Thought and Method on Establishing the Prediction Model of TCM Dominant Population with Advanced Digestive Tract Malignant Tumors based on TCM Tumor Registration Platform
2020-04-20XUYuying徐钰莹YANGYufei杨宇飞FENGLiHOULiYIDanhui易丹辉LIUJian
XU Yu-ying (徐钰莹), YANG Yu-fei (杨宇飞), FENG Li (冯 利),HOU Li (侯 丽), YI Dan-hui (易丹辉), LIU Jian (刘 剑)
1. Graduate School of Beijing University of Chinese Medicine, Beijing 100029, China
2. Xiyuan Hospital, China Academy of Chinese Medical Sciences, Beijing 100091, China
3. Cancer Hospital, Chinese Academy of Medical Sciences, Beijing 100021, China
4. Dongzhimen Hospital, Beijing University of Chinese Medicine, Beijing 100700, China
5. School of Statistics, Renmin University of China, Beijing 100872, China
ABSTRACT Advanced digestive tract malignant tumors, represented by advanced colorectal cancer,advanced gastric cancer and advanced esophageal cancer, have insidious onsets and high mortality.Western medicine based on targeted therapy greatly can improves the benefit and efficacy for patients through population stratification, but its population is limited. Traditional Chinese medicine (TCM) has a long history in treatment of tumors, which is an important part of comprehensive treatment of tumors.Clinical observation has shown that different patients could get different efficacy from TCM treatment.Based on real world registration studies, patients with advanced colorectal cancer, advanced gastric cancer or advanced esophageal cancer who had received TCM treatment were observed and followed, and a TCM dominant population that achieved significant efficacy was screened out to carry out multivariate regression analysis, further explore key factors that affect survival in advanced digestive tract malignant tumors, and establish a prediction model of TCM dominant population. It will provide reference for the follow-up TCM treatment, and provide reference for development of individualized treatment plans, making the TCM treatment for advanced digestive tract malignant tumors more targeted, and helping to improve the benefit rate in TCM.
KEYWORDS Registration; Advanced colorectal cancer; Advanced gastric cancer; Advanced esophageal cancer; Dominant population of TCM; Discriminant analysis; Prediction model
The high incidence and mortality of advanced digestive tract malignant tumors seriously threaten life and health of Chinese people. According to the latest national statistical data of cancer released by National Cancer Center in January 2019, deaths from malignant tumors accounted for 23.91% of all deaths in residents. Among them,the incidence of digestive tract malignant tumors represented by colorectal cancer, gastric cancer and esophageal cancer accounted for 26.4% of all malignant tumors, while the mortality accounted for 28.49% of all malignant tumors, more than the ones of lung cancer, which used to be in the first place[1]. Although Western medicine treatment,which is based on targeted therapy, has already entered a stage of individualized stratified treatment,significantly prolonging survival time in patients with advanced tumors, factors like stringent inclusion criteria, severe side effects and narrow coverage for people make some patients unable to receive the treatment, so survival data in patients with advanced digestive tract malignant tumors in the real world are still not optimistic. Registry data from 77,490 cases of advanced colorectal cancer within 21 continuous years showed that the median overall survival (OS)in advanced colorectal cancer in the real world was approximately 11 months, and from 1988 to 2008,the median OS increased from 8 months to 14 months[2]. The best level of OS in advanced gastric cancer and esophageal cancer in Western medicine ranged from 10 to 16 months, and the longest median OS in the best supportive treatment was only 5 months[3-6], with high cost, poor quality of life and long-term hospitalization.
Advanced digestive tract malignant tumors cannot be cured, and TCM has certain advantages in assisting Western medicine in routine treatment or single treatment. Many studies reported that TCM medicine can prolong survival time of patients with advanced malignant tumors, alleviate clinical symptoms and improve quality of life[7-13], but no high quality evidence has been shown to prove the efficacy. Therefore, from the earliest systematic review and meta analysis to randomized controlled trial, and to reestablishment of the standard model of TCM comprehensive efficacy in advanced colorectal cancer through retrospective continuous cases, Professor YANG Yu-fei's team made a series of attempts and explorations. Finally, it was found that only by finding the population that is more sensitive to TCM efficacy, that is the TCM dominant population, and digging out their characteristics,can better serve TCM clinical treatment for tumors,further prove the TCM efficacy, give full play to the TCM advantages, and better combine the TCM and Western medicine. If the sensitivity and benefits of patients to TCM can be predicted in advance before the start of TCM treatment, new thought and methods will be provided for the TCM to treat advanced malignant tumors. Based on the above thought and supported by Special Projects of Capital Scientific Research on Health Development in 2016, Professor YANG Yu-fei combined with a team of Professor HOU Li from Department of Hematology and Oncology in Dongzhimen Hospital of Beijing University of Chinese Medicine (BUCM), and a team of Professor FENG Li from Cancer Hospital of Chinese Academy of Medical Sciences (CAMS). This study was carried out with advanced digestive tract malignant tumors as a breakthrough point, in order to explore characteristics of TCM dominant population with advanced digestive tract malignant tumors and establish a prediction model of TCM dominant population on the basis of real world registration studies.
