuroepithelial tumors and meningiomas[1,2].Transsphenoidal pituitary adenoma resection is a mature technique,and it has the advantages of less surgical trauma,shorter operation time,faster postoperative recovery,and fewer complications compared to traditional craniotomy[3-5].The neuroendoscopic approach has the advantages of a clear operative field,convenient tumor removal,and less damage,and is the development direction of modern neurosurgery[6].It has been found in clinical practice that some patients with this type of surgery may experience post-operative nausea and vomiting (PONV) and other discomforts[7].We hypothesize is that there is a correlation with the endonasal approach surgery.Since intraoperative disinfectant,washing fluid,bleeding,and postoperative mucosal oozing flow into the stomach through the nasopharynx,it is easy to induce postoperative vomiting in patients.Additionally,because the vomit contains bloody liquid,patients and their families become emotionally stressed.At the same time,patients are prone to flatulence due to bilateral nasal congestion prompting them to open their mouths to breathe,which will also induce and aggravate nausea and vomiting after general anesthesia,increasing the possibility of aspiration.PONV is one of most frequent side effects after anesthesia[7,8],occurring in 30%of unselected patients and up to 70% of “high-risk” patients during the 24 h after emergence[9].In severe cases,surgical wound bleeding may be induced by increased intracranial pressure and blood pressure,resulting in delayed discharge[10] and a possible unexpected admission[11,12].
In light of the aforementioned postoperative problems,this study adopted the intervention method of gastric tube application during the endoscopic endonasal resection of pituitary tumors to explore the application of reserved gastric tubes in patients,achieving promising results.
MATERIALS AND METHODS
Ethics approval and consent to participate: This study was reviewed and approved by the Ethics Committee of Affiliated 2 Hospital of Nantong University.
General information
In total,60 patients with pituitary tumors admitted to the neurosurgery department of our hospital from February 2021 to February 2023 were selected as the research participants.According to the random number method,the patients were evenly divided into the experimental group and the control group.The experimental group consisted of 17 males and 13 females aged 39.6 ± 14.7 years,and the control group,18 males and 12 females aged 36.72 ± 15.4 years.There was no statistically significant difference between the two groups in terms of sex,age,condition,course of disease,and other baseline information (P>0.05);both groups were comparable.
Inclusion criteria: (1) Adult patients diagnosed with pituitary adenoma who underwent endoscopic transsphenoidal pituitary tumor surgery for the first time;(2) Pituitary adenoma ≤ 3 cm;(3) No surgical contraindications;(4) Participants with American Society of Anesthesiologists classification Ⅰ-Ⅲ;and (5) Voluntarily signed the patient’s informed consent form.
Exclusion criteria: (1) Cases of pituitary adenoma combined with cerebral aneurysm and cerebrovascular malformation;(2) Mental disorders;(3) Pregnant patients;(4) Hypertrophy of the tonsils;(5) Patients with chronic pharyngitis;(6) Patients with severe heart,lung,and/or liver disease;and/or (7) Renal dysfunction.
Research methods
Surgical method:Both groups underwent neuroendoscopic endonasal pituitary tumor resection by the same medical team.Each patient was placed in the supine position,the trachea was intubated under conventional general anesthesia,and the nasal cavity and operative field were disinfected with povidone iodine.The nasal cavity was filled with epinephrine saline cotton pads to shrink the nasal mucosa.The neuroendoscope was inserted;the right middle turbinate was moved laterally under the endoscope;the pedicled mucosal flap of the right nasal septum was prepared;the back of the nasal septum and then the nasal passage were opened;the anterior wall of the sphenoid sinus was ground;the inner septum and the sphenoid sinus mucous membrane were removed;and the sellar floor,sellar tubercle,and sphenoid plateau bone were ground.The dura mater was cut to expose the tumor,the tumor boundary was separated after intratumoral decompression,and the bleeding was completely stopped after tumor resection.Autologous fat,artificial dura mater,autologous fascia,and a pedicled nasal septum mucosa flap were used to reconstruct the skull base.Naxi cotton was used to stuff the nasal cavity for support,and at this time,the lower nasal passage was kept unobstructed as much as possible[3].
