Effectiveness and safety of electroacupuncture for the treatment of pain after laparoscopic surgery:a systematic review
2022-07-20HUANGYusiYANGJijuLIXinyiHAOHuifengLIChongZHANGFanLINHaimingXIEXianfeiHEKeTIANGuihua
HUANG Yusi,YANG Jiju,LI Xinyi,HAO Huifeng,LI Chong,ZHANG Fan,LIN Haiming,XIE Xianfei,HE Ke,TIAN Guihua
HUANG Yusi,YANG Jiju,LI Xinyi,LI Chong,ZHANG Fan,LIN Haiming,XIE Xianfei,Beijing Dongzhimen Hospital,Beijing University of Chinese Medicine,Beijing 100700,China
HAO Huifeng,Department of Integration of Chinese and Western Medicine,Key Laboratory of Carcinogen esis and Translational Research (Ministry of Education/Beijing),Peking University Cancer Hospital &Institute,Beijing 100142,China
Abstract OBJECTIVE:To evaluate the clinical effectiveness and safety of electroacupuncture for treating pain after laparoscopic surgery.METHODS:The following databases were searched(since their establishment until November 16,2021) for randomized controlled trials (RCTs) on electroacupuncture for pain after laparoscopic surgery:PubMed,Embase,the Cochrane Library,Web of Science,China National Knowledge Infrastructure Database,Wanfang Database,China Science and Technology Journal Database,and Chinese Biomedical Literature Database.Data were screened independently and extracted by two reviewers.Two researchers independently extracted and cross-checked data and applied the modified Jadad scale and the Cochrane-recommended assessment method to evaluate the bias risk.The Meta-analysis was conducted using RevMan5.3 software.RESULTS:Twelve RCTs enrolling 788 patients were included.(a) For postoperative 24 h visual analogue scale,five trials were included on electroacupuncture+routine analgesia therapy vs routine analgesia therapy with significance in electroacupuncture conducted after surgery [mean difference (MD)=-0.63,95% confidence interval (CI) (-0.90,-0.37)],as well as in electroacupuncture conducted before and after surgery[MD=−1.01,95% CI (−1.62,−0.41)] and in surgery.However,two trials were included in electroacupuncture conducted 24 h before surgery with no significant difference [MD=−0.16,95% CI (−0.44,0.12)].(b) The anesthetics intake of electroacupuncture+routine analgesia therapy vs.routine analgesia therapy was significant [MD=−121.71,95% CI (−164.92,−78.49)].(c)The adverse effects of electroacupuncture+routine analgesia therapy vs.routine analgesia therapy were significant both in the incidence of postoperative nausea and vomiting [risk rate (RR)=0.49,95% CI (0.39,0.61)]and postoperative dizziness and headache [RR=0.14,95% CI (0.04,0.47)].CONCLUSION:The evidence showed that electroacupuncture combined with routine analgesia therapy effectively treated pain after laparoscopic surgery.However,more rigorously designed RCTs are required due to the low quality of the included studies and the incomplete outcome evaluation system.
Keywords:electroacupuncture;laparoscopy;pain;treatment outcome;safety;systematic review
1.INTRODUCTION
Recently,with minimally invasive technology evolving,laparoscopic surgery has been widely used to treat digestive and genitourinary systems diseases.It has become an essential medical tool in surgical diagnosis and treatment.1Laparoscopic surgery has the following advantages compared with traditional laparotomy:small incision range,fast recovery time,and low incidence of postoperative complications,which significantly improve the postoperative recovery rate of patients.However,approximately 30% of patients inevitably had moderate or severe pain postoperatively,2mainly manifested by local incision pain,abdominal pain due to peritoneal,diaphragm stretching and soft tissue inflammation,and shoulder pain caused by intraoperative gas filling.The poor postoperative analgesia may increase complications during hospitalization,prolong the hospitalization duration,and may not be conducive to postoperative recovery.3,4Therefore,finding the best analgesic treatment for pain after laparoscopic surgery has become an urgent clinical issue.
Laparoscopic postoperative analgesia is primarily treated with opioid analgesics,nonsteroidal anti-inflammatory drugs,and local anesthetics.However,they often cause a series of adverse drug reactions,such as drowsiness,nausea,vomiting,and respiratory inhibition,5not favorable to the postoperative rehabilitation of patients.Electroacupuncture is a modern acupuncture therapy that combines acupuncture with pulse current stimulation of different frequencies and modes to improve efficacy.6Clinical investigation showed that electroacupuncture could significantly reduce the incidences of postoperative pain and adverse drug reactions and decrease analgesic use.7,8However,relevant evidence to support its use is limited.Therefore,electroacupuncture's clinical effectiveness and safety for treating pain after laparoscopic surgery were evaluated to provide a clinical basis and reference.
2.METHODS
2.1.Inclusion criteria
(a) Study type:randomized controlled trials (RCTs).
