Active video games in fully immersive virtual reality elicit moderate-to-vigorous physical activity and improve cognitive performance in sedentary college students
2022-04-18CioVictorSousJungyunHwngRominCrerPerezAustinFernndezAikMiswKelseyNewhookAmyShirongLu
Cio Victor Sous ,Jungyun Hwng ,Romin Crer-Perez ,Austin Fernndez ,Aik Misw ,Kelsey Newhook ,Amy Shirong Lu ,*
a Health Technology Lab,College of Arts,Media and Design,Bouv´e College of Health Sciences,Northeastern University,Boston,MA 02115,USA
b Department of Aging and Geriatric Research,University of Florida,Gainesville,FL 32603,USA
Abstract
Keywords:Active video game;Cognitive performance;Mnemonic similarity test;MVPA;Virtual reality
1.Introduction
An insufficient level of physical activity(PA)is a major contributor to multiple non-communicable diseases,including type 2 diabetes,obesity,and cardiovascular disease.1Researches have shown that active video games(AVGs)may induce moderate-to-vigorous PA(MVPA)in adults and children.2Current U.S.PA guidelines recommend at least 150-300 min/week of moderate-intensity or 75-150 min/week of vigorous-intensity aerobic PA,3yet few individuals meet this guideline.4Sedentary behavior and low levels of PA are prevalent in college students due to class attendance and study sessions at the library as well as screen media engagement(i.e.,smartphones,video games,or computers).5,6Low PA and high sedentary behavior earlier in adulthood are strong determinants of the same behaviors in later life,along with an increased likelihood of cardiovascular disease.7Therefore,identification of strategies to increase MVPA in the young adult population is crucial.
AVG constitutes an important option in terms of exercise and eliciting MVPA.This is especially true in times of social isolation,such as the current coronavirus disease 2019 pandemic,during which more traditional methods for increasing PA(i.e.,outdoor running,resistance exercise in the gym,in-person yoga classes,and indoor cycling)are unavailable or represent an additional risk of infection.Additionally,compared to conventional methods of inducing PA,AVG elicits higher levels of motivation and engagement.8For instance,well-designed video games can create a sense of flow and immersion by incorporating important parts of game engagement,such as discovery,role playing,mastery,and control.9,10These aspects,along with AVG-elicited feelings of competence,autonomy,and immersion,are key contributors to a greater motivation to play video games.8,10During the last 2 decades,AVGs have evolved rapidly,and the recent development of virtual reality(VR)provides a novel platform for active gaming.11An immersive VR headset with image and sound input entirely cocoons the user within a computer-generated world.12VR can be AVR,which requires lower-,upper-,or whole-body movements,or sedentary VR(SVR),which requires only finger movements.These are likely to result in different levels of PA.Also,a VR setting may yield a better player game experience than the non-VR setting,13i.e.,its use has been found to elicit greater immersion,flow,positive affect,and empathy while lowering negative affect.13These aspects could help increase game engagement and,for players using AVR,time spent in MVPA.
A fully immersive VR(3-dimensional VR)is an immersive display device for individual immersion.14When immersed in a VR environment,the player can interact in real-time with objects and avatars.14With AVR,this complete immersion might produce motion sickness because of the mismatch between an individual’s visual and vestibular systems.15Research found that adults using fully immersive VR are at increased risk of experiencing motion sickness due to increased postural instability.16In such cases,the motion required to play the AVG in VR may lead to decreased game engagement.17
Hip-worn accelerometers,18-20the recommended method for assessing PA in free-living conditions,21are frequently employed in studies of AVG-induced MVPA.22Due to the lack of uniform AVG requirements for body movements and player body-movement types,additional physiological measurement methods(e.g.,heart rate)should be considered when evaluating activity elicited by AVG play.Using multiple sensing measurement methodologies may improve the validity of MVPA measurement during AVG play,23especially in a VR environment.
Researchers have demonstrated that a single AVG play session elicited cognitive benefits in healthy adults24and children.25Cognition is defined as the actions of the brain involved in understanding and functioning in an external environment.26While cognitive performance has been shown to predict real-world functionality and occupational performance,27it naturally decreases across the lifespan of an individual and is associated with several age-related comorbidities.28Thus,activities that acutely boost cognition,such as AVG play,may attenuate the natural age-related cognitive decline in children and young adults,thereby preventing it in older adults.29Reports of comparisons of the effects of AVG,sedentary games,and treadmill exercise indicate that AVG elicits benefits for focus and concentration that are similar to those of treadmill exercise but with lower exertion levels and a higher perception of fun.24A substantial body of literature indicates that exercise can elicit cognitive improvement,possibly due to an increased heart rate as well as an increase in circulating catecholamines and brain-derived neurotrophic factor.30Additionally,a comparison of the effects of a desktop game vs.immersive SVR indicated that only the latter elicited a greater amount of working memory.31Thus,immersive VR coupled with exercise could result in a boost in cognitive performance.
We investigated the use of AVR as an MVPA inducer for sedentary college students and validated the outcomes using 2 methods of PA assessment.We also compared the cognitive performance effects of AVR vs.SVR in college students.We hypothesized that AVR would yield greater MVPA,regardless of the PA monitoring method,and greater cognitive benefits than either SVR or control.We examined the difference in motion sickness and game engagement as part of an exploratory analysis.
2.Methods
2.1.Ethical concerns
The Institutional Review Board at the Northeastern University approved our study.
2.2.Sample
We invited participants via web advertisements and posters displayed in common areas on campus and nearby areas.Inclusion criteria were:low levels of PA(weekly reported total PA metabolic equivalent of task(MET)minutes≤1500 min as calculated using the International Physical Activity Questionnaire-Short Version);32aged between 20-29 years;no cardiovascular,cerebrovascular,or neurological diseases,no attention disorders or physical disability;never used tobacco(as both its usage and deprivation impact cognitive function);33,34English speaking;and never previously played the video games we used.
We recruited 306 students who indicated their interest by completing an online pre-screening questionnaire,including the International Physical Activity Questionnaire-Short Version.32Most of these students were excluded due to reported high PA levels(weekly reported total PA MET minutes>1500 min),leaving 66 who met our inclusion criteria and were invited to the initial screening and first visit.We sent ineligible responders a“thank-you”e-mail for their interest.Of the 66 students,34 completed all 3 visits,of whom 5 were excluded due to invalid heart rate data(due to device misplacement or malfunction).Thus,our final sample size was 29 participants.
2.3.General procedures
During the first visit,participants signed a written informed consent and provided their demographic information via an online questionnaire.The research assistants measured their height and weight using a stadiometer(ShorrBoard,Weigh and Measure,LLC,Olney,MD,USA)and a calibrated scale(Seca GmbH,Hamburg,Germany).Three visits(AVR,SVR,and control session(CS))were required of each participant and administered in random order based on Microsoft Excel’s(Microsoft,Redmond,WA,USA)random list function.Each visit was scheduled,on average,between 96 h and 120 h apart.
During each session(AVR,SVR,and CS),participants were not allowed to use their mobile devices(smartphones,tablets,or laptops),perform any other activity,or fall asleep.We attached an accelerometer to their non-dominant hip(wGT3x-bt;ActiGraph,Pensacola,FL,USA)and an heart rate(HR)band(Polar H7;Polar,Kempele,Finland)to their chest.For AVR and SVR,participants first obtained instructions on how to play the game via a tutorial.They then performed one of the three 20-min session assignments by playing the AVR or SVR or by sitting quietly(CS).Next,participants completed an abbreviated version of the game experience questionnaire (GEQ).35We then cognitively assessed them using the mnemonic similarity test(MST).36Participants completing all 3 visits received a USD45“thank-you”gift card.
2.4.AVR and SVR
For both AVR and SVR sessions,we used the Vive Pro system(HTC,New Taipei,Taiwan,China).The Vive Pro headset features high-resolution displays at 1440×1600 resolution per eye,along with a second outward-facing camera,attachable headphones,a microphone for noise cancellation analysis,and a wireless adapter for untethered play.They are lightweight(803 g)and have a sizing dial.
In the AVR session,participants played Beat Saber,37a rhythm-based AVG in which the participant uses virtual lightsabers(laser swords)to cut through blocks(upper-body movement)or to evade large blocks by moving to either side or crouching(whole-body movement).The blocks move in the player’s direction according to the rhythm of the song being played in the background.Since all participants played Beat Saber for the first time in our study,we created a song list that began with an easier song to ensure the participants could better understand the game flow as well as the game instructions.The difficulty gradually increased with each subsequent song.The playlist was as follows:USD100;Country Roads;Escape;Beat Saber;Level Insane;Turn Me On;Elixia;Commercial Pumping;Unlimited Power;and Balearic Pumping.
In the SVR session,participants played Thumper,38another rhythmic game in which players guide their character and hit“notes”in synchrony with background music.In this game,players use an Xbox One controller(Microsoft,Redmond,WA,USA)while seated and are only required to move their fingers.
Although Beat Saber and Thumper are both rhythm games and share similar visual characteristics and audio styles,they differ significantly in the amount of PA required to play them.
During the CS,the participant remained seated without any task.
2.5.PA assessment
ActiGraph accelerometer devices are widely used to assess individual levels of PA in children and young adults.39-41In this study,we attached an ActiGraph GT3x-bt(ActiGraph)to each participant’s non-dominant hip and initialized the device at a 30-Hz sampling rate.The ActiGraph triaxial accelerometers(ActiGraph)assessed PA by providing measures of acceleration from the subject’s movement in 3 individual axes(anterior-posterior,vertical,and medial-lateral).With these measures we were able to obtain the frequency,duration,and intensity of their physical movement.23
We also attached a Polar HR band(Polar)to each participant’s chest behind a privacy curtain.We used heart rate measurements only as a measure of the intensity of PA,23including the linear and proportionate increase corresponding to more intense movement.42
We downloaded the activity monitor data via ActiLife software(Version 6.13.2;ActiGraph,Pensacola,FL,USA)and converted it into a triaxial form for activity counts in order to quantify the amplitude and frequency of detected accelerations at a 1-s epoch.A 1-s epoch is the most appropriate epoch length to detect short bursts of intense PA and may be the best choice for examinations of intermittent PA.40We also used the ActiLife software(Version 6.13.3;Acti-Graph)to download the HR measurement data,which we analyzed at 1-min intervals.
We used the following cut-off points to estimate the time spent in light,moderate,and vigorous PA according to the hip accelerometers:light,<760 counts/min;moderate,=760-5724 counts/min;and vigorous,>5724 counts/min.43We estimated HR-based MVPA using the maximum HR(HRmax)together with the relative HR intensity cut-offs set by the American College of Sports Medicine:light PA<64%HRmax;moderate PA=64%-76%HRmax;and vigorous PA>76%HRmax.44
2.6.Motion sickness and GEQ
In the AVR and SVR sessions,we asked participants to complete an abbreviated version of the GEQ,in-game GEQ,35and a motion sickness questionnaire.45The motion sickness questionnaire is a 15-item,10-point Likert-style scale(0=not at all;9=severely).Sample items included“I felt sick to my stomach”,“I felt queasy”,and“I felt dizzy”.
We used the in-game GEQ35to minimize participant burden while obtaining as much information as we could.The original GEQ contained 33 items,measuring 7 components of the game experience,including immersion and flow;more specifically,immersion was measured with 6 items and flow was measured with 5 items in this version of the GEQ.The in-game GEQ,however,only contained 14 items,with 2 items measuring each of the 7 components.Since immersion and flow are highly relevant to our project’s scope and also represent the core definition of VR,14we decided to use the full measure of these 2 components from the original GEQ Module by including the 4 items for immersion and 3 items for flow that had been omitted from the in-game GEQ.To report their gaming experience, participants responded to our 21-item questionnaire;each item had a 5-point Likert-style scale response(0=not at all;4=extremely).This information was used to assess competence,sensory and imaginative immersion,flow,tension,challenge,and positive and negative affect.
Sample items for immersion included“It was aesthetically pleasing”,“I felt imaginative”,“I felt that I could explore things”,and“It felt like a rich experience”.Sample items for flow included“I lost track of time”,“I was deeply concentrated in the game”,and“I lost connection with the outside world”.
2.7.MST
The MST is a robust behavioral measure of recognition(REC)memory with strong demands on pattern separation processes;it has been used in various populations across the lifespan.46-49The MST task assesses REC memory performance for objects using the traditional targets and unrelated foils plus similar lures varied along several dimensions.50PA,especially MVPA,has been found to improve respondents’MST performance.51
Each MST testing session took about 15 min to complete in 2 phases during each of the 3 visits:encoding and retrieval(Fig.1).In the encoding phase,the participants classified each item in a sequence of 128 objects to be indoor or outdoor(2 s per object presentation with 0.5 s interstimulus interval).There was no right or wrong answer in this phase.In the retrieval phase,the participants classified each item in a sequence of 192 objects to be old,new,or similar.Of the 192 objects,64 were items seen in the encoding phase(target),64 were similar to items seen in the encoding phase(lure),and 64 were new objects(foil).All object images were randomly selected from the MST Image Set F(https://faculty.sites.uci.edu/starklab/mnemonic-similarity-taskmst/),which was a recent expansion of the original sets with better graphic quality and ease of application.50
The raw data from each of the sessions are present in Table 1.From the raw MST data,we derived the Lure Discrimination Index as the difference between the rate of“similar”responses for the lure items minus“similar”responses for the foils(to correct for any response biases).Wecalculated the REC for repeat items as the difference between the rate of“old”responses for target items minus“old”responses for the foils.36

Table.1 Raw data of MST after each session(n=29)(mean±SD).
2.8.Statistical analysis
All data are expressed as mean±SD.All GEQ-derived variables were scored and analyzed per the developer’s recommendation.35Immersion(Cronbach’sα>0.79),flow(Cronbach’s α>0.85),and motion sickness(Cronbach’sα>0.95)were calculated by averaging their respective items(immersion:6 items;flow:5 items;motion sickness:15 items).All other constructs(e.g.,challenge,competence)were measured by 2 items each and averaged as suggested.35
We used a general linear model(GLM:two-way analysis of variance)with sessions(CS,SVR,and AVR)and methods(hip,HR)as random factors to analyze MVPA.We used repeated-measures analysis of variance to determine whether there was a session effect on HR and MST scores.Bonferroni’s post hoc was used to identify specific differences among the sessions.

Fig.1.Mnemonic similarity test.

3.Results
The average body mass index of the participants falls within the normal weight category(<25 kg/m2).All reported insufficient weekly MET to be considered physically active(Table 2).
The GLM for MVPA showed a significant method-effect(F=48.9;p<0.001),session-effect(F=168.9;p<0.001);and interaction effect of method×session(F=37.7;p<0.001).Post hoc analysis identified the AVR session as inducing higher MVPA than CS or SVR across the 2 PA assessment methods(Table 3).HR showed a significant session-effect(F=29.1;p<0.001)with higher values in the AVR session after a post hoc analysis(Table 3).
The GLM for the MST identified no significant session-effect for Lure Discrimination Index(F=0.06;p=0.909),and a trend session-effect for REC(F=3.69;p=0.057).A post hoc analysis for the REC showed a trend of higher scores following AVR than SVR(p=0.084)(Fig.2).
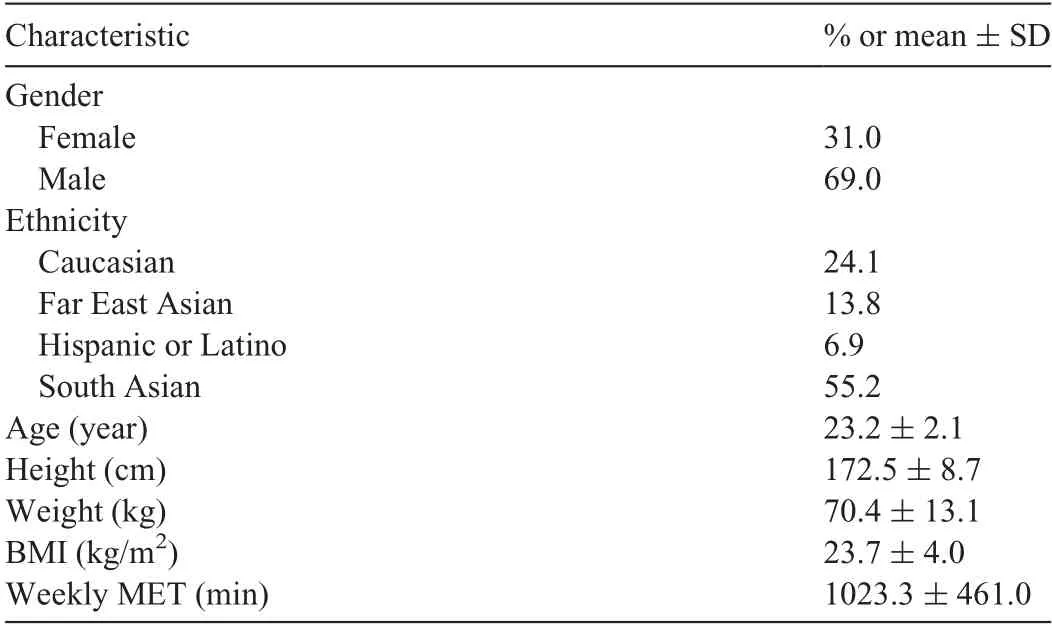
Table 2 Demographic and anthropometric characteristics of the sample(n=29).

Table 3 Time spent in MVPA and average HR assessed through hip-worn accelerometers and HR band(mean±SD).

Fig.2.LDI and REC from the MST after CS,SVR,and AVR.Borderline session-effect for REC(p=0.084).AVR=active virtual reality;CS=control session;LDI=Lure Discrimination Index;MST=mnemonic similarity test;REC=recognition;SVR=sedentary virtual reality.
The motion sickness scores were relatively low and not different between the AVR and SVR conditions.The GEQ scores showed significantly higher immersion(p<0.05),challenge(p<0.05),and positive affection for AVR than SVR(p<0.01),with moderate-to-large effect sizes(Table 4).

Table 4 Motion sickness,competence,sensory and imaginative immersion,flow,tension,challenge,positive affect,and negative affect after active and sedentary VR(mean±SD).
4.Discussion
We elicited MVPA via AVR among sedentary young adults without significantly increasing motion sickness.The within-subject design and inclusion of a control condition add to the robustness of the findings.AVR could thus be an alternative to traditional exercise methods intended to increase PA in young adults.AVR resulted in higher immersion,challenge,and positive affect than did SVR,although the game experiences did not seem to mediate the relationship between VR type and MVPA.AVR marginally increased the REC score from MST,whereas SVR did not.
Researchers have demonstrated that fully immersive VR can reduce pain scores as a distraction,53increase knowledge retention as an educational method,54and improve cardiovascular parameters as a method of exercise.55We are among the first to demonstrate that a fully immersive AVR game can elicit MVPA in young adults with better game engagement in several dimensions and without significantly increasing motion sickness.Our results indicate that the time spent in MVPA represents around 40%of the total play time,a considerable portion(5-8 min out of 20-min play time).To induce health-related outcomes,it is recommended that an adult should engage in a minimum of 200 min of MVPA every week.56Additional physical exercise activities might be needed to achieve weekly MVPA goals.
Although researchers have investigated AVG-induced MVPA in college students,57research on PA via AVR is scarce.An investigation of the effect of a 15-min session of AVR exergame indicated that,regardless of age,gender,and PA level,AVR elicited high levels of perceived exertion and HR.19An examination of HR during 2 types of AVR using an omni treadmill vs.a flight simulator indicated that the omni treadmill produced 80.6%of HRmaxat the recommended PA guidelines.58It is likely that VR with an enhanced technological interface could induce more intense PA via a more immersive experience.
Similar to previous researchers who found that a VR setting improves the player’s experience more than a non-VR setting does,13we found that an AVR elicits greater immersion,challenge,and positive affect than an SVR does.Immersive hardware with well-developed software may result in a better game experience.59,60For AVR,this experience might yield increased play with more MVPA.AVR games eliciting a better game experience could benefit the users with PA-derived positive health outcomes beyond entertainment.While both VR sessions elicited some levels of challenge and immersion,the physical exercise component in the AVR may create another level of role playing and game goals,further increasing perceived immersion and challenge.The challenge construct in video games contains“goals”and“feedback”.61Although the goal-setting can be utilized for behavioral change,its role in motivating exergame play remains unclear.62The motion sickness measure produced relatively low scores across both game conditions.This could potentially alleviate some VR by-standers’concerns.
Studies of time spent in MVPA during AVG play using multiple sensors are scarce.To our knowledge,no one has studied immersive VR.In one study,hip-worn accelerometers used to assess time spent in MVPA during two 20-min Xbox 360 AVG play sessions indicated an average of 10.7 min of MVPA—approximately 50%of playing time.57MVPA,measured through hip-worn accelerometer and HR band,was estimated in 40%-50%of the play session,corroborating our findings.57Another investigation of time spent in MVPA used wrist and hip accelerometers in a 30-min AVG play session on Xbox Kinect and reported 29.9 min vs.30.0 min of MVPA,respectively.19As the wrist accelerometer records accelerations of the forearm,indicating a large number of upper-body movements,63this could lead to overestimated PA measures.That is,while hip-worn accelerometers may not record the upper-movements used in many AVGs,wrist-worn accelerometers may overestimate PA during AVG play.Thus,in addition to PA monitoring,physiological measures(e.g.,HR,oxygen uptake)should be monitored during AVG sessions to better assess exercise intensity.
The effects of AVG on cognitive function are evident in older adults64and children.25The use of active games in AVR is scarce,and no one has investigated the use of immersive AVR to induce MVPA among young adults.Research indicates that immersive VR alone has the ability to boost cognitive performance in people with cognitive impairment.65,66This is not reflected by our findings,which showed no difference between SVR and control.However,most studies that used non-exercising VR applications to improve cognition used a software package or specialized game developed for cognitive improvement in populations with cognitive deficit.65-67Our study was conducted among young adults using a commercially available entertainment VR game that does not target cognitive improvement.Specifically,with regard to MST,researchers have demonstrated an age-related deficit in cognitive performance.36This means that our young adults should have performed excellently on MST and,thus,created a ceiling effect from the beginning.
Nevertheless,AVR still elicited a borderline better REC score than CS or SVR.Physical fitness is associated with better baseline MST scores in young adults,68though whether long-term AVR play can improve baseline MST scores remains to be studied.Additionally,our results show that the exercise component in AVR might contribute to its ability to elicit more significant cognitive improvement than SVR.These findings are in line with previous research indicating that an acute session of moderate exercise can improve cognitive performance.30However,specifically regarding memory,the literature is not consistent with respect to positive exercise-induced effects.69,70
AVR and SVR games may elicit MVPA and cognitive benefits differently,but our evaluations were limited to one game of each type.Our study was conducted in a laboratory setting with a preset time limit and preselected games.Investigating VR gameplay in a free-living environment for players across the developmental span would afford better generalizability of similar evaluations along with clinically relevant outcomes.Future comparisons of the ability of different AVR games to affect MVPA and cognitive performance,and their potential long-term effects on players,should be conducted.Additionally,the fact that participants played different games in AVR and SVR sessions does not rule out the possibility that some of the game design characteristics,rather than PA,elicited the differing physiological and cognitive responses.Nevertheless,both are rhythm games with similar visual and audio style characteristics,leaving the active capacity as the key difference.
5.Conclusion
AVR feasibly elicits MVPA,which we validated through hip-worn accelerometers and HR monitors,without a significant increase in motion sickness.AVR also induced a better game experience and better borderline cognitive performance than did SVR in young adults.We hope our results may inform future fully powered explorations and well-developed interventions to maximize the potential physical and cognitive health benefits of fully immersive VR.
Acknowledgments
The authors thank the Health Technology Laboratory members,including Dar Alon for her help and effort with data collection and data preparation.This study was supported in part by a grant from the National Institute of Diabetes and Digestive and Kidney Diseases(R01DK109316,principle investigator:ASL),and by the College of Arts,Media,and Design,Bouv´e College of Health Sciences at Northeastern University,Boston,MA,USA.
Authors’contributions
CVS contributed to data collection,data analysis,interpretation of results,and wrote the first draft of the manuscript;JH participated in the design of the study and manuscript preparation;RCP,AF,AM,and KN participated in data collection and contributed to data preparation;ASL participated in the design of the study,supervised the study data collection,and contributed to data analysis,results interpretation,and manuscript preparation.All authors have read and approved the final version of the manuscript,and agree with the order of presentation of the authors.
Competing interests
The authors declare that they have no competing interests.
杂志排行

Journal of Sport and Health Science的其它文章
- Acceptability,usefulness,and satisfaction with a web-based video-tailored physical activity intervention:The TaylorActive randomized controlled trial
- Effects of a remote,YouTube-delivered exercise intervention on young adults’physical activity,sedentary behavior,and sleep during the COVID-19 pandemic:Randomized controlled trial
- Teen reactions to a self-representational avatar:A qualitative exploration
- Situational interest impacts college students’physical activity in a design-based bike exergame
- Effect and feasibility of wearable physical activity trackers and pedometers for increasing physical activity and improving health outcomes in cancer survivors:A systematic review and meta-analysis
- The effects of resistance training on muscular strength and hypertrophy in elderly cancer patients:A systematic review and meta-analysis