Intervention method of the experimental group:After the anesthesiologist anesthetized and intubated the trachea,while inserting a No.14 gastric tube (Fuerkai,China),the anesthesiologist and the nurse were assisted by a video laryngoscope(Zhejiang Youyi Medical,China) to confirm that the position was below the oropharynx (oropharyngeal tongue root plane).Low negative pressure control was adopted during the operation;the suction pressure of the low negative pressure suction device (Simanfeng Company,China) was 100-120 mmHg.After the operation,the esophagus and oropharynx were sucked out before the stomach tube was removed.
Intervention methods for the control group:Routine care was given,and gastric tubes were blindly inserted through the nose or through the mouth in patients with disturbance of consciousness after surgery.
Evaluation indicators
PONV times and aspiration times:The number of patients with PONV;coughing,dyspnea,blood oxygen saturation below 90%,suffocation,other symptoms during or after vomiting,or food residues that could be seen through mouth and nose suction were judged as aspiration[13].
Scoring of sore throats after the patient woke up and after the operation:The Visual Analogue Scale (VAS) was used to score the patients after they woke up as well as the ward nurse at 6 h and 24 h after the operation,respectively.To assess sore throat,the VAS is used to assess pain and is widely used clinically[14].The basic method is to use a moving ruler of about 10 cm long,with 10 scales,on one side,and the two ends are “0” and “10.” And 0 means no pain,and 10 means difficulty.The most severe pain endured.Specifically,0 is no pain;1-3 is mild pain;4-6 is moderate pain;7-10 is severe pain.
Cases of postoperative cerebrospinal fluid leakage and intracranial infection and hospitalization days of patients:The number of cases of cerebrospinal fluid leakage and intracranial infection,as well as the length of hospitalization of patients were recorded after the operation.
Statistical methods
SPSS 24.0 statistical software was used for the t andχ2test and Fisher’s exact test.
RESULTS
Comparison of PONV times and aspiration times between the two groups
The number of nausea in the test group was less than that in the control group,and the difference was statistically significant (P<0.01).The frequency of vomiting in the experimental group was less than that in the control group,but the difference was not statistically significant (P>0.05).The number of aspirations in the experimental group was less than that in the control group,and the difference was not statistically significant (P>0.05;Table 1).

Table 1 Comparison of postoperative nausea and vomiting aspiration between the two groups of patients (mean ± SD,n=30)
Scores of sore throat after waking up and postoperatively
The VAS scores of patients in the experimental group after waking up were lower than that in the control group,and the difference was statistically significant (P<0.05).The VAS scores of the experimental group were lower than that of the control group at six hours post-operation,and the difference was statistically significant (P<0.05).The 24 h postoperative VAS score of the experimental group was lower than that of the control group,and the difference was statistically significant (P<0.05;Table 2).

Table 2 Comparison of sore throat scores between the two groups after waking up,6 hours postoperatively and 24 hours postoperatively (mean ± SD,n=30)
Comparison of postoperative cerebrospinal fluid leakage, intracranial infection, and hospitalization days between the two groups
There was one case of cerebrospinal fluid leakage in the experimental group compared to the three in the control group,though the difference was not statistically significant (P>0.05).There was one case of intracranial infection in the experimental group compared to the two in the control group;the difference was statistically significant (P>0.05).The experimental group had 7.91 ± 2.020 days of hospitalization compared to the control group’s 8.94 ± 2.503 days;the difference was statistically significant (P<0.05;Table 3).
