Efficacy and Safety of Wuling Powder and Western Medicine in Treatment of Hyperuricemia: A Meta-analysis of Clinical Trials
2021-10-21QiushuangLIZheLIQingyuXIEKunZHANGGuangRONGPingxinHAN
Qiushuang LI, Zhe LI, Qingyu XIE, Kun ZHANG, Guang RONG*, Pingxin HAN
1. Biomedicine Department of Beijing City University, Beijing 100094, China; 2.Dongzhimen Hospital, Beijing 100700, China; 3. Chengdu Yilian Technology Co., Ltd., Chengdu 610041, China
Abstract [Objectives] To compare the clinical efficacy and safety of Wuling powder and conventional Western medicine for lowering uric acid in the treatment of hyperuricemia. [Methods] Databases such as CNKI, Wanfang Data, VIP Database, PubMed, Cochrane library and Embase, were retrieved, and comparative experiments of efficacy (serum uric acid level) and safety (incidence of adverse reactions) between Wuling powder (used singly or combined with other prescriptions) and conventional Western medicine in the treatment of hyperuricemia were included, and effect size was pooled with Revman 5.3. [Results] A total of 11 articles, involving 817 patients, were included, and their research quality was evaluated to be low. In terms of overall effect, Wuling powder (used singly or combined with other prescriptions) was better than the control drug in reducing serum uric acid level, but the difference was insignificant [SMD=-0.37, 95% CI (-0.90, 0.16)]. The heterogeneity between studies was high. The incidence of adverse reactions in the experimental group was significantly lower than that in the control group. Subgroup analysis shows that Wuling powder combined with other prescriptions was better than the control drug in reducing serum uric acid level [SMD=-0.37, 95% CI (-0.90, 0.16), P=0.17], and the heterogeneity was reduced. [Conclusions] Wuling powder combined with other prescriptions is better than conventional Western medicine in the treatment of hyperuricemia, and has better safety. Wuling powder alone is not as effective as conventional Western medicine. It is suggested that in clinical work, doctors may need to modify the prescription of Wuling powder. The low quality of the literature supporting this conclusion suggests that this evidence should be interpreted with caution.
Key words Hyperuricemia, Wuling powder, Meta-analysis
1 Introduction
Hyperuricemia (HU) is a pathological state that occurs when the level of serum uric acid (SUA) increases due to abnormal production and/or excretion of SUA, and exceeds a critical value[1]. In recent years, the incidence rate of HU has been increasing in China year by year, 21.7% in men and 8.6% in women, equal to the levels of developed countries[2]. HU is an independent risk factor leading to labor loss. It is also related to the occurrence of atherosclerosis[3], myocardial infarction[4], diabetes[5]and hypertension[6]. HU is a sufficient and non-necessary condition for gout[7]. Among HU patients, 18.8% will progress to gout within five years[8]. The acute onset of gout has a clear causal relationship with SUA level fluctuations[9]. Therefore, controlling the level of SUA is a key for the treatment of gout, and may improve the above-mentioned related diseases or adverse events.
Conventional urate lowering therapies (ULTs) include allopurinol, benzbromarone and febuxostat. Studies have shown that the SUA-lowering effect of the three is satisfactory. However, allopurinol may cause severe allergic reactions such as Steven-Johnson syndrome and toxic epidermal necrolysis[10].A study[11]has shown that such allergic reactions are closely related to the genotype of commonHLA-B*5801 in Asians. Benzbromarone may also be hepatotoxic[12].Febuxostat can be used in cases of allopurinol allergy and renal insufficiency, but the price is very expensive[13]. Generally, it is only used when the patient cannot tolerate allopurinol[14]. Therefore, research on new methods to reduce SUA has very important clinical and social significance.
Wuling powder is first recorded inTreatiseonFebrileandMiscellaneousDiseases, and it is widely used in the clinical treatment of HU[15]. Clinical study[16]has found that Wuling powder and its modified prescriptions may have a certain effect in reducing SUA. However, the study has a small sample size and insufficient test power, and the result may be positive due to sampling error. In addition, some patients in the study have differences in baseline disease, and the combination medication situation and medication time of the experimental group are different, making it difficult for clinicians to obtain intuitive conclusions to guide clinical practice. To this end, this research intended to carry out a meta-analysis to explore whether Wuling powder and its modified prescriptions actually have the effect of reducing SUA.
2 Materials and methods
2.1 Retrieval strategyThe databases of CNKI, Wanfang Data, VIP Database, PubMed, Embase and Cochrane were retrieved, and the retrieval time was from the establishment of each database to December, 2019. Taking CNKI as an example, the retrieval strategy for Chinese databases was as follows: (AB=痛风 or AB=痹症 or AB=痹证 or AB=白虎历节 or AB=历节 or AB=高尿酸血症) and FT=五苓散 and (FT=临床观察 or FT=队列研究 or FT=疗效观察 or FT=对照); and taking PubMed as an example, the retrieval strategy for English databases was as follows: 1. exp gout/; 2. hyperuricemia$.tw.; 3. 1 or 2; 4. wu ling san.tw.; 5. wu lingsan.tw.; 6. wulingsan.tw.; 7. wu-ling- san.tw.; 8. $wu-ling-san.tw.; 9. wu-ling-san$.tw.; 10. or/4-9; 11. 3 and 10; 12.randomized controlled trial.pt.; 13. controlled clinical trial.pt.; 14. randomized.ab.; 15. placebo.ab.; 16. drugtherapy.fs.; 17. randomly.ab.; 18. trial.ab.; 19. groups.ab.; 20. or/12-19; 21. (animals not (humans and animals)).sh.; 22. 20 not 21; 23.11 and 22. Other data retrieval was adjusted accordingly.
2.2 Inclusion and exclusion criteria
2.2.1Inclusion criteria. (i) Article in which the subject is clearly diagnosed as HU; (ii) Intervention measures: patients in the control group of the article need to use at least one of the urate lowering therapies (alopurinol, benzbromarone and febuxostat), and patients in the treatment group should use Wuling powder singly or in combination with other Chinese medicine prescriptions (Single use of Wuling powder refers to using Wuling powder original prescription or modifying the prescription simply based on TCM syndrome differentiation. Combined use of Wuling powder and other Chinese medicine prescriptions refers to using Wuling powder combined with other prescriptions or Wuling powder-like prescriptions[17], and none Western medicine that has a direct effect on lowering uric acid is taken. If the treatment group and the control group evenly take a certain non-uric acid-lowering drug on the basis of Wuling powder or its combination with other prescriptions as the basic treatment, and the change in the observed effect of the drug is offset between the two groups, the article can be included).(iii) Outcome indicators: the outcome indicators in the article should include at least one of the following indicators, SUA and overall effect. (iv) Control trials that meet the above intervention measures and outcome indicators.
2.2.2Exclusion criteria. (i) Animal experiments, expert experience, case reports,invitroexperiments,etc.; (ii) Clinical study without a control group; (iii) Clinical research on combined use with other Western medicines except western medicine for lowering uric acid;(iv) Repeated publication; (v) Gout complicated by other diseases; (vi) The outcome indicator of overall effect is mixed with non-SUA evaluation factors, such as the patient’s pain level, and the overall effect cannot be extracted through data processing; (vii) The original research is not standardized and has obvious errors; (viii) Research for which data cannot be extracted; (ix) Non-Chinese and non-English literature.
2.3 Data extractionTwo reviewers cross-screened the literature, read the titles and abstracts, and excluded articles that did not meet the inclusion criteria. Then, they read through the full text of the articles that might meet the inclusion criteria. The results obtained by the two were checked, and if there was a dispute, a third party was invited to make a ruling.
2.4 Outcome indicators(i) Main outcome indicator: SUA. (ii) Secondary outcome indicator: overall effect. Article including at least one of the above indicators was included.
2.5 Quality evaluationAccording to the bias risk evaluation tool of Cochrane Reviewer’s Manual 5.1.0[18], the bias risk of the included studies was evaluated, including (i) whether the method is randomized; (ii) whether the allocation is hidden; (iii) whether there is a reasonable blinding method for participants and implementers; (iv) whether there is a reasonable blinding method for the outcome assessor; (v) whether the result data is incomplete, and whether to conduct loss to follow-up/withdrawal and intention analysis; (vi) whether there is selective reporting bias, and whether to report adverse reactions, uric acid value and other results; (vii) other sources of bias, such as the source of funds. The above items were evaluated by two persons synchronously, and if there was dispute, a third party was invited to make a ruling.
2.6 Statistics and analysisMeta-analysis of outcome indicators was performed using Revman 5.3. Count data are expressed using relative risk (RR, risk ratio) and 95% confidence interval (95%CI), and measurement data are expressed using standard mean difference (SMD) and 95%CI. A heterogeneity test was performed on the included data. WhenI2≤50%, the heterogeneity is considered acceptable, and the fixed effects model is used; and whenI2>50%, the heterogeneity is considered large, and the random effects model is used[19]. When the random effects model was still highly heterogeneous, subgroup analysis was tried (if the number of articles actually included in a certain index was less than 2, the index would not be subjected to subgroup analysis) to explain the source of heterogeneity. The analysis result is shown in a forest plot. If the number of articles ≥ 10[20], Stata 12.0 was used to draw a funnel chart and perform Egger[21]and Begg[22]tests to quantitatively evaluate publication bias. WhenP≥0.1 in the test result, it is not enough to prove that the research has publication bias[23].
3 Results and analysis
3.1 Search resultsAccording to the retrieval strategy, a total of 409 articles were obtained, including 352 articles in CNKI, 49 articles in Wanfang Data, and 8 articles in VIP Database. None related article was retrieved in PubMed, Embase and Cochrane Library. After eliminating 21 duplicate articles and 377 articles based on the reasons in Fig.1, 11 articles were finally included[24-34]. The literature retrieval and screening process is shown in Fig.1.
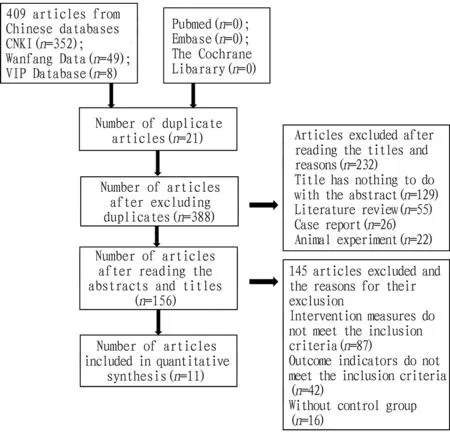
Fig.1 Flow chart of literature retrieval
3.2 Features of included literatureThe basic characteristics of the included literature are shown in Table 1. The included subjects were all clearly diagnosed as HU, and all the literature clearly reported the diagnosis basis. In all the articles, Wuling powder (used singly or in combination with other prescriptions) was used in the experimental group, and conventional Western medicine was used in the control group.
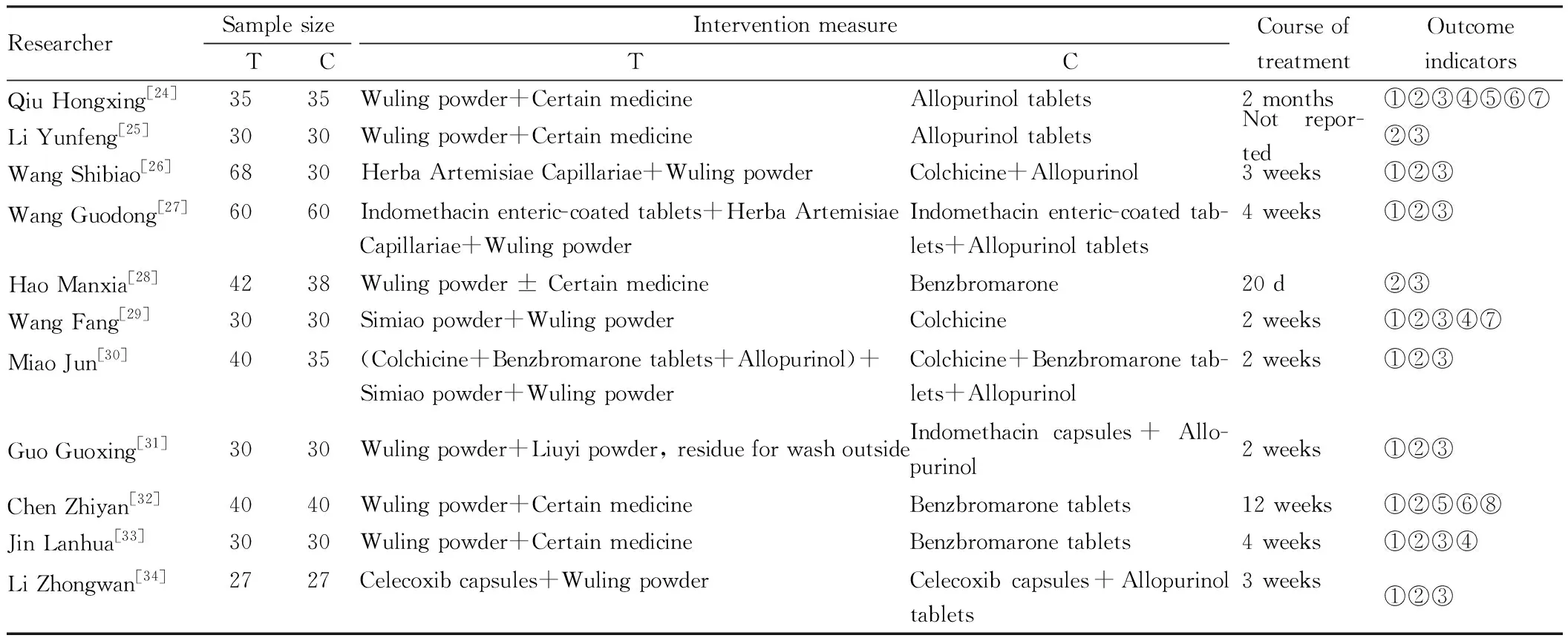
Table 1 Features of included literature
3.3 Quality evaluationThe results of the Cochrane systematic review show that the 11 articles[24-34]were all grouped by random methods, random number table method in 2 articles[33-34], numbering-based random grouping in one article[27], admission order-based grouping in one article[25], and simple random methods in the rest articles. None of the articles mentions allocation concealment, one article[29]uses the single-blind method, and one article[32]mentions withdrawal and dropout cases. The methodological characteristics are detailed in Table 2. The evaluation results of the bias risk are shown in Fig.2.
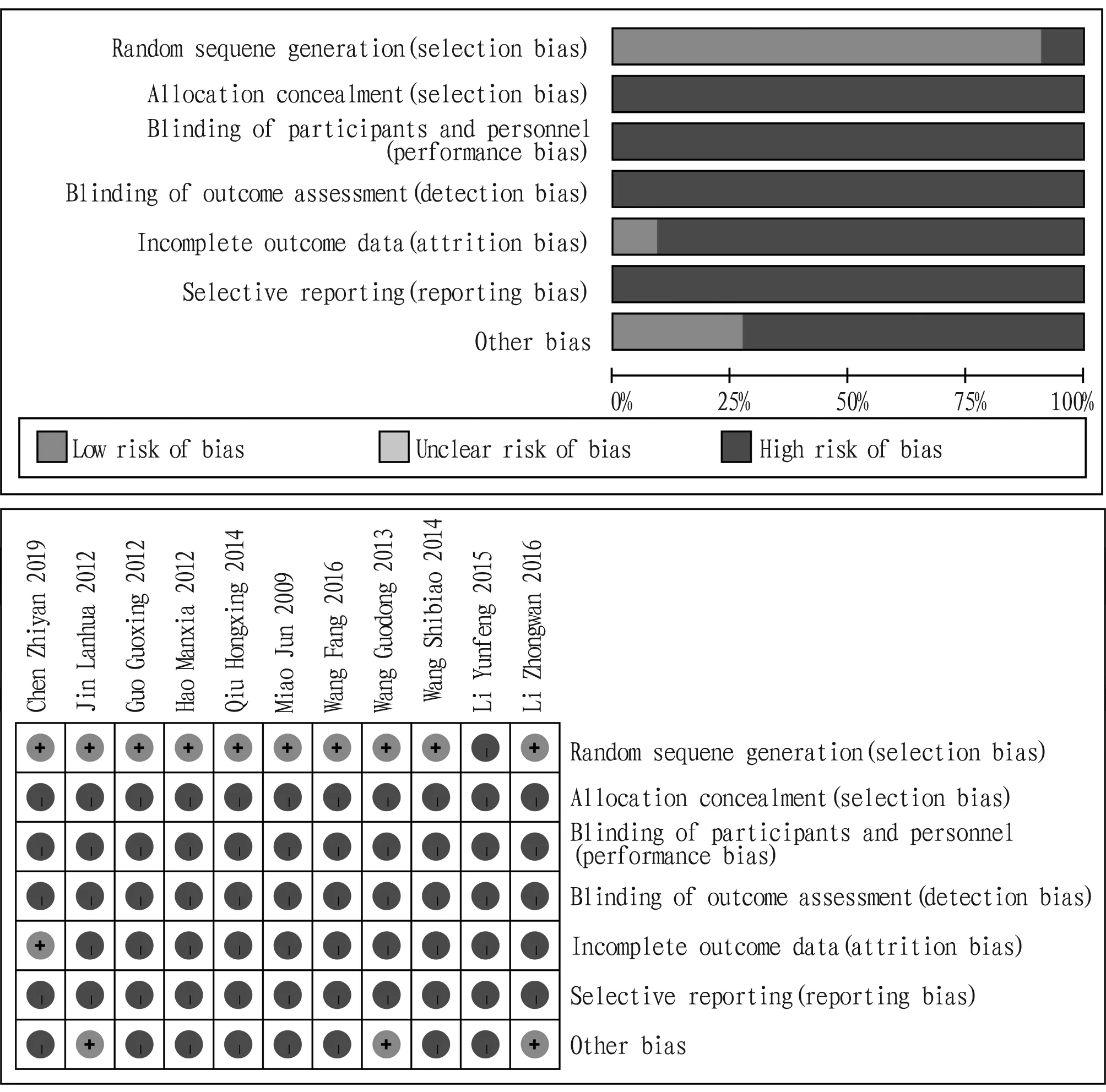
Fig.2 Analysis results of bias risk of included literature

Table 2 Methodological quality evaluation of included literature
3.4 Meta-analysisIn the literature included in this study, the outcome indicators include the SUA level. The evaluation of the overall effect in most of the included literature is based on the evaluation method for the overall effect on gout (GuidingPrinciplesforClinicalResearchofNewDrugs[35-37], which does not list the evaluation method for the overall effect on serum uric acid level), and the indicators also cover non-SUA indicators such as patient’s pain level. We believe that improving the actual symptoms of patients is the focus of clinical research evaluation and should be paid attention to. However, the main purpose of this study is to explore the influence of the experimental drug on the level of SUA, and in the clinic, HU patients are not necessarily accompanied by gout, and patients with gout may also not be accompanied by HU due to good medication control. Therefore, the overall effect reported in these articles was not included in the study.
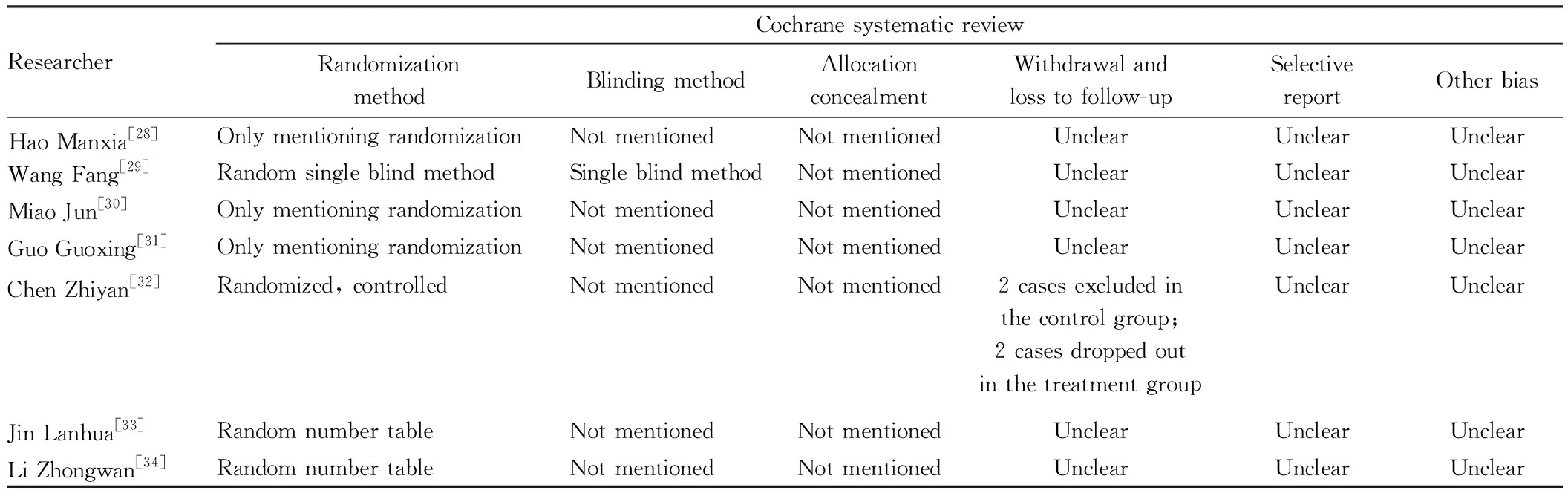
ResearcherCochrane systematic reviewRandomizationmethodBlinding methodAllocationconcealmentWithdrawal andloss to follow-upSelectivereportOther biasHao Manxia[28]Only mentioning randomizationNot mentionedNot mentionedUnclearUnclearUnclearWang Fang[29]Random single blind methodSingle blind methodNot mentionedUnclearUnclearUnclearMiao Jun[30]Only mentioning randomizationNot mentionedNot mentionedUnclearUnclearUnclearGuo Guoxing[31]Only mentioning randomizationNot mentionedNot mentionedUnclearUnclearUnclearChen Zhiyan[32]Randomized, controlledNot mentionedNot mentioned2 cases excluded inthe control group;2 cases dropped outin the treatment group UnclearUnclearJin Lanhua[33]Random number tableNot mentionedNot mentionedUnclearUnclearUnclearLi Zhongwan[34]Random number tableNot mentionedNot mentionedUnclearUnclearUnclear
Taking SUA as the observation index, a heterogeneity test (I2=92%) was performed on the 11 articles, and it is indicated that there is a certain degree of heterogeneity between the studies, so the random effects model is adopted for meta-analysis. The results show thatSMD=-0.37, 95%CI(-0.90, -0.16), andP=0.17, without statistical difference between the two groups, indicating that the treatment group was not evidently better than the control group in reducing SUA level in HU patients, so further subgroup analysis was required (Fig.3).

Fig.3 SUA forest plot
3.5 Subgroup analysisThe results of meta-analysis show that the heterogeneity of the research is great, so subgroup analysis was conducted based on the use of Wuling powder alone and in combination with other prescriptions to try to explain the source of heterogeneity.
3.5.1Subgroup analysis of original prescription and modified prescription of Wuling powder. The treatment groups of total 6 articles[24-25, 28, 32-34]used Wuling powder alone, and the rest 5 articles[26-27, 29-31]used Wuling powder in combination with other Chinese medicines. The results of the SUA subgroup analysis are shown in Fig.4.
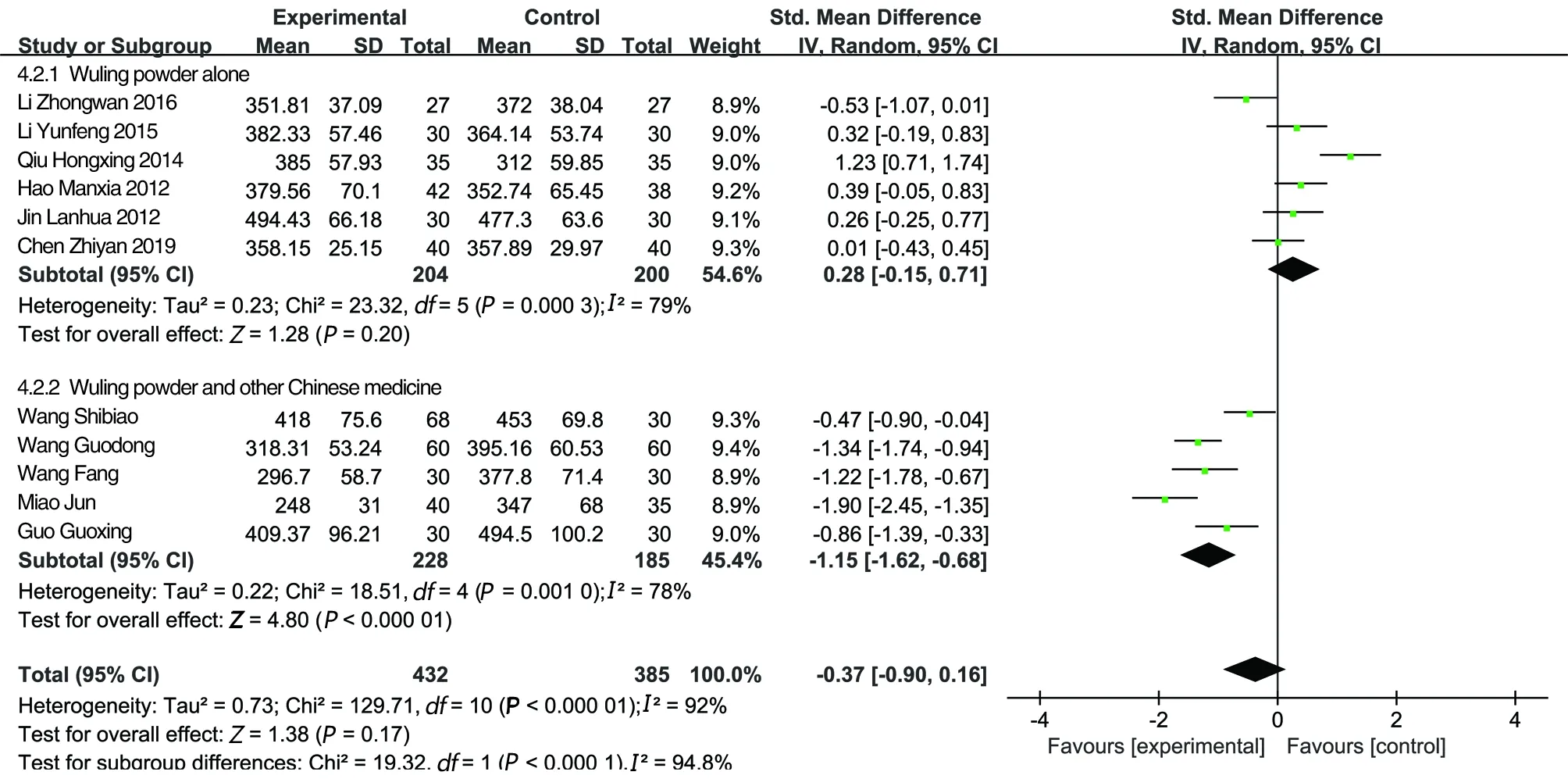
Fig.4 SUA forest plot of subgroups of original and modified prescriptions of Wuling powder
3.6 Safety analysisA total of 4 articles[26-27, 30, 32]reported adverse reactions, and none of the others reported. The results showed that 1 case of diarrhea occurred in the treatment group, and 16 cases of gastrointestinal reactions, 5 cases of drug intolerance, 3 cases of dizziness, 2 cases of leukopenia, and 1 case of allergic rash appeared in the control group. The incidence of adverse reactions in the treatment group was 0.48% (1/208), and that in the control group was 16.36% (27/165). The difference is statistically significant [RR=0.07, 95%CI(0.02, 0.24),P<0.000 1], indicating the use of Wuling powder combined with other prescriptions to treat HU has a lower incidence of adverse reactions than conventional Western medicines for lowering uric acid (Fig.5).
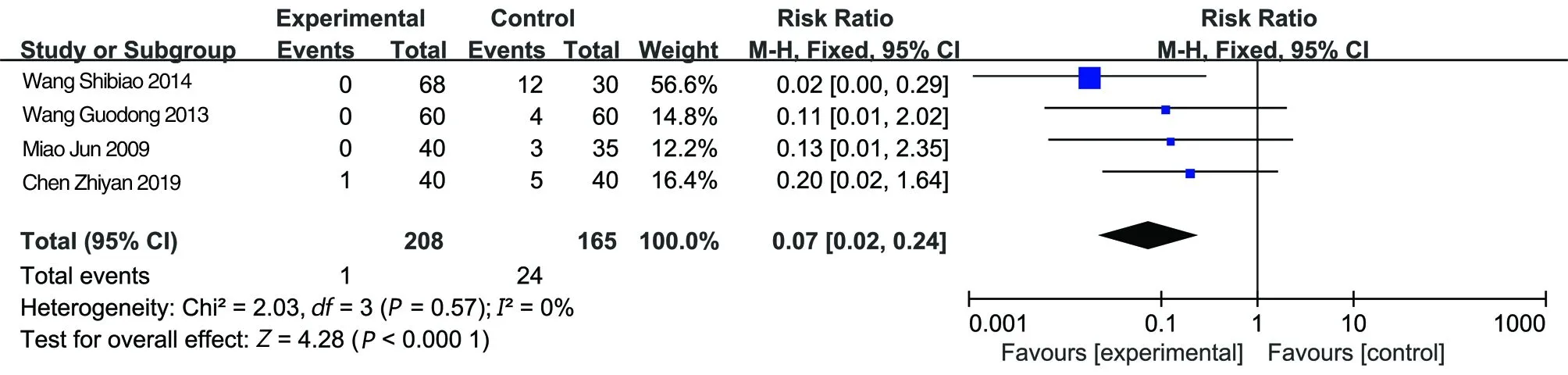
Fig.5 Forest plot of adverse reaction incidence
3.7 Analysis of publication biasThe publication bias of SUA is elucidated using a funnel chart. The results of Egger’s test (t=-0.13,P>0.901) show that there was no significant publication bias (Fig.6), but those of Begg’s test (Z=0.180,P=0.200) show that there was significant publication bias in the SUA level (Fig.7).
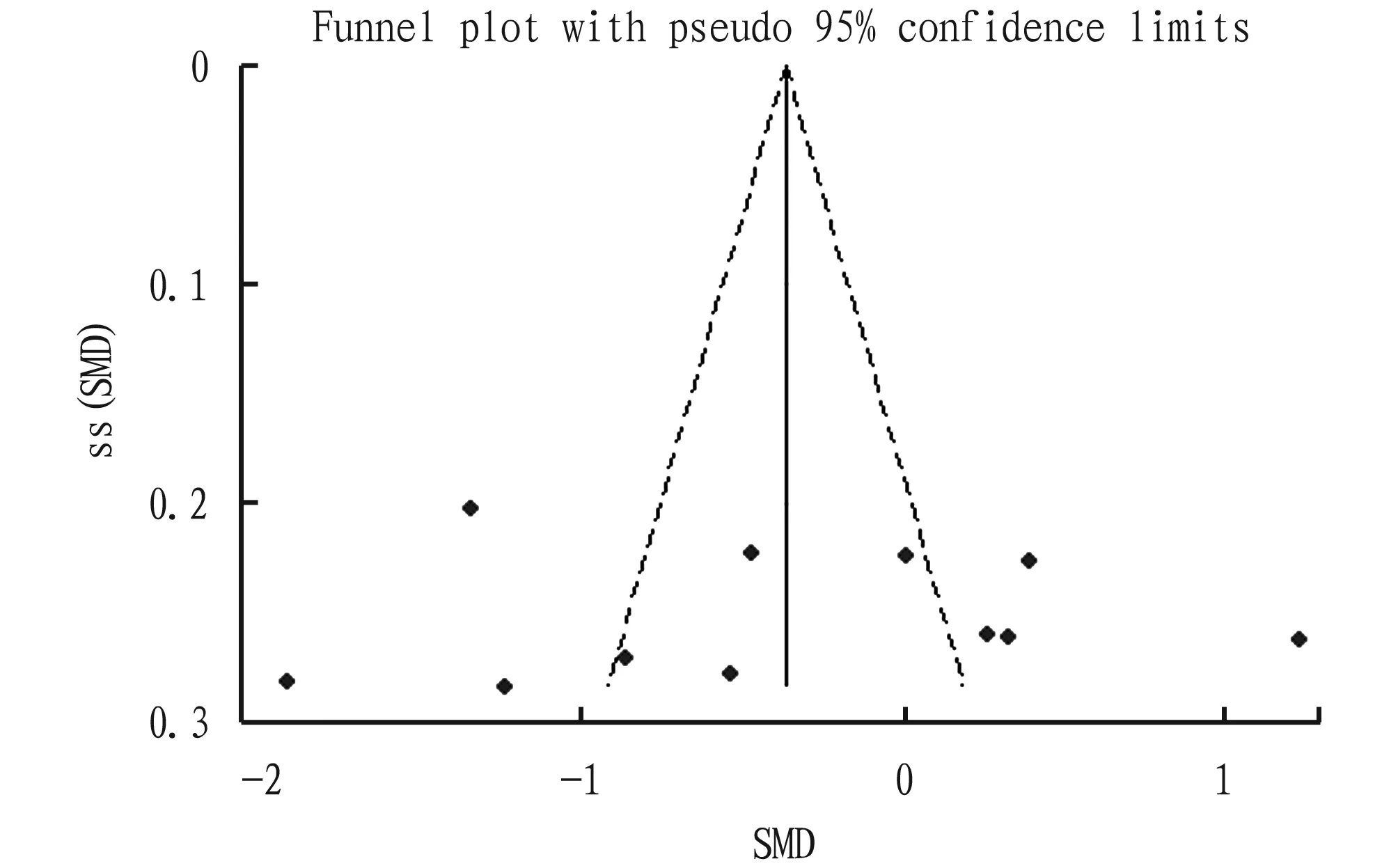
Fig.6 Funnel plot of SUA publication bias
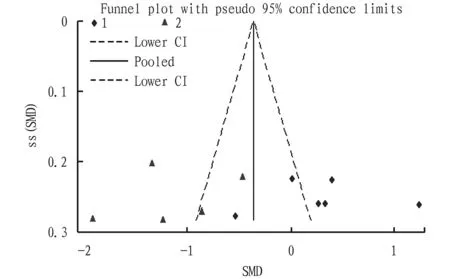
Note: 1. Wuling powder alone; 2. Original and modified prescriptions of Wuling powder.
4 Discussion
A total of 11 articles were included in this study, involving 817 patients. The analysis results show that although the overall effect of Wuling powder (used singly or in combination with other prescriptions) is more effective in reducing patients’ SUA level than conventional uric acid-lowering drugs, but the difference is not statistically significant. What is more, there is great heterogeneity among the studies. Subgroup analysis found that compared with conventional SUA-lowering western medicine, Wuling powder has a better effect in reducing patients’ SUA level when combined with other prescriptions (except for single use), with statistical difference, and the heterogeneity between groups also decreased.
Existing experimental research shows that Wuling powder should indeed have a certain effect in the treatment of HU, and the main mechanism is to increase the excretion of urine, sodium, urea,etc., similar to that of benzbromarone[38-43]. This study found that the effect of Wuling powder single use subgroup was not better than that of the control drug (the difference from the control drug was not statistically significant,P=0.20), indicating that although Wuling powder alone has no advantage over the control drug, it is at least equivalent in effect, consistent with the finding of the above study that its onset mechanism is similar to western medicine.
In addition, it was observed that in the subgroup of Wuling powder modified prescriptions, the compatible prescriptions used commonly include Yinchen Wuling powder, Pingwei powder, Simiao powder and Simiao Yongan decoction, and the single herbs used commonly included Herba Artemisiae Capillariae, Rhizoma Atractylodis and Cortex Magnoliae Officinalis. The above-mentioned prescriptions and herbs have all been reported clinically and experimentally, providing evidence for their effectiveness and mechanisms[44-46], and corroborating the results of this study.
Traditional Western medicines such as allopurinol, febuxostat and benzbromarone have been the basic drugs for the treatment of HU for decades, but a certain amount of adverse events have been reported[47-50]. Traditional Chinese medicine believes that gout-related diseases belong to the categories of "pyretic arthralgia" and "pain arthralgia", and their treatment is based on the principle of "activating blood circulation, relieving pain, promoting urination and excreting dampness"[51]. According toTreatiseonFebrileDiseases, the pathogenesis of the diseases treated with Wuling powder prescription is the abnormal metabolism of fluid in the body, and Wuling powder is a representative prescription for strengthening the spleen, exuding dampness and promoting urination[52]. Pharmacological studies have shown that Wuling powder can increase urine output and increase the excretion of Na+, K+and Cl-in urine, and its diuretic and sodium excretion effect approaches or exceeds that of western diuretics[53]. This is in line with the understanding of Chinese medicine, and is the same as the treatment principle of promoting uric acid excretion in Western medicine. The results of this study show that the incidence of adverse reactions in the Western medicine group was 12.16%, while that in the Wuling powder group was only 1.34%, indicating that Wuling powder has a low incidence of adverse reactions. When Wuling powder is used with allopurinol, in addition to promoting uric acid excretion and inhibiting uric acid production, it is possible to avoid the disadvantages of increased risk of adverse events when two types of Western medicine are used in combination.
The main advantage of this study is that the experimental groups of all the included articles used Wuling powder alone or in combination with other prescriptions (except conventional Western medicines for lowering uric acid), and the final overall effect is entirely from traditional Chinese medicine. Subgroup analysis was used to compare the effect of Wuling powder used singly or in combination with other traditional Chinese medicines and conventional therapies, and it was found that Wuling powder combined with other traditional Chinese medicines has a significantly better uric acid lowering effect than the control drugs. This provides evidence for how to choose prescriptions and medications for hyperuricemia.
The meta-analysis in this study has certain limitations, dominated by low methodological quality of the included studies and the small number of included trials. Among the 11 articles, only 4 articles[26-27, 29, 32]describe randomization methods. None of the articles mentioned allocation concealment or blinding. The quality of the research involved in this study is low, so the results may be biased. The included studies have a small sample size, and the systematic error caused by the "small sample research effect" cannot be ruled out[54]. In addition, only 4 of the 11 articles[26-27, 30, 32]described adverse reactions. Due to insufficient description, the count data of adverse reactions is not comprehensive. Therefore, with the development of large-scale, well-designed randomized controlled trials, a more reasonable method is needed to evaluate the adverse reactions and clinical efficacy of Wuling powder. Limited by the number of documents that meet the criteria for inclusion, this study was unable to pass subgroup analysis. Which prescription used in combination with Wuling powder has the best effect needs further study.
The above results indicate that traditional classic prescriptions can achieve satisfactory results in the treatment of HU when used under the guidance of the theory of syndrome differentiation. Clinically, based on syndrome differentiation, modifying the prescription appropriately may achieve better results. But limited by the number of existing studies, it is yet unable to conduct a sufficient subgroup analysis to distinguish whether this therapeutic advantage comes from other prescriptions used in combination or the interaction between these prescriptions and Wuling powder. Therefore, by combining previous reports and the results of this research, based on the above discussion and analysis, we infer that the effect and mechanism of Wuling powder to reduce SUA should be similar to those of benzbromarone. When combined with other prescriptions with non-diuretic mechanism, a better result will be achieved than Wuling powder alone. In addition, the disadvantage of increased risk of adverse events when two types of Western medicine are used in combination may be avoided.
5 Conclusions
Wuling powder combined with other prescriptions is better than conventional Western medicine in treating HU, with good safety. Wuling powder alone is not as effective as conventional Western medicine. In clinical work, doctors may need to modify the prescription of Wuling powder. The low quality of the literature supporting this conclusion suggests that this evidence should be interpreted with caution.
猜你喜欢
杂志排行

Medicinal Plant的其它文章
- Introduction and Selection of Dandelion Varieties under the Forest
- Study on the Quality Standard of Dujieqing Pill
- A Case Report of Immediate Implant Placement Combined with Flap Surgery, Guided Bone Regeneration and Non-submerged Healing with a Labial Bone Wall Defect in the Esthetic Zone
- Effects of Rhynchophylline on Learning and Memory of Alzheimer’s Disease Zebrafish
- Research Progress of Hirudo
- Evaluation of Anti-inflammatory Effect of Different Polar Parts of Argyreia acuta Lour.