(b) Participants:Patients who underwent laparoscopic surgery,with no limitations on the patients' age,sex,race,nationality,or course of the disease.
(c) Intervention measures:the experimental group comprised of patients who received electroacupuncture combined with routine analgesia (including patientcontrolled intravenous analgesia (PCIA),routine nursing,and other Western Medicine),and the control group consisted of patients who received routine analgesia therapy or routine analgesia therapy combined with sham electroacupuncture.
(d) Outcome indicators:visual analogue scale (VAS)score was the primary outcome indicator.Secondary outcome indicators were the intraoperative anesthetic dosage,the postoperative incidence of dizziness and headache,and postoperative nausea and vomiting.
2.2.Exclusion criteria
(a) Studies with incomplete data;(b) duplicate detection and publications;(c) studies not published in Chinese or English.
2.3.Methods and strategies of literature collection
Literature was retrieved from PubMed,Embase,the Cochrane Library,Web of Science,China National Knowledge Infrastructure Database,Wanfang Database,China Science and Technology Journal Database,and Chinese Biomedical Literature Database from their establishment until November 16,2021.In addition,the references of the selected literature were searched to supplement the relevant literature.The search terms were acupuncture,electroacupuncture,needling,electroacupuncture,needle therapy,auriculotherapy,acupoint therapy,laparoscopy,laparoscopic surgery,postoperative pain,randomized controlled trial,randomized controlled study,randomized controlled trial,and randomized controlled study.
2.4.Study selection
Two researchers (HUANG Yusi and YANG Jiju)independently read and screened the literature,extracted data,and cross-checked the data for any differences.When screening the literature,the title and abstract were read first.After excluding irrelevant literature,the full text was read to determine whether it satisfied the inclusion criteria.The data were extracted using a predefined form,which included details of the first author,country,year,the sample size of each group,age,the sex of patients,the type of surgery,American Society of Anesthesiologists (ASA) grade,the experimental and control interventions,intervention timing,outcomes,and bias risk.
2.5.Risk of bias assessment
The methodological quality of the included studies was evaluated by two reviewers (YANG Jiju and HUANG Yusi) according to the Cochrane Risk of Bias Assessment Tool provided by Cochrane Reviewer's Handbook 5.3:9(a) selection bias:whether the random allocation method was adopted,type of random allocation method and type of allocation hiding method was adopted;(b) implementation bias:whether a blinding method was applied on implementers and participants;(c) measurement bias:whether the blinding method was implemented in the outcome evaluation;(d)follow-up bias:whether there was a loss to follow-up or withdrawal and type of analysis method used;(e) report bias:whether there was a selective reporting of results;(f) other bias:whether there were other sources of bias.
2.6.Statistical analysis
Meta-analysis was performed using RevMan 5.3 software (Cochrane Collaboration,Oxford,UK).10Mean difference (MD) with the 95% confidence intervals (CIs)was used for continuous data,including the VAS score and intraoperative anesthetic dosage.In contrast,risk rate(RR) with 95% confidence intervals (CIs) was used for dichotomous data,including the incidence of postoperative adverse reactions.The χ2test andI2statistics were used to identify and measure statistical heterogeneity,which estimated variation resulting from study heterogeneity.The fixed-effect model was used for Meta-analysis if there was no statistical heterogeneity among the results.The random-effect model was used for Meta-analysis for statistical heterogeneity among the results.The level of the Metaanalysis was set to α=0.05.Significant clinical heterogeneity was treated by subgroup analysis or only descriptive analysis,and publication bias was conducted for outcome with included studies ≥ 10.
3.RESULTS
3.1.Study selection process
A total of 273 articles were initially detected,and after the layer-by-layer screening,12 RCTs11-22were included,with a total of 788 patients.The selection process is shown in Figure 1.
3.2.Study characteristics
The included studies' characteristics are shown in Table 1.Ten studies were conducted to investigate the effect of electroacupuncture+routine analgesia therapy (EA +RA)vsroutine analgesia therapy (RA) on pain recovery after laparoscopic surgery.11-15,18-22In addition,two studies were conducted on the effect of electroacupuncture+routine analgesia therapy (EA+RA)vssham electroacupuncture+routine analgesia therapy(Sham EA+RA) on pain recovery after laparoscopic surgery.16,17
3.3.Study quality
Of the 12 included trials,only one study21described the allocation hiding method and implemented the blind method.Two studis14,22only mentioned "random" and did not specify the random allocation method.One study19was conducted by drawing lots,and the rest of the studies11-13,15-18,20,21were assigned randomly by the method of random number table.The risk of bias summary is shown in Figure 2.