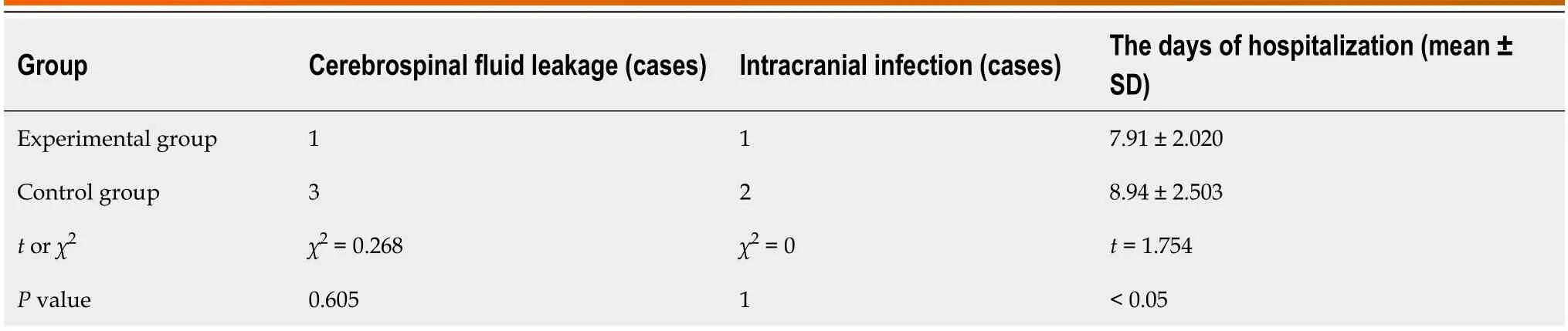
Table 3 Comparison of postoperative cerebrospinal fluid leakage (cases) and intracranial infection (cases) and hospitalization days between the two groups (mean ± SD,n=30)
DISCUSSION
At present,the advancement of neuroendoscopic technology has enabled this to be widely used in sellar region lesions,such as pituitary tumors.Cappabiancaet al[15] emphasized that the important feature of endoscopic transsphenoidal surgery is that it does not use a retractor to dilate the nasal cavity and uses the endoscope as a lighting and observation device,utilizing the physiological channels of the nasal cavity to gradually shrink the nasal mucosa to expand the operation path.However,the endoscopic lens is easily covered by blood,water vapor,and other substances,which interfere with the operative field[3,4].The surgeon needs to wash the lens and wound surface intermittently to keep the operative field clear.Therefore,it is inevitable that there will be fluid accumulation in the throat and upper gastrointestinal tract,mixed with disinfectant iodophor,blood,and other irritating liquids,which will irritate the digestive tract and cause related complications and discomfort.Therefore,it is necessary to study similar technologies to reduce related side effects,reduce the occurrence of complications,and improve patient comfort.
During endonasal neuroendoscopic surgery,there is fluid accumulation in the surgical area.Although the aspirator will suck out some bloody fluid (including blood,disinfectant,and flushing fluid),because the patient is in an unconscious state during general anesthesia,there is no throat reflex[8,9].Due to the connection between the nasal and oral cavities through the pharynx and the impact of body position,some liquid will accumulate in the oropharynx and upper gastrointestinal tract along the posterior pharyngeal wall.During the awakening period of general anesthesia,the patient’s consciousness gradually recovers,and involuntary swallowing will occur.The mouth is the only channel that can be used at this time.Postoperative nasal bleeding and frequent swallowing can cause a large amount of gas and blood to be swallowed into the digestive tract,causing gastric dilation,leading to nausea and vomiting occurrence[16,17].
At present,such factors have not been fully considered clinically,and no pharyngeal or upper gastrointestinal drainage tube was placed during the operation.In the experimental group of this study,a gastric tube was inserted after anesthesia,and the fluid was drained during the operation.After the operation,the miscellaneous fluid was sucked out and then removed.Through the study of this group,we found that intraoperative gastric tube reservation is necessary in the perioperative process of the neuroendoscopic endonasal resection of pituitary tumors.
Reserving gastric tube during operation can improve postoperative vomiting and aspiration
Postoperative nausea,vomiting and aspiration are common postoperative complications,and the incidence rate of highrisk patients with major surgery can reach 70% to 80%[7].In addition to increasing postoperative discomfort,frequent vomiting can also lead to delayed eating time,increased wound tension,electrolyte imbalance,aspiration,and other complications,which is an important reason for prolonging the hospital stay and increasing patient satisfaction[10].The intranasal resection of pituitary tumors may cause intraoperative bleeding to flow into the stomach through the nasopharynx,and postoperative nasal bleeding will continue to flow in,making the stomach contain more blood and irritating the gastrointestinal tract.When the patient vomits,there will be bloody fluid,emotionally aggravating the patient.These will induce and aggravate postoperative nausea and vomiting in patients and increase the incidence of aspiration.In this study,the nausea,vomiting,and aspiration in the experimental group improved correspondingly to those in the control group,and the number of nausea cases in the experimental group was significantly different from that in the control group,which was statistically significant.This study shows that the intraoperative reserved gastric tube can improve postoperative nausea symptoms.
Reserving gastric tube during the operation can improve postoperative sore throat
Postoperative sore throat (POST) is one of the most common airway complications after general anesthesia.Studies have pointed out that the incidence of POST can reach 10% to 60%[18,19].It is worth noting that severe POST may lead to dyspnea and dysphagia,reduce patient satisfaction with anesthesia,and may even prolong hospital stay.The site and position of surgery are important reasons for POST.The incidence of POST in head and neck surgery,especially in oropharyngeal surgery,is bound to be higher than that of non-neck surgery patients due to reasons such as the compromised surgical site or the surgeon pulling the airway during the operation[20,21].
For patients undergoing endonasal surgery for pituitary tumors,in addition to the discomfort caused by tracheal intubation to the throat,due to surgery in the nasopharynx,intraoperative bleeding and other stimuli will cause postoperative pharyngeal discomfort.In this study,by sucking out the effusion,reducing the stimulation of iodine and other disinfectants and blood,and other factors,the postoperative pharyngeal discomfort was improved,which had a good effect on the postoperative comfort of patients.Insertion of a gastric tube can improve postoperative discomfort for pituitary tumor removal.
Comparison of postoperative cerebrospinal fluid leakage, intracranial infection, and hospitalization days between the two groups
Since the 1990s,skull base endoscopy has allowed great progress in the clinical application of neurosurgery and has become a routine operation for pituitary tumor resection.At the same time,serious complications,such as cerebrospinal fluid leakage and intracranial infection,have gradually attracted attention[4].Safe and effective intraoperative skull base reconstruction can reduce postoperative short-term and long-term cerebrospinal fluid leakage,thereby preventing intracranial infection.
However,postoperative behaviors,such as sneezing,coughing,expectoration,and defecation increase intracranial pressure,which can damage the sphenoid sinus and cause cerebrospinal fluid leakage[3].In this study,the number of cases of cerebrospinal fluid leakage and brain infection in the experimental group was more than those in the control group.Although there was no statistical significance,the small number of cases may have contributed to this.However,the hospitalization days of the experimental group were statistically significantly lower than those of the control group,suggesting that the reserved gastric tube during the operation was beneficial for the patients.
CONCLUSION
Reserved gastric tube application in the resection of pituitary tumors through the endoscopic approach through the nose can predictably improve patients’ postoperative pharyngeal discomfort and improve the symptoms of postoperative vomiting and aspiration.It has a high clinical application value and is suitable for all kinds of nerve promotion of the endoscopic endonasal approach in tumor resection.
ARTICLE HIGHLIGHTS
Research background
The neuroendoscopic approach has the advantages of a clear operative field,convenient tumor removal,and less damage,and is the development direction of modern neurosurgery.At present,transnasal surgery for sphenoidal pituitary tumor is widely used.But it has been found in clinical practice that some patients with this type of surgery may experience postoperative nausea and vomiting (PONV) and other discomforts.
Research motivation
At present,it has been found that some patients after endonasal endosphenoidal neuroendoscopy surgery may experience PONV and other discomforts.Whether there can be corresponding methods to avoid the occurrence of similar events is our research motivation.
Research objectives
To explore the effect of reserved gastric tube application in the neuroendoscopic endonasal resection of pituitary tumors.