CONSTRUCTION OF TCM TUMOR REGISTRATION PLATFORM AND COLLECTION ON MALIGNANT TUMOR REGISTRATION INFORMATION
In the early stage of the study, a data platform was established, a website called "TCM Tumor Registration Platform" was developed,and its design and development on webpages was completed. The data display system of tumor patients, follow-up system, data analysis system,entry system of electronic case report forms (CRF),scientific research quality monitoring system of the supervision company, and background management system for the systems were established on the platform. Then, experts were organized for discussion to formulate extracting factors of TCM tumor registration information, and construct the tumor registration platform in cooperation with information departments of Xiyuan Hospital of China Academy of Chinese Medical Sciences (CACMS),Dongzhimen Hospital of BUCM, and Cancer Hospital of CAMS. First of all, registration accounts were opened to the 3 cooperative hospitals.After logging in, the 3 hospitals could share the registration data and progress. According to preset screening conditions, eligible cases were included in a case database of this study in real time (Shown in Figure 1. for the platform framework). There was a total of 473,078 person-times and 162,509 patients'outpatient service and hospitalization malignant tumor registration information collected through the platform form Xiyuan Hospital of CACMS,Dongzhimen Hospital of BUCM, and Sanhuan Caner Hospital - a medical treatment alliance of Cancer Hospital of CAMS. Among them, there were 286,946 person-times (56,386 patients) from Xiyuan Hospital of CACMS, 71,658 person-times (25,512 patients)from Dongzhimen Hospital of BUCM, and 114,474 person-times (80,611 patients) from Sanhuan Caner Hospital (the medical treatment alliance of Cancer Hospital of CAMS). According to different data on patients' outpatient service and hospitalization,tumor-related information was divided into outpatient service and hospitalization data sets, which were dynamically displayed through intuitive data such as report forms, icons, self-service enquiries,comparative analysis, etc.. A patent on this TCM Tumor Registration Platform has been applied, with a patent number of 201910002252.0.
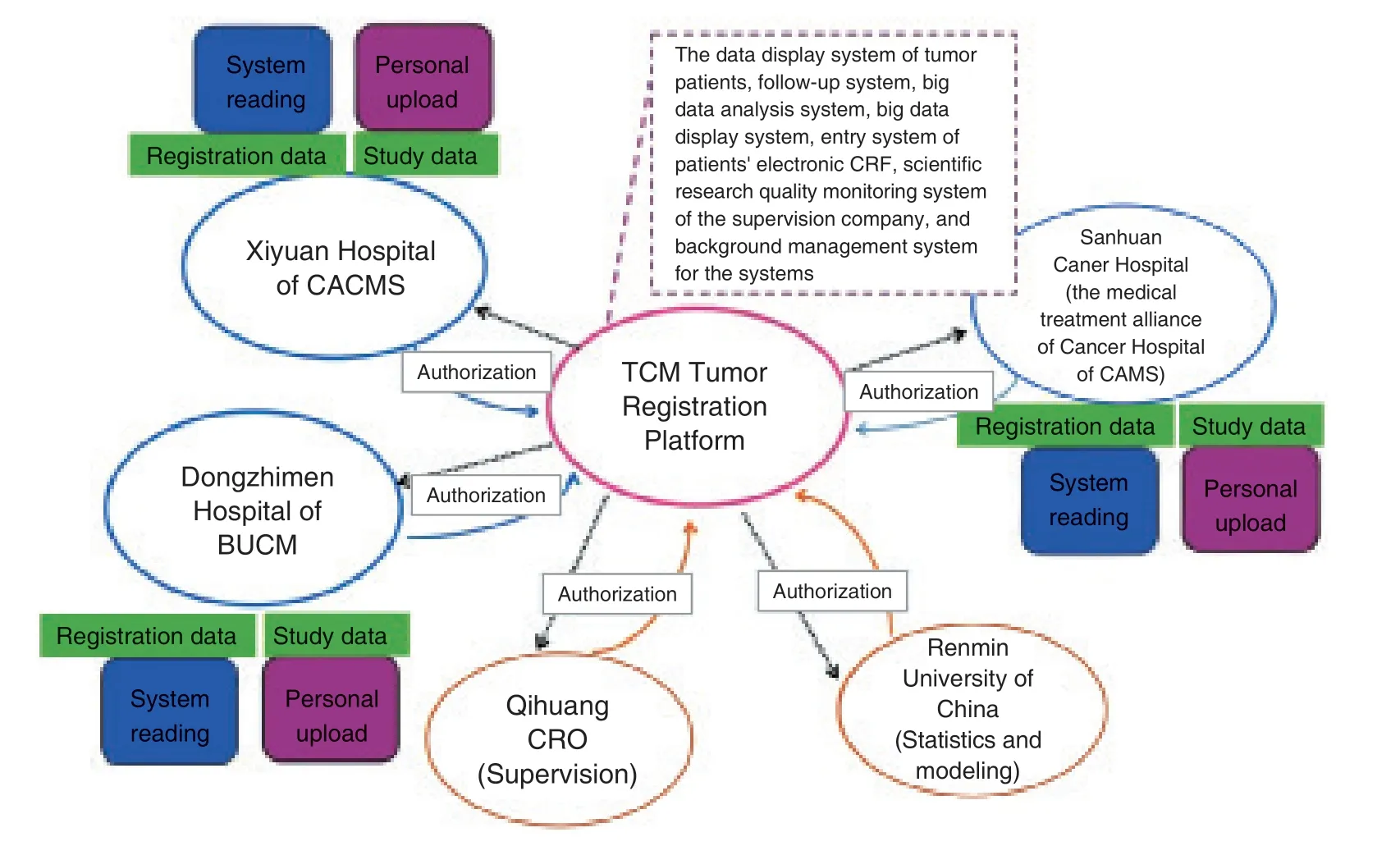
Figure 1. Framework of TCM Tumor Registration Platform
SCREENING ADVANCED DIGESTIVE TRACT MALIGNANT TUMOR CASES MEETING INCLUSION CRITERIA
