Intravascular lymphoma with hypopituitarism:A case report
2020-09-14
Teiko Kawahigashi,Department of General Internal Medicine,Shonan Kamakura General Hospital,Kanagawa 247-8533,Japan
Shinichi Teshima,Department of Histopathology,Shonan Kamakura General Hospital,Kanagawa 247-8533,Japan
Eri Tanaka,Department of Hematology,Shonan Kamakura General Hospital,Kanagawa 247-8533,Japan
Abstract
Key words:Intravascular lymphoma;Random skin biopsy;Hypopituitarism;General internal medicine;Tingling;Pancytopenia;Case report
INTRODUCTION
Intravascular lymphoma (IVL) is a rare subtype of lymphoma,characterized by the selective proliferation of lymphoma cells within the lumina of small-to-medium-sized blood vessels[1].A B-cell immunophenotype is most commonly observed,although cases with T-cell receptor rearrangements have also been reported[2].Although various organs can be affected by lymphoma cells,hypopituitarism is an extremely rare complication,and limited cases have been reported[3].We herein report a case of hypopituitarism due to IVL,which was successfully treated with chemotherapy.
CASE PRESENTATION
Chief complaints
An 80-year-old Japanese woman with no significant comorbidities noticed a bilateral tingling sensation on the anterior surface of her lower limbs.
History of present illness
The sensation was localized below her thighs;however,she felt neither numbness nor weakness,and could walk and ride a bicycle without any problems.Her symptoms persisted for about one month,which resulted in a visit to a local outpatient clinic.Laboratory studies performed in the clinic showed pancytopenia.Although the patient was examined at another general hospital,the cause of her condition was unknown.Subsequently,she experienced a high fever (a temperature of 38°C - 39°C) daily.However,she did not have any other accompanying symptoms,such as chills,pain,and appetite loss,and her general state was relatively normal.Despite a more detailed evaluation,the patient’s diagnosis was inconclusive,and she was observed as an outpatient.Five months after her first visit,she was taken to the emergency department of the hospital at which she was previously treated,because of sudden loss of consciousness.Laboratory studies showed that she had lost consciousness because of hypoglycemia,and further evaluation revealed that hypoglycemia was one of the signs of hypopituitarism.She received glucocorticoid and replacement therapy.Whereas treatment resulted in blood glucose level control,the tingling sensation gradually progressed.Although seven months had elapsed since her first visit,the causes of her symptoms remained unknown.Therefore,she was admitted to the Department of Hematology of our hospital for further assessment.
History of past illness
Her past medical history was noncontributory.
Personal and family history
Her family history was noncontributory.
Physical examination upon admission
On physical examination,we observed the presence of a tingling sensation on the anterior regions of the lower limbs,under the thighs,and on both palms of the patient.Decreased vibratory sensation on both sides of the lower extremities was also noticed.Hepatosplenomegaly,lymph node enlargement,and skin eruption were not observed.
综上笔者对BIM技术在建筑施工阶段的应用流程进行了分析,BIM技术可在施工设计阶段、施工组织阶段等方面得以应用,详情如下:
Laboratory examinations
Blood test results were as follows:White blood cell count,300 cells/μL;Hemoglobin level,9.0 g/dL;and Platelet count,113000 platelets/μL,lactate dehydrogenase,971 IU/L;Ferritin,710 ng/mL;Soluble interleulin-2 receptor alpha,3412 U/mL.No evidence of infection or solid tumor was observed on serum examination,culture,and imaging.Brain magnetic resonance imaging (MRI),however,showed enlargement of the pituitary gland (Figure 1A and B).It did not appear to be a tumor as the entire pituitary gland was almost equally contrasted;no other abnormalities were present.We performed stimulating hormone tests,as the patient had been diagnosed with hypopituitarism in the previous hospital.The patient received an injection of four kinds of hormones [growth hormone (GH)-releasing hormone,corticotropin-releasing hormone,luteinizing hormone (LH)-releasing hormone,and thyrotropin-releasing hormone],and we monitored the levels of seven kinds of hormones [GH,LH,folliclestimulating hormone (FSH),thyroid-stimulating hormone (TSH),cortisol,adrenocorticotropic hormone (ACTH),and prolactin] produced in response.Low levels of six of the seven hormones were observed,with the exception of prolactin,which confirmed the diagnosis of hypopituitarism.
Imaging examinations
Contrast-enhanced computed tomography scans of the abdomen and pelvis showed a hepatic cyst and mild splenomegaly.There was no evidence of tumor and lymphadenopathy could not be seen.Bone marrow aspiration and biopsy,performed to evaluate pancytopenia,revealed the presence of hemophagocytic lymphohistiocytosis (HLH) (Figure 2A and B).There was no evidence of tumor involvement.She met five of eight criteria of HLH (fever ≥ 38.5°C,splenomegaly,peripheral blood cytopenia,hemophagocytosis in bone marrow,ferritin >500 ng/mL,elevated soluble IL-2 receptor alpha two standard deviations above age-adjusted laboratory-specific norms)[4].We suspected lymphoma as a cause of HLH,as no evidence of infection or solid tumors were present.One of the most common causes of adult HLH is lymphoma.However,as the patient did not show lymphadenopathy,a random skin biopsy was performed,which showed that the tumor cells had proliferated predominantly within the small vessels of the dermis with no infiltration outside the vessels (Figure 3).Immunohistochemical staining revealed positivity for the B-cell markers CD20 and CD79a in the absence of staining for T-cell markers.These characteristics were consistent with those of intravascular large B-cell lymphoma.
FINAL DIAGNOSIS
The patient was diagnosed with IVL,as well as HLH and hypopituitarism secondary to IVL.
TREATMENT
The patient was immediately treated with rituximab,cyclophosphamide,doxorubicin,vincristine,and prednisolone.After the first chemotherapy cycle,the tingling sensation partially improved and the symptoms in the palms disappeared.Bone marrow aspiration performed after the first chemotherapy cycle demonstrated the absence of hemophagocytosis,and the bone marrow image was normal,suggesting that HLH had improved with chemotherapy.She completed six cycles of chemotherapy.After the third cycle,head MRI showed that the pituitary gland had returned to its normal size (Figure 1C and D),and it remained at that size after the six cycles.Although the patient required hormone replacement therapy after chemotherapy,her LH,FSH,TSH,free T4,ACTH,and cortisol levels,which were all lower than normal,and prolactin levels,which were higher than normal,returned to normal levels and remained so after completion of the final chemotherapy cycle(Table 1).She did not develop any signs and symptoms associated withhypopituitarism,such as hypoglycemia,after the second cycle of chemotherapy,and her peripheral blood cell count remained normal.
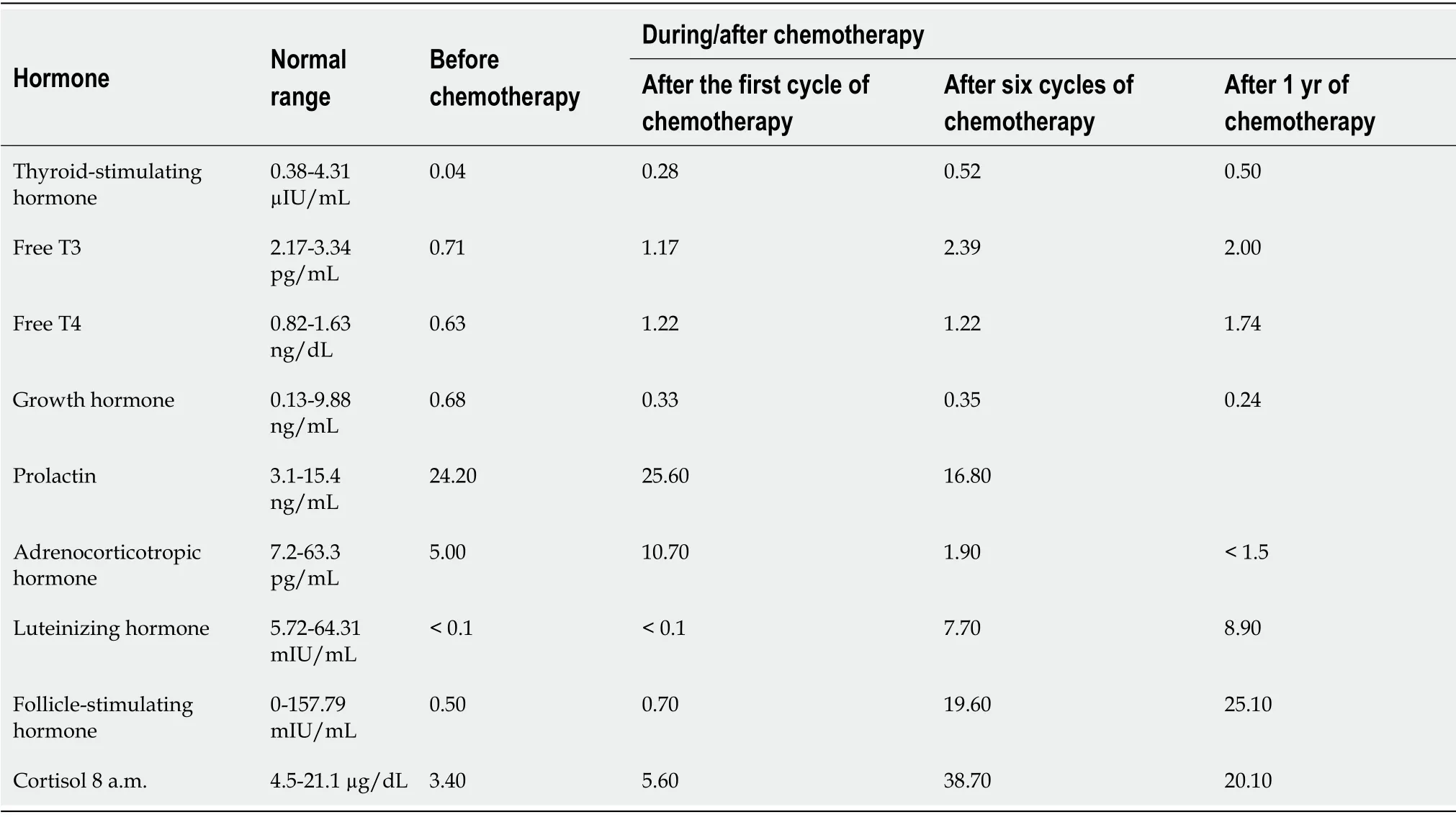
Table1 Hormonal levels before and during/after chemotherapy
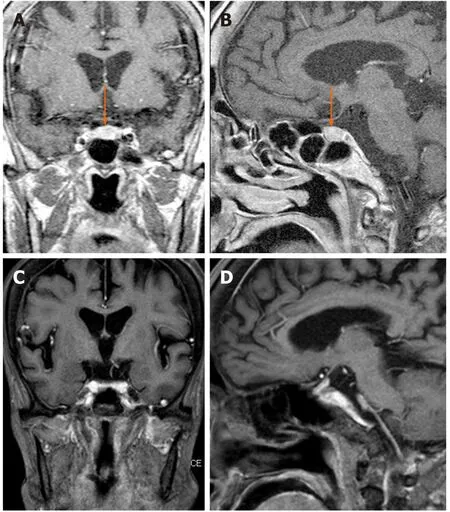
Figure1 Magnetic resonance imaging:T1-weighted imaging.
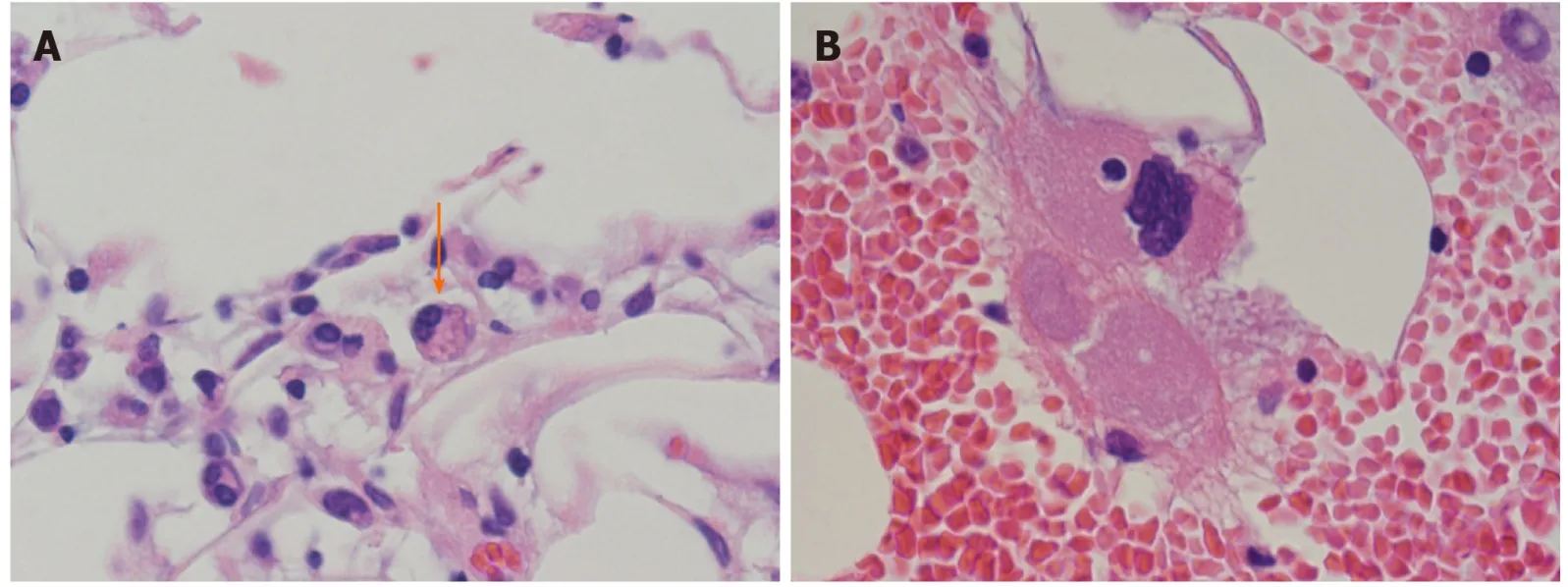
Figure2 Bone marrow aspiration showing hemophagocytosis (designated by an arrow).