3.4.Postoperative 24-hour VAS scores
Seven trials11-15,21,22reported postoperative 24 h VAS scores.For electroacupuncture conducted 24 h before surgery of EA+RAvsRA,two trials were included,13,21with no statistical significance [MD=−0.16,95%CI(−0.44,0.12),P=0.26,I2=0%].Electroacupuncture conducted after surgery of EA+RAvs.RA;two trials were included,12,15showing a statistical significance [MD=−0.63,95%CI(−0.90,−0.37),P <0.000 01,I2=0%].Electroacupuncture conducted before and after surgery of EA+RAvsRA,two trials were included,11,22with a statistical significance [MD=−1.01,95%CI(−1.62,−0.41),P=0.001,I2=93%].Electroacupuncture was conducted in surgery of EA+RAvs.RA;one trial was included,14showing a statistical significance [MD=−1.92,95%CI(−2.32,−1.52),P <0.000 01] (Figure 3).
3.5.Intraoperative anesthetic dosage
Four trials16-19reported intraoperative anesthetic dosage in patients undergoing laparoscopic surgery.EA+RA was significantly lower than RA [MD=−121.71,95%CI(−164.92,−78.49),P<0.000 01,I2=59%].For EA+RA vs RA,two trials were included,18,19with a statistical significance [MD=−136.18,95%CI(−183.02,−89.34),P<0.001,I2=0%].For EA+RAvsSham EA+RA,two trials were included,16,17showing a statistical significance [MD=−110.37,95%CI(−192.80,−27.93),P=0.009,I2=84%] (Figure 4).
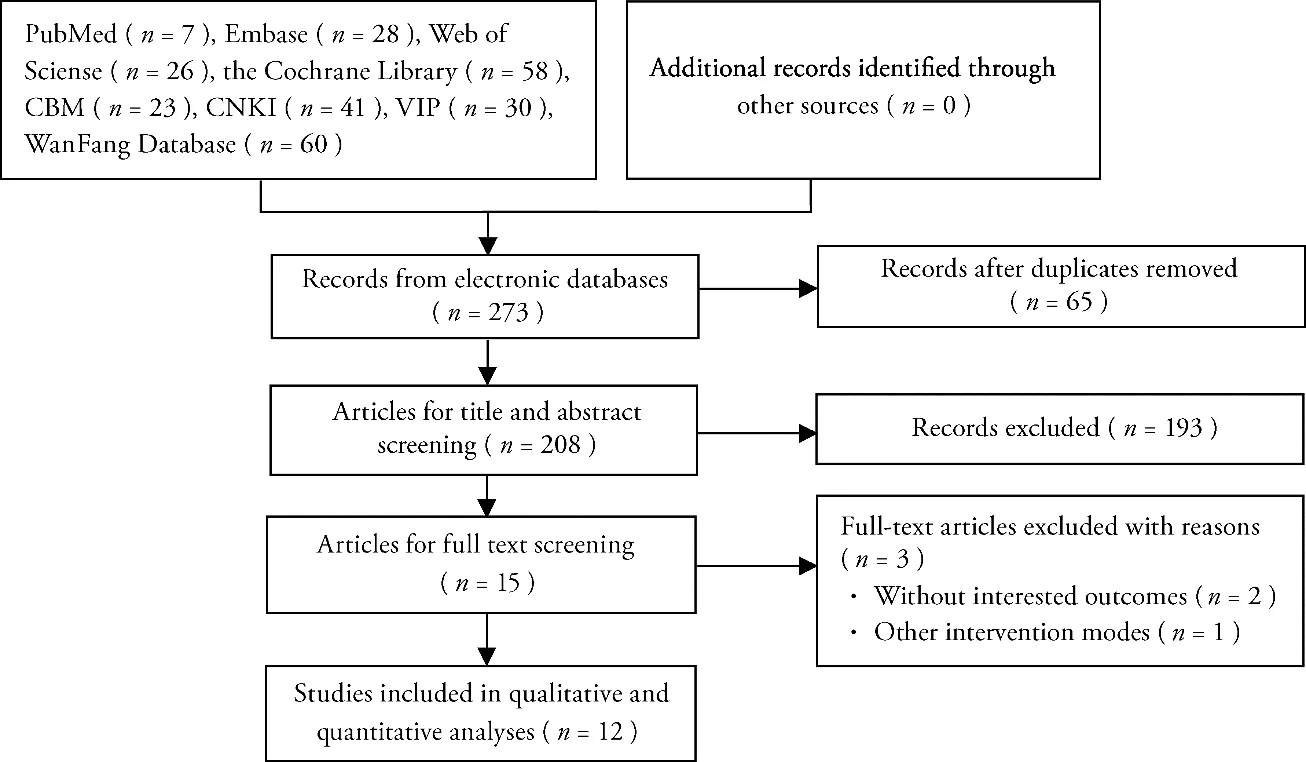
Figure 1 PRISMA flowchart of the selection process
3.6.Postoperative adverse reaction rate
(a) Incidence of postoperative nausea and vomiting

Ten trials11-15,17,18,20-22reported postoperative nausea and vomiting.Results showed that EA+RA was more effective than RA in improving postoperative nausea and vomiting after laparoscopic surgery [RR=0.49,95%CI(0.39,0.61),P <0.000 01,I2=37%] (Figure 5).