Research methods
Patients who underwent pituitary adenoma resectionviathe endoscopic endonasal approach were selected and randomly divided into the experimental and control groups.Experimental group: After anesthesia,a gastric tube was placed through the mouth under direct vision using a visual laryngoscope,and the fluid accumulated in the oropharynx was suctioned intermittently with low negative pressure throughout the whole process after nasal disinfection,during the operation,and when the patient recovered from anesthesia.Control group: Given the routine intraoperative care,no gastric tube was left.The number of cases of nausea/vomiting/aspiration within 24 h post-operation was counted and compared between the two groups;the scores of pharyngalgia after waking up,6 h post-operation,and 24 h postoperation.The frequency of postoperative cerebrospinal fluid leakage and intracranial infection were compared.The hospitalization days of the two groups were statistically compared.
Research results
The times of postoperative nausea and vomiting in the experimental group were lower than that in the control group.The number of cases of postoperative cerebrospinal fluid leakage and intracranial infection was higher than that of the control group.The hospitalization days of the experimental group was lower than that of the control group.
Research conclusions
Reserved gastric tube application in the resection of pituitary tumors through the endoscopic approach through the nose can predictably improve patients’ postoperative pharyngeal discomfort and improve the symptoms of postoperative vomiting and aspiration.
Research perspectives
In the next step,we can further study the pressure attracted by the negative pressure of the reserved gastric tube and the use time of the reserved gastric tube,so as to better propose the scheme of the reserved gastric tube.
FOOTNOTES
Co-first authors:Xi Chen and Long-Yao Zhang.
Author contributions:Chen X,Wang XJ,and Yin YH treated all these patients;Zhang Y and Wang ZF collected the data;Chen X and Zhang LY analyzed the data;Wang XJ wrote the manuscript,Zhang LY and Wang XJ revised and checked this article;All authors contributed to the article and approved the submitted version.
Supported byTraditional Chinese Medicine Science and Technology Project in Jiangsu Province,No.YB2 015113;the Science and Technology Program of Nantong Health Committee,No.MA2019003,No.MA2021017,No.MB2021026,and No.MB2 021027;Science and Technology Program of Nantong City,No.Key003,No.MS12015016 and No.JCZ2 022040;and Kangda College of Nanjing Medical University,No.KD2021JYYJYB025,No.KD2022KYJJZD019,No.KD2022KYJJZD022,and No.2023ZC127.
Institutional review board statement:This research has been approved by the ethics committee of Affiliated Hospital 2 of Nantong University.
Informed consent statement:Informed consent has been obtained and this investigation has been conducted according to the principles expressed in the Declaration of Helsinki.
Conflict-of-interest statement:All the authors report no relevant conflicts of interest for this article.
Data sharing statement:The original contributions presented in the study are included in the article,further inquiries can be directed to the corresponding author at 6841441@163.com.
STROBE statement:The authors have read the STROBE Statement—checklist of items,and the manuscript was prepared and revised according to the STROBE Statement—checklist of items.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORCID number:Long-Yao Zhang 0000-0001-7460-7903;Zhi-Feng Wang 0000-0001-8154-0356;Yi Zhang 0000-0002-4618-6256;Yu-Hua Yin 0000-0003-3760-0264;Xue-Jian Wang 0000-0003-0389-5674.
Corresponding Author's Membership in Professional Societies:American Association for Peripheral Neurosurgery,0921121.
S-Editor:Li L
L-Editor:A
P-Editor:Yuan YY
杂志排行
World Journal of Clinical Oncology的其它文章
- Current interventional options for palliative care for patients with advanced-stage cholangiocarcinoma
- Ferroptosis biomarkers predict tumor mutation burden's impact on prognosis in HER2-positive breast cancer
- Nomogram based on multimodal magnetic resonance combined with B7-H3mRNA for preoperative lymph node prediction in esophagus cancer
- Establishment of a prognosis predictive model for liver cancer based on expression of genes involved in the ubiquitin-proteasome pathway
- Transarterial chemoembolization plus stent placement for hepatocellular carcinoma with main portal vein tumor thrombosis: A meta-analysis
- PD-1 antibody in combination with chemotherapy for the treatment of SMARCA4-deficient advanced undifferentiated carcinoma of the duodenum: Two case reports