Figure3 Hematoxylin and eosin.
OUTCOME AND FOLLOW-UP
A complete response was achieved,and the patient was relapse free two years after treatment.Although she still required minimal hormone replacement therapy,5 mg/d of hydrocortisone,she does not show any signs of hormone deficiency.
DISCUSSION
Antemortem diagnosis of IVL is often challenging because it affects various organs,resulting in highly variable and unpredictable presentations,although the lymph nodes are typically spared[1].For example,the presence of a tingling sensation,which was the first complaint in this case,is a common symptom of IVL.The proliferation of tumor cells leads to multiple ischemic necrosis of the central nervous system,nerve roots,cranial nerves,and peripheral nerves[5,6].This case highlights the importance of a random skin biopsy in diagnosing IVL.IVL is diagnosed by the identification of large lymphoma cells within small-to-medium blood vessels[7].IVL has been reported following biopsies of various organs,such as the bone marrow,liver,and/or spleen[7].However,with a random skin biopsy,sufficient specimens can be obtained easily with minimal invasion,and like the bone marrow trephine biopsy,it is highly sensitive for IVL diagnosis[7,8].Sitthinamsuwanet al[8]demonstrate that random skin biopsy is reliable method for diagnosis of IVL especially in patients with unusual neurological symptoms with co-existing hematologic abnormalities and without lymphadenopathy,such as our case.
In this case,we observed hypopituitarism,a rare complication of IVL.Endocrinopathy is a rare presentation of IVL.Hypopituitarism associated with IVL Bcell lymphoma has been described in fewer than 20 reports[3].The pituitary gland is a hypervascular organ,and hypopituitarism may be caused by vascular occlusion by the lymphoid tumor cells in the hypothalamus or pituitary gland[3,9].It is unclear why selective growth of tumor cells occurs[3,9].Although we did not perform a pituitary biopsy,we diagnosed lymphoma infiltration of the pituitary gland based on poor evidence of other causes of hypopituitarism and pituitary gland enlargement;both conditions improved after chemotherapy.Although most patients of IVL with central nerves system involvement need intrathecal chemotherapy,most patients with pituitary involvement have responded to chemotherapy alone,as this case showed[10].
Although the common clinical or hormonal course after treatment for pituitary involvement with IVL remains uncertain because of the limited number of reported cases,early chemotherapy may be effective.Sawadaet al[3]described the case of a patient with hypopituitarism associated with IVL and the endocrinological course that followed.In this case,although the patient showed symptoms of panhypopituitarism before treatment,the levels of LH,FSH,TSH,ACTH,and prolactin returned to normal.She did not receive hormonal supplementation before and after chemotherapy.Sawadaet al[3]stated that hematological therapy at an earlier disease stage may contribute to better endocrinological prognoses,and that the amelioration of pituitary infarction by chemotherapy improves pituitary function when the damage is not irreversible,enabling avoidance of hormone replacement therapy.Our case supports their theory,as the function of the pituitary gland in our patient also partially improved after chemotherapy.The infarction-related damage was not irreversible.
CONCLUSION
In conclusion,we observed a case of IVL with hypopituitarism as a rare complication,which was diagnosed antemortem and successfully treated.Although early chemotherapy is effective,the clinical diagnosis of IVL is challenging.On encountering cases with a variety of symptoms that cannot be explained reasonably,general physicians should consider IVL.Additionally,the mechanisms of lymphomaassociated hypopituitarism associated with IVL have not yet been elucidated,necessitating further case studies and laboratory-based research.
猜你喜欢
杂志排行

World Journal of Clinical Oncology的其它文章
- GOECP/SEOR clinical recommendations for lung cancer radiotherapy during the COVID-19 pandemic
- B-cell lymphoma-2 inhibition and resistance in acute myeloid leukemia
- Combination drug regimens for metastatic clear cell renal cell carcinoma
- Circular RNA and its potential as prostate cancer biomarkers
- Statins in risk-reduction and treatment of cancer
- Novel molecular targets in hepatocellular carcinoma