(b) Incidence of postoperative dizziness and headache
Three trials11,14,17reported postoperative dizziness and headache.EA+RA was found more effective than RA in improving dizziness and headache after laparoscopic surgery [RR=0.14,95%CI(0.04,0.47),P=0.001,I2=0%] (Figure 6).
3.7.Sensitivity analysis
For the outcome of the postoperative 24 h VAS scores,the included studies were excluded one by one.Our results showed that the Meta-analysis results did not change substantially,indicating stable results.
3.8.Publication bias
Sensitivity analysis was performed for ten RCTs11-15,17,18,20-22in terms of postoperative nausea and vomiting incidence,which showed an asymmetry indicating a publication bias (Figure 7).
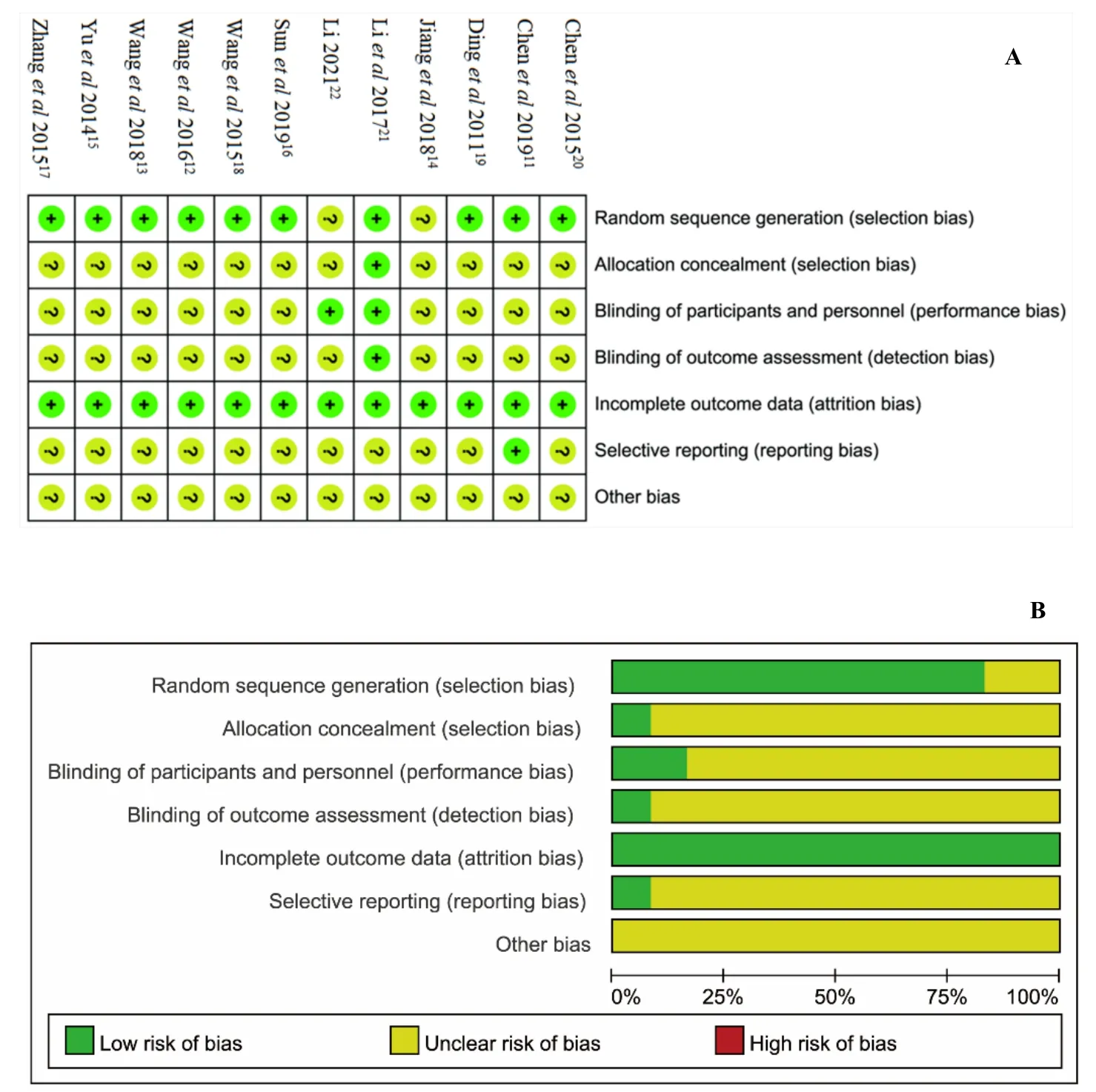
Figure 2 Risk of bias

Figure 3 Forest plot:postoperative 24 h visual analogue scale scores

Figure 4 Forest plot:intraoperative anesthetic dosage
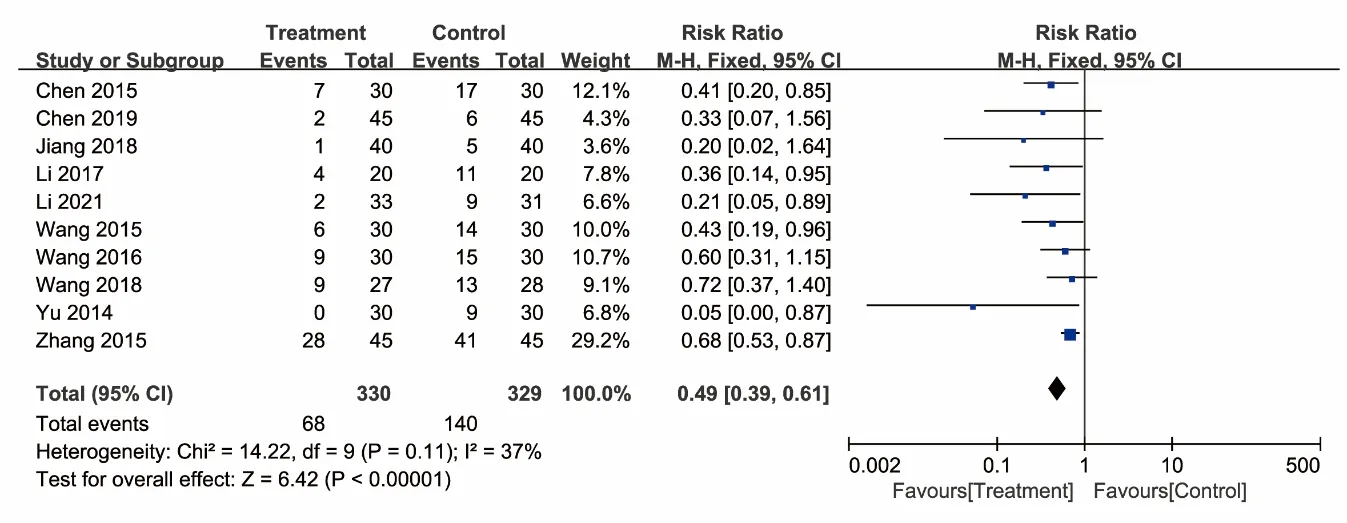
Figure 5 Forest plot:incidence of postoperative nausea and vomiting
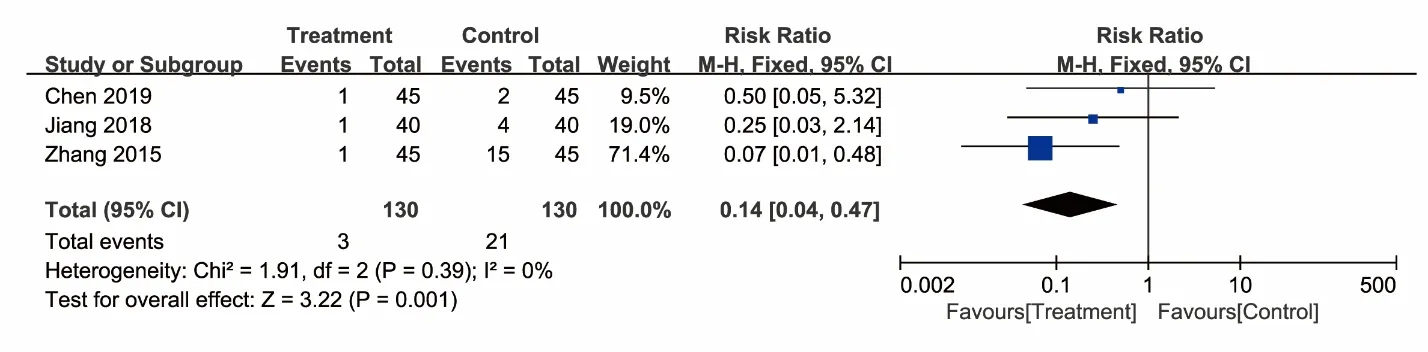
Figure 6 Forest plot:incidence of postoperative dizziness and headache
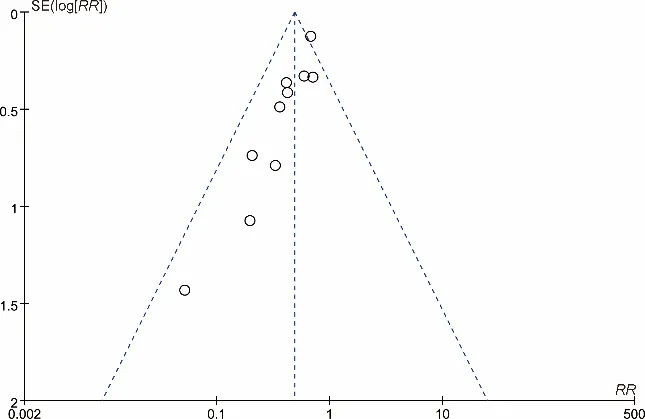
Figure 7 Funnel plot of studies in terms of the incidence of postoperative nausea and vomiting
4.DISCUSSION
Pain after laparoscopic surgery-induced by trauma,inducing ischemia-reperfusion injury,needs an emergency and urgent care.23If not controlled timely,pain after laparoscopic surgery gradually leads to chronic pain through oxidative stress and immune responses.24Acupuncture has been known for its unique advantages in acute or chronic pain treatment.Among the 107 dominant diseases recommended by the World Health Organization for acupuncture,pain-associated diseases account for 43%.25-27Electroacupuncture combines traditional Chinese acupuncture therapy and electronic technology,which produces a sense of “DeQi”viaelectrical stimulation instead of manual acupuncture.It provides a full effect on invigoratingQiand activating blood circulation,dredging collaterals,and relieving pain.Recently,its exact clinical efficacy was verified from research on acupuncture analgesia.28,29Therefore,our study aimed to analyze and explore the clinical efficacy of electroacupuncture to treat pain after laparoscopic surgery and provide new ideas to optimize the clinical treatment.
This Meta-analysis found that compared with routine analgesia therapy,electroacupuncture combined with routine analgesia therapy relieved pain more effectively and safely.For the postoperative 24 h VAS scores,electroacupuncture conducted 24 h before surgery showed no significance on electroacupuncture+routine analgesia therapy.However,it showed a statistical significance in electroacupuncture conducted after surgery,before and after surgery,and in surgery.Acupuncture enhances the function of central opioid genes and receptors and promotes the production and utilization of analgesic substances such as endorphins.It can also inhibit the transmission of pain information,change the nature of pain by integrating neurohumoral and pain modulation systems,weaken the feeling and response caused by pain stimulation and thus play an analgesic role.30The clinical efficacy of electroacupuncture is correlated to time,expressing a process of development,peak,and attenuation.31Electroacupuncture conducted before an operation could not maintain its analgesic effect 24 h after the operation.In intraoperative anesthesia dose,electroacupuncture combined with routine analgesia was also significantly lower than patients receiving only routine analgesia or sham electroacupuncture combined with routine analgesia through subgroup analysis.Electroacupuncture for pain after laparoscopic surgery can reduce postoperative complications and lead to fewer adverse reactions than western medicine.32,33In this study,a total of 12 studies reported the occurrence of adverse reactions.The incidence of adverse reactions,including nausea,vomiting,headache,and dizziness in patients with electroacupuncture combined with routine analgesia was statistically lower.Current evidence suggested that acupuncture is good at pain treatment and controlling nausea and vomiting after laparoscopic surgery,enhancing protective immunity.34-37Thus,electroacupuncture is a necessary adjunct therapy for pain after laparoscopic surgery.
There are some limitations to this study.Firstly,this systematic review had a high risk of bias.Some studies did not clearly describe the random and blinding methods,and the total numbers of RCTs and participants involved were too small to draw concrete conclusions.We suggest that multi-center,large-sample RCTs should be conducted to avoid bias,referring to the recent extension of the Consolidated Standards of Reporting Trials statement for trials of acupuncture interventions.Secondly,there are several problems in reporting outcome indexes of electroacupuncture for pain after laparoscopic surgery.Some studies included in the Metaanalysis did not fully report the VAS scores of patients at different time points postoperatively;thus,the results could not be included in this systematic review to provide a higher level of evidence for clinical trials.Moreover,as a subjective symptom scale,the VAS scores could weaken the credibility of the conclusions regarding electroacupuncture effectiveness.38The construction method of the international core outcome set can be referred to establish the core outcome set with the clinical characteristics of Traditional Chinese Medicine,39providing a complete outcome evaluation system for clinical research on electroacupuncture for pain after laparoscopic surgery.Third,the patients of the included RCTs were from China,where the positive results reports were common,casting some doubt on data validity.All of the limitations indicated a publication bias.Thus,our conclusions should be verified further in the future.
To summarize,electroacupuncture intervention is a safe and effective postoperative analgesia therapy that can relieve pain after laparoscopic surgery,reduce the analgesic drugs intake and the occurrence of related adverse effects.Multicenter,large-sample,welldesigned RCTs should be conducted to validate these findings.In addition,it should also be considered carefully for constructing the core outcome set of clinical research on electroacupuncture treating pain after laparoscopic surgery.This study will provide a solid foundation for higher-quality research in the future.
5.REFERENCES
1.Li L,Tian JH,Tian HL,Sun R,Wang Q,YangKH.The efficacy and safety of different kinds of laparoscopic cholecystectomy:a network Meta-analysis of 43 randomized controlled trials.PLoS One 2014;2:e90313.