Before the study was carried out, screening criteria were set up on the platform to screen cases according to diagnostic criteria, as well as inclusion and exclusion criteria, etc.. Before the study was implemented, it had been approved by medical ethics committees in the 3 hospitals respectively,and the ethical review approval numbers were 2016XLA136-1, 2016XLA156-1 and 16-114/1193.All the patients enrolled in the study had signed informed consent forms.
Diagnostic Criteria
Diagnostic criteria referred to WHOPathology and Genetics,Tumors of the Digestive System[14].Staging criteria referred to AJCC (American Joint Committee on Cancer) 7th Edition TNM (Tumor Node Metastasis) staging of colon cancer, rectal cancer, esophageal cancer and gastric cancer[15].The TCM standard of syndrome differentiation referred toClinic Terminology of Traditional ChineseMedical Diagnosis and Treatment - Syndromes[16]andGuiding Principles for Clinical Study on New Chinese Materia Medica[17].
Inclusion and Exclusion Criteria
Inclusion criteria: (1) Pathological diagnosis was colorectal cancer, gastric cancer or esophageal cancer. (2) TNM staging was Stage Ⅳ. (3) The age was 18-80 years old, with no limitation on gender. (4)Patients had received or would receive systematic TCM treatment (oral administration of decoctions based on TCM oncologists' treatment based on syndrome differentiation). (5) Karnofsky performance score (KPS) was no less than 60 points.
Exclusion criteria: (1) Patients previously had or were complicated with 2 or more kinds of malignant tumors. (2) There were non-neoplastic severe diseases and dysfunction, active cerebrovascular diseases, or uncontrolled infection and metabolic diseases in the patient's liver, kidney, heart or other major organs.(3) Patients could not take decoction and needed intravenous nutrition. (4) Patients suffered from malabsorption syndrome or other diseases affecting gastrointestinal absorption, or suffered from active peptic ulcers. (5) Pregnant women, breast-feeding women and mental patients were excluded.
Removing criteria: (1) Patients had complications or special physiological changes that researchers thought they were not suitable to continue the trial. (2) Patients did not meet the inclusion criteria and had been mistakenly included.(3) During the trial, patients' compliance was poor,which could affect the final result judgment.
Basis for Calculation on Sample Size
This study intended to use multivariate regression analysis. According to the results of previous retrospective pre-analysis, the number of TCM dominant population accounted for about 30% of the total number of survivors of advanced malignant tumors. Analysis factors were 10 variables of age, gender, genotyping, location of onset, location of metastasis, TCM syndrome,KPS, TCM intervention time, improvement degree of main TