Effects of acupoint thread-embedding therapy on serum apelin and GLP-1 in type 2 diabetes mellitus patients with obesity due to dampness-heat encumbering spleen
2021-04-23XuBingguo徐炳国WangHui王会WangShulan王淑兰DaiLijuan戴丽娟
Xu Bing-guo (徐炳国), Wang Hui (王会), Wang Shu-lan (王淑兰), Dai Li-juan (戴丽娟)
Nanjing First Hospital, Nanjing Medical University, Nanjing 210006, China
Abstract
Objective: To observe the effects of acupoint thread-embedding therapy on serum apelin and glucagon-like peptide-1(GLP-1) in type 2 diabetes mellitus patients with obesity due to dampness-heat encumbering spleen.
Methods: Sixty-six patients were randomly divided into a control group and an observation group according to the random number table method, with 33 cases in each group. Patients in the control group were treated with exenatide and metformin, while patients in the observation group were treated with additional acupoint thread-embedding. After 12-week treatment, the obesity-related indicators, including body mass index (BMI), waist circumference and body fat rate, the glycometabolism indicators, including fasting blood glucose, 2 h postprandial blood glucose and glycosylated hemoglobin, and the lipid metabolism indicators, including total cholesterol (TC), triglyceride (TG) and low-density lipoprotein cholesterol (LDL-C), as well as serum apelin and GLP-1 levels were observed in patients of the two groups.
Results: After treatment, the BMI, waist circumference and body fat rate of patients in the two groups were all reduced(all P<0.05), and were lower in the observation group than in the control group (all P<0.05); the fasting blood glucose,2 h postprandial blood glucose and glycosylated hemoglobin levels of patients in both groups were all decreased (all P<0.05), and were significantly lower in the observation group than in the control group (all P<0.05); the TC level was decreased (P<0.05), while the TG and LDL-C levels did not change significantly in the control group (both P>0.05); the TC,TG and LDL-C levels were all significantly reduced in the observation group (all P<0.05), lower than those in the control group (all P<0.05); the serum apelin level was decreased (P<0.05) and the serum GLP-1 level was increased (P<0.05) in the observation group, statistically different from those in the control group (both P<0.05).
Conclusion: Combined with the conventional medication, acupoint thread-embedding therapy can significantly improve the obesity-related indicators, glycometabolism and lipid metabolism in type 2 diabetes mellitus patients with obesity due to dampness-heat encumbering spleen. This may be achieved by regulating the serum apelin and GLP-1 levels.
Keywords: Embedding Therapy; Embedding, Thread; Acupoint Therapy; Obesity; Diabetes Mellitus, Type 2; Apelin;Glucagon-like Peptide 1
Type 2 diabetes mellitus (T2DM) is a common metabolic disease. The T2DM incidence has been significantly increasing in recent years due to the life style change with the continuous improvement of living standards[1]. In China, more than 80% of T2DM patients have obesity or are overweight[2]. Obesity increases the risk of T2DM and the difficulty in blood glucose control.It is also an important factor in the occurrence of T2DM complications such as diabetic nephropathy and atherosclerosis[3]. Therefore, strengthening weight management together with reducing blood glucose is of great significance for the treatment of T2DM with obesity. The hypoglycemic drugs with weight loss are mainly glucagon-like peptide-1 (GLP-1) receptor agonists,sodium-glucose co-transporter 2 (SGLT2) inhibitors, and metformin. However, GLP-1 receptor agonists are expensive and difficult to be popularized and SGLT2 inhibitors have adverse reactions such as genitourinary system infections, fractures and ketoacidosis[4]. In recent years, studies have shown that acupoint threadembedding therapy shows a satisfactory effect on simple obesity and T2DM, with benefits for weight loss and blood glucose control. Therefore, it has a good application prospect in the treatment of T2DM with obesity[5-6]. The current study observed the effect of acupoint thread-embedding therapy combined with the conventional medication on serum apelin and GLP-1 in T2DM patients with obesity due to dampness-heat encumbering spleen. The report is as follows.
1 Clinical Materials
1.1 Diagnostic criteria
1.1.1 Diagnostic criteria in Western medicine
T2DM diagnostic criteria[7]: Typical diabetes symptoms(polydipsia, polyphagia and polyuria), random
blood glucose ≥11.1 mmol/L, fasting blood glucose≥7.0 mmol/L, and 2 h intravenous blood glucose≥11.1 mmol/L in a glucose tolerance test. If the same result was obtained in a repeated test, the final diagnosis can be confirmed when any of the above three blood glucose levels met the standard, even without obvious hyperglycemia.