2.Li YX,Li SP.Current status of research on analgesia methods after laparoscopic surgery.Shi Jie Zui Xin Yi Xue Xin Xi Wen Zhai 2019;66:50-1.
3.Mitra S,Khandelwal P,Roberts K,Kumar S,Vadivelu N.Pain relief in laparoscopic cholecystectomy-a review of the current options.Pain Pract 2012;12:485-96.
4.Choi GJ,Kang H,Baek CW,Jung YH,Kim DR.Effect of intraperitoneal local anesthetic on pain characteristics after laparoscopic cholecystectomy.World J Gastroenterol 2015;47:13386-95.
5.Wheeler M,Oderda GM,Ashburn MA,Lipman AG.Adverse events associated with postoperative opioid analgesia:a systematic review.J Pain 2002;3:159-80.
6.Chen RD,Tu WZ,Jiang SH.Research progress on the role of purines and their receptors in the analgesic effect of electroacupuncture.Zhong Guo Teng Tong Yi Xue Za Zhi 2012;1:53-6.
7.An LX,Chen X,Ren XJ,Wu HF.Electroacupuncture decreases postoperative pain and improves recovery in patients undergoing a supratentorial craniotomy.Am J Chin Med 2014;5:1099-109.
8.Sun Y,Gan TJ,Dubose JW,Habib AS.Acupuncture and related techniques for postoperative pain:a systematic review of randomized controlled trials.Br J Anaesth 2008;2:151-60.
9.Higgins JPT,Altman DG,Sterne JAC (editors) (2011) Chapter 8:Assessing risk of bias in included studies.In:Higgins JPT,Green S (editors).Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011).The Cochrane Collaboration,2011.Available from URL:www.cochranehandbook.org.
10.Review Manager (RevMan) [Computer program].Version 5.3.Copenhagern:the Nordic Cochrane Centre,The Cochrane Collaboration,2014.
11.Chen M,Teng YJ,Deng CW,Chen C.The influence of acupuncture on adverse reactions and early recovery after laparoscopic hysterectomy.Guangzhou Zhong Yi Yao Da Xue Xue Bao 2019;12:1939-43.
12.Wang J,Fu GQ,Y L,Shen WD,Wang K.Comparative study on the effect of electroacupuncture and morphine intravenous patientcontrolled analgesia on postoperative recovery of patients with laparoscopic cholecystectomy.Shanghai Zhong Yi Yao Za Zhi 2016;9:52-6.
13.Wang XQ,Wu WZ,Zheng M,Li S.The feasibility study of preoperative electroacupuncture on gastrointestinal function in patients undergoing gynecological laparoscopic surgery.Zhen Jiu Lin Chuang Za Zhi 2018;2:35-8.
14.Jiang M,Zhou M,Shen FY.Clinical study of analgesic effect of acupuncture-assisted anesthesia on patients undergoing laparoscopic cholecystectomy-Clinical data of 40 cases.Jiangsu Zhong Yi Yao 2018;3:67-8.
15.Yu GJ,Fu GQ,Li FR,et al.Observation of the analgesic effect of long-stay-needle electrical stimulation for postoperative laparoscopic cholecystectomy.Zhong Guo Zhen Jiu 2014;2:169-72.
16.Sun Y,Zhang DW,Li HF.The influence of electroacupuncture on the rapid recovery of elderly laparoscopic bowel surgery.Shi Yong Yi Xue Za Zhi 2019;11:1837-40.
17.Zhang L,Wu C.A clinical comparative study of two acupuncture methods assisted in patients undergoing laparoscopic cholecystectomy under general anesthesia.Zhong Hua Zhong Yi Yao Xue Kan 2015;4:826-28.
18.Wang YD,Zhou J,Han G,Kong XC,Cao Y,Gong HJ.Observation on the clinical effect of combined acupuncture and medicine anesthesia in laparoscopic cholecystectomy.Zhong Guo Zhong Yi Ji Chu Yi Xue Za Zhi 2015;6:728-30.
19.Ding YH,Gu CY,Shen LR,Chen YL,Shi Z.The influence of different anesthesia methods on the immune function of T lymphocytes in patients undergoing laparoscopic cholecystectomy and the effect of postoperative analgesia.Zhong Guo Zhen Jiu 2011;5:447-50.
20.Chen BN,Zhang FX,Zhang JC,et al.The effect of acupuncture on the early recovery quality of patients after gynecological laparoscopy:QoR-40 scale.Zhong Hua Ma Zui Xue Za Zhi 2015;12:1428-30.
21.Li S,Zheng M,Wu WZ,Guo J,Ji FB,Zheng Z.Effects of electroacupuncture administered 24 h prior to surgery on postoperative nausea and vomiting and pain in patients undergoing gynecologic laparoscopic surgery:a feasibility study.EXPLORENY 2017;13:313-8.
22.Li MJ.Discussion on the clinical effect of Acupuncture Electrical Stimulation on gynecological minimally invasive surgery based on ERAS concept.Nanjing:Nanjing TCM University,2021:15-24.
23.Jin YH.Acute post surgical pain may result in chronic post surgical pain:a systemic review and Meta analysis.Pak J Med Sci 2015;4:833-6.
24.Marks JL,Ata B,Tulandi T.Systematic review and Meta-analysis of intraperitoneal instillation of local anesthetics for reduction of pain after gynecologic laparoscopy.J Minim Invasive Gynecol 2012;5:545-53.
25.World Health Organization (WHO).Acupuncture:review and analysis of reports on controlled clinical trials.Geneva serial online 2003,.cited 2008-07-15;Available from URL:http//apps.who.int/iris/handle/10665/42414.
26.Xie CJ,He XJ.Acupuncture anesthesia combined with cervical plexus anesthesia for 32 cases of thyroid surgery Clinical Observation.Zhong Yi Yao Dao Bao 2007;2:50-2.
27.Zhou J,Shen WD,Li GA,Chi H,Fu GX,Zhu ZM.Severe pulmonary valve stenosis resection under combined acupuncture and anesthesia.Zhong Guo Zhen Jiu 2007;3:203-4.
28.Li MJ,Wei BX,Deng QX,Liu X,Zhu XD,Zhang Y.Effect of electroacupuncture preemptive analgesia on stress response and epidural analgesia of parturient women.Zhen Ci Yan Jiu 2019;10:752-6.
29.Wu JY,Chen B,Zhang XL,Yin P,Xu SF.Effect of Electroacupuncture on postoperative analgesia of mixed hemorrhoids.Shanghai Zhen Jiu Za Zhi 2016;6:680-3.
30.Zhu XM,Yin LH.Research trend of acupuncture analgesia mechanism in the new period.Zhong Guo Zhong Yi Ji Zheng 2012;1:33-5.
31.Dong Q.Time-effect relationship of acupuncture treatment for diabetic peripheral neuropathy.Nanjing Zhong Yi Yao Da Xue Xue Bao 2011;4:3.
32.Ding Y,Su SY,Li YL,et al.Effects of electroacupuncture preconditioning on cardiac function in patients undergoing laparoscopic myomectomy.Zhen Jiu Lin Chuang Za Zhi 2014;7:4-6.
33.Ye CH,Huang FQ.The effect of electroacupuncture at Neiguan on nausea and vomiting after gynecological laparoscopy.Shi Jie Zui Xin Yi Xue Xin Xi Wen Zhai 2019;93:223-4.
34.Alizadeh R,Esmaeili S,Shoar S,Bagheri HS,Shoar N.Acupuncture in preventing postoperative nausea and vomiting:efficacy of two acupuncture points versus a single one.J Acupunct Meridian Stud 2014;2:71-5.
35.Lin Z.Effect of acupuncture combined with bladder function training on the recovery of bladder function after hysterectomy.Zhong Guo Zhong Yi Yao Ke Ji 2019;3:460-2.
36.Qiu XZ,Cai LY,Zhang JN,Zhou HM,Jiang CH.Research progress of the application of acupuncture-assisted anesthesia in the perioperative period and organ protection.Shanghai Zhong Yi Yao Za Zhi 2020;1:92-6.
37.Wang NK,Qu Y,Qing W,et al.Combined acupuncture and generalanesthesia on immune and cognitive function in elderly patients following subtotal gastrectomy for gastric cancer.Oncol Lett 2018;1:189-94.
38.Hu JY,Qiu RJ,Li XY,Shang HC,Tian GH.Research ideas on multidimensional evaluation methods of clinical effects of Traditional Chinese Medicine in treating chronic pain.Shi Jie Ke Xue Ji Shu-Zhong Yi Yao Xian Dai Hua:l-6.
39.Qiu RJ,Li M,Han SJ,et al.Interpretation of COMET Handbook 1.0 and its enlightenment on constructing core index set of clinical research of Traditional Chinese Medicine.Zhong Guo Xun Zheng Yi Xue Za Zhi 2017;12:1482-8.
杂志排行

Journal of Traditional Chinese Medicine的其它文章
- Effectiveness of redcore lotion in patients with vulvovaginal candidiasis:a systematic review and Meta-analysis
- Efficacy and safety of external application of Chinese herbal medicine for psoriasis vulgaris:a systematic review of randomized controlled trials
- Effect of astragaloside IV on the immunoregulatory function of adipose-derived mesenchymal stem cells from patients with psoriasis vulgaris
- Shenqihuatan formula (参七化痰方) reduces inflammation by inhibiting transforming growth factor-beta-stimulated signaling pathway in airway smooth muscle cells
- Drug response biomarkers of Pien Tze Huang (片仔癀) treatment for hepatic fibrosis induced by carbon tetrachloride
- Wenshen Yangxue decoction (温肾养血方) promotes follicular development in aged female mice via stimulation of the silent information regulator 3/forkhead transcription factor O1 3a pathway