Obesity diagnostic criteria[8]: Body mass index (BMI)≥28 kg/m2; or waist circumference ≥90 cm in men, or≥85 cm in women.
1.1.2 Syndrome differentiation criteria of traditional Chinese medicine (TCM)
The TCM syndrome differentiation criteria for dampness-heat encumbering spleen were developed following theGuiding Principles for Clinical Study of NewChinese Medicines[9]. Main symptoms: obese body shape;chest, gastric and abdominal distension or fullness after eating; heavy feeling in the head and whole body.Secondary symptoms: distress and stuffiness in the heart and chest, weakness in the extremities, reddish yellow urine, and sticky stool. A red tongue with yellow-greasy coating, and slippery-rapid pulse.
1.2 Inclusion criteria
Met the above-mentioned diagnostic criteria for T2DM and obesity; met the TCM syndrome differentiation criteria for dampness-heat encumbering spleen; glycosylated hemoglobin ≥7%; 20-70 years old;voluntarily participated in the trial with signed informed consent form.
1.3 Exclusion criteria
Patients with acute complications such as diabetic ketoacidosis, diabetic hyperosmolar coma, or acute diabetic infection within 1 month; pregnant or lactating women; patients with severe cardiovascular, lung, or kidney diseases; patients who were allergic to the involved drugs.
1.4 Elimination and dropout criteria
Those who failed to receive treatment as required;those who had incomplete data; those who could not continue the original treatment plan due to serious adverse reactions or deterioration of their condition during the trial; those who voluntarily withdrew from the trial.
1.5 Statistical methods
SPSS version 22.0 software was used for statistical analysis. The normally-distributed measurement data were expressed as mean ± standard deviation (±s) and compared witht-test; the Chi-square test was used for the count data.P<0.05 indicated a statistically significant difference.
1.6 General data
A total of 66 T2DM patients with obesity, who were admitted to our hospital between January 2018 and August 2019, were included and divided into a control group and an observation group according to the random number table method, with 33 cases in each group. There were no dropout cases in either group during the trial. The gender, age, fasting blood glucose,BMI and other general data between the two groups were not statistically different (allP>0.05), indicating that the two groups were comparable (Table 1).
2 Treatment Methods
Patients in the two groups were educated on the diabetes-related knowledge, and provided with personalized diet and exercise programs.thread was cut into short sections of 2 cm in length, and soaked in sterile normal saline. The patient lied in a supine position and exposed the acupoints; after iodophor disinfection, the surgeon wearing disposable sterile gloves with both hands inserted the protein thread into the front end of the needle tube for threadembedding, and quickly punctured the threadembedding needle and slowly pushed the wick-in-needle,while pulling the needle tube to completely implant the protein thread under the skin after arrival of needling sensation (Deqi); pressed the needle hole with a cotton ball to prevent bleeding after the needle withdrawal.Disinfected the needle hole again and covered it with a sterile dressing after checking and excluding exposed threads. Patients were treated twice a week, for a total of 12 weeks.
2.1 Control group
Exenatide [State Food and Drug Administration (SFDA)Approval No.: H20090382, Baxter Pharmaceutical Solutions LLC, USA] was subcutaneously injected,5 μg/time in the first 4 weeks, 10 μg/time after 4 weeks,twice a day; oral metformin hydrochloride tablets (SFDA Approval No.: H11020541, China Resources Doublecrane Pharmaceutical Co., Ltd., China), 0.5 g/time,3 times/d. Patients were treated for 12 weeks in total.
2.2 Observation group
Patients in the observation group were treated with acupoint thread-embedding combined with the medications used in the control group.
Acupoints: Zhongwan (CV 12), bilateral Tianshu (ST 25),Yinlingquan (SP 9), Zusanli (ST 36), Fenglong (ST 40) and Quchi (LI 11). Under sterile conditions, the protein

Table 1. Comparison of general data between the two groups
3 Observation of Results
3.1 Observation items
3.1.1 Obesity-related indicators
Obesity-related indicators, such as BMI, waist circumference and body fat rate in the two groups were measured and recorded before and after treatment.
3.1.2 Glycometabolism indicators
Glucose oxidase method and high-performance liquid phase method were used to determine the levels of fasting blood glucose, 2 h postprandial blood glucose,and glycosylated hemoglobin before and after treatment.3.1.3 Lipid metabolism indicators
An automatic biochemical analyzer was used to detect serum total cholesterol (TC), triglyceride (TG) and lowdensity lipoprotein cholesterol (LDL-C) levels before and after treatment.
3.1.4 Serum apelin and GLP-1 levels
Early morning fasting venous blood was drawn from the patients before and after treatment, and the serum apelin and GLP-1 levels of patients in the two groups were determined by enzyme-linked immunosorbent assay.
3.2 Results
3.2.1 Comparison of obesity-related indicators
The BMI, waist circumference and body fat rate before treatment were not significantly different between the two groups (allP>0.05), and were decreased in both groups after treatment (allP<0.05), lower in the observation group than in the control group (allP<0.05),(Table 2).
3.2.2 Comparison of glycometabolism indicators
The fasting blood glucose, 2 h postprandial blood glucose, and glycosylated hemoglobin levels before treatment were not significantly different between the two groups (allP>0.05), and were decreased after treatment (allP<0.05), significantly lower in the observation group than in the control group (allP<0.05),(Table 3).
3.2.3 Comparison of lipid metabolism indicators
Before treatment, there were no statistical differences in the TC, TG and LDL-C levels between the two groups(allP>0.05). After treatment, the TC level in the control group was decreased (P<0.05), while the TG and LDL-C levels did not change significantly (bothP>0.05); the TC,TG and LDL-C levels in the observation group were significantly decreased (allP<0.05) and lower than in the control group (allP<0.05), (Table 4).
3.2.4 Comparison of the serum apelin and GLP-1 levels
There were no significant differences in the serum apelin and GLP-1 levels between the two groups before treatment (bothP>0.05). After treatment, the serum GLP-1 level was increased (P<0.05), while the serum apelin level did not change significantly in the control group (P>0.05); the serum apelin level was decreased(P<0.05), and the serum GLP-1 level was increased(P<0.05) in the observation group, and they were statistically different from those in the control group(bothP<0.05), (Table 5).
Table 2. Comparison of obesity-related indicators between the two groups ( ±s)

Table 2. Comparison of obesity-related indicators between the two groups ( ±s)
Note: Compared with the same group before treatment, 1) P<0.05; compared with the control group after treatment, 2) P<0.05
Group n Time Average BMI (kg/m2) Average waist circumference (cm) Average body fat rate (%)Control 33 Before treatment 29.78±0.80 100.74±5.90 35.65±3.23 After treatment 28.92±0.721) 97.79±4.921) 33.99±3.051)Observation 33 Before treatment 29.95±0.76 101.19±4.86 34.81±3.32 After treatment 28.36±0.691)2) 93.94±2.951)2) 31.11±2.721)2)
Table 3. Comparison of glycometabolism indicators between the two groups ( ±s)

Table 3. Comparison of glycometabolism indicators between the two groups ( ±s)
Note: Compared with the same group before treatment, 1) P<0.05; compared with the control group after treatment, 2) P<0.05
Group n Time Fasting blood glucose(mmol/L)2 h postprandial blood glucose(mmol/L)Glycosylated hemoglobin(%)Control 33 Before treatment 8.27±0.81 13.81±1.47 8.08±0.57 After treatment 6.61±0.611) 10.19±1.591) 6.87±0.431)Observation 33 Before treatment 8.16±0.72 14.01±1.58 8.06±0.58 After treatment 6.16±0.581)2) 9.15±1.271)2) 6.53±0.331)2)
Table 4. Comparison of lipid metabolism indicators between the two groups ( ±s, mmol/L)

Table 4. Comparison of lipid metabolism indicators between the two groups ( ±s, mmol/L)
Note: Compared with the same group before treatment, 1) P<0.05; compared with the control group after treatment, 2) P<0.05
Group n Time TC TG LDL-C Control 33 Before treatment 4.79±0.48 2.52±0.60 2.73±0.62 After treatment 4.10±0.511) 2.49±0.51 2.77±0.57 Observation 33 Before treatment 4.69±0.39 2.63±0.59 2.84±0.61 After treatment 3.72±0.441)2) 1.99±0.491)2) 2.44±0.541)2)
Table 5. Comparison of serum apelin and GLP-1 levels between the two groups ( ±s)
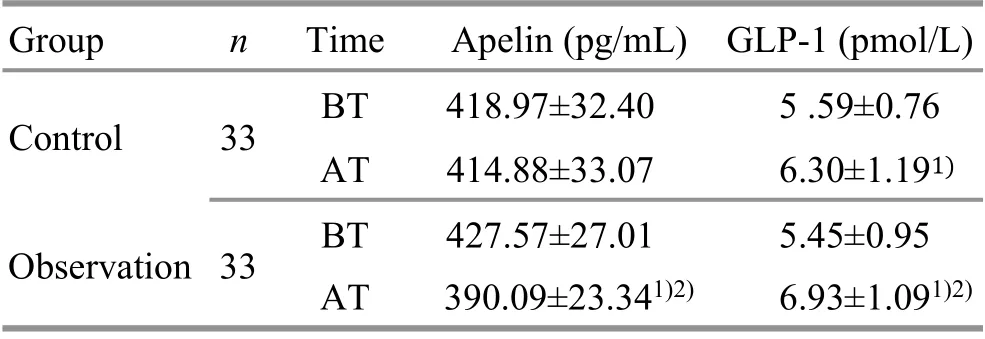
Table 5. Comparison of serum apelin and GLP-1 levels between the two groups ( ±s)
Note: BT=Before treatment; AT=After treatment; compared with the same group before treatment, 1) P<0.05; compared with the control group after treatment, 2) P<0.05
Group n Time Apelin (pg/mL) GLP-1 (pmol/L)Control 33 BT 418.97±32.40 5 .59±0.76 AT 414.88±33.07 6.30±1.191)Observation 33 BT 427.57±27.01 5.45±0.95 AT 390.09±23.341)2) 6.93±1.091)2)
4 Discussion
Most researchers believe that insulin resistance is the fundamental mechanism of T2DM caused by obesity[10].In obesity, fat cells are accumulated to secrete large amounts of adiponectin, leptin, tumor necrosis factor-α,resist in and other adipocytokines; meanwhile,macrophages are accumulated to induce inflammation,changing the body’s immune environment and lipid metabolism, which lead to insulin resistance. Then the efficiency of glucose utilization by muscles and other tissues are reduced, and excessive insulin is produced by compensatory secretion, which eventually causes pancreatic failure and diabetes mellitus[10-11].
Exenatide and metformin are commonly used drugs in the treatment of T2DM with obesity. Exenatide is the first artificially synthesized GLP-1 receptor agonist, which promotes the differentiation and proliferation of pancreatic β-cells, improves insulin resistance, produces a long-lasting and stable blood glucose control effect,and has a low risk of hypoglycemia[12]. Exenatide can also reduce gastric emptying, gastrointestinal motility and gastrointestinal absorption. Meanwhile, it also affects the leptin-controlled central appetite to reduce hunger and increase satiety. In addition, exenatide also acts on the adipocytes to reduce the expression of adipocyte peroxisome proliferator-activated receptor γ and protein,to inhibit the differentiation, maturation, and proliferation of adipocytes, thereby achieving weight loss and lipid regulation[13]. Metformin plays a hypoglycemic effect by reducing liver glucose output and enhancing the sensitivity of peripheral tissues to insulin. It is a firstline drug for T2DM with weight loss effect[14].
T2DM with obesity belongs to the categories of‘Xiaoke (diabetes)’ and ‘obesity’ in TCM. Dampness-heat encumbering spleen is the key factor in the pathogenesis of this disease. Long-term consumption of fatty, sweet,greasy and heavy-tasting foods will damage the spleen and stomach. Consequently, the water and grain essence is accumulated in the skin, muscles and internal organs to form the fat rather than to be transported. The lasting accumulation of fat will lead to obesity. Meanwhile,spleen deficiency causes endogenous phlegm-dampness,which will then be transformed into heat. The dampnessheat will encumber the spleen and stomach, causing abdominal flatulence and endogenous heat, and then the transformed heat will lead to body fluid consumption,which eventually develops into ‘Xiaoke’. Studies have reported that dampness-heat encumbering spleen is the predominant syndrome in T2DM with obesity,accounting for about 41%, significantly higher than other syndromes[15]. It can be seen that the fundamental cause of T2DM with obesity is spleen deficiency, while the manifestation is damp-heat. Therefore, the treatment should be based on invigorating the spleen, dispelling dampness and clearing heat.
Acupoint thread-embedding therapy is to embed thread into the corresponding acupoints to produce continuous and long-lasting stimulation to the acupoints,suitable for chronic diseases such as T2DM with obesity[16]. In the current study, Zhongwan (CV 12),Tianshu (ST 25), Yinlingquan (SP 9), Zusanli (ST 36),Fenglong (ST 40) and Quchi (LI 11) were selected as the main acupoints. Among them, Zhongwan (CV 12) is the Front-Mu point of the stomach, which is one of the Eight Influential points (Fu organs), and also the crossing point of the Meridians of Hand Taiyang, Hand Shaoyang and Foot Yangming and the Conception Vessel. The function of Zhongwan (CV 12) is to invigorate the spleen and stomach, regulate qi activities and resolve the dampness.Tianshu (ST 25) is the Front-Mu point of the large intestine, and can invigorate the spleen and stomach,dredge the intestines, regulate qi activities and dissipate the stagnation, clear the heat and remove the dampness.Yinlingquan (SP 9) is the He-Sea point of the Spleen Meridian, having the effects of invigorating the spleen and expelling the dampness, and clearing the dampness and heat. Zusanli (ST 36) is the He-Sea point of the Stomach Meridian, having the functions of strengthening the spleen and tonifying qi, regulating the qi movement, and transporting and distributing the fluids. Fenglong (ST 40) is the Luo-Connecting point of the Stomach Meridian, good for regulating the spleenstomach qi. It not only regulates the Taiyin (spleen) to transport water and dampness, but also modulates Yangming (stomach) to remove heat. It is suitable to treat internal accumulation of phlegm and dampness, and dampness-heat encumbering spleen. Quchi (LI 11) is the He-Sea point of the Large Intestine Meridian. It can clear the heat of the large intestine and remove phlegm and turbidity. These acupoints were used together to invigorate the spleen, tonify qi, and clear dampness-heat.
The results of this study showed that after treatment,the BMI, waist circumference and body fat rate in the two groups were all reduced, and were lower in the observation group than in the control group; the fasting blood glucose, 2 h postprandial blood glucose and glycosylated hemoglobin levels in the two groups were decreased, and were significantly lower in the observation group than in the control group; the TC level was decreased in the control group, while the TG and LDL-C levels did not change significantly; the TC, TG and LDL-C levels were significantly reduced in the observation group, and were lower than in the control group. These results indicated that the application of acupoint thread-embedding plus medication significantly improved indicators of obesity-related,glycometabolism and lipid metabolism in T2DM patients with obesity.
The serum apelin and GLP-1 levels in the two groups were also measured before and after treatment in this study. Apelin is a kind of adipokines secreted by white fat and closely related to obesity. Studies have shown that the serum apelin level in obesity patients is significantly higher than that in the healthy control, and is significantly positively correlated with BMI; the serum apelin level is closely related to visceral fat, the more visceral fat, the higher the serum apelin level[17]. Apelin is also related to insulin sensitivity, since it has an inhibitory effect on insulin secretion stimulated by hyperglycemia. Apelin also mediates the expression of coupling proteins, and interferes with insulin signal transduction and glucose transportation to induce insulin resistance[18]. These findings all suggested that apelin was the connection point between obesity and T2DM. GLP-1 is a peptide hormone secreted by intestinal L cells. By binding to the GLP-1 receptor, it promotes the secretion of insulin by β cells, enhances the glucose utilization capacity of peripheral tissues, and reduces the liver glycogen output[19]. GLP-1 also inhibits gastric juice production to slow down gastrointestinal motility, and acts as an appetite suppressing neuropeptide to reduce food intake[20]. It can be seen that the GLP-1 secretion decrease is related to the onset of both T2DM and obesity. In this study we found that the serum apelin level was decreased, and the serum GLP-1 level was increased in the observation group after treatment,which were statistically different from those in the control group (allP<0.05). These results suggested that medication combined with acupoint thread-embedding significantly regulated the serum apelin and GLP-1 levels in T2DM patients with obesity. Therefore, regulating the serum apelin and GLP-1 levels may be one of the mechanisms of acupoint thread-embedding in the treatment of T2DM with obesity.
In summary, combined with the conventional medication, acupoint thread-embedding therapy significantly improved obesity, glycometabolism and lipid metabolism in T2DM patients with obesity due to dampness-heat encumbering spleen. This may be achieved by regulating the serum apelin and GLP-1 levels.
Conflict of Interest
The authors declare that there is no potential conflict of interest in this article.
Statement of Informed Consent
Informed consent was obtained from all individual participants.Received: 23 February 2020/Accepted: 9 June 2020
杂志排行

Journal of Acupuncture and Tuina Science的其它文章
- Review of systematic reviews of acupuncture for diabetic peripheral neuropathy
- Clinical observation on spleen-invigorating and qibenefiting pediatric massage for treating recurrent respiratory tract infection in children with cerebral palsy due to qi deficiency of spleen and lung
- Acupoint catgut-embedding therapy as promising treatment for non-alcoholic fatty liver disease
- Clinical observation of electroacupuncture with different frequencies for migraine without aura
- Warm needling moxibustion plus PKP for vertebral compression fracture due to kidney deficiency and blood stasis: a randomized controlled trial
- Evaluation of the prevention and treatment effects of acupuncture-moxibustion for Alzheimer disease based on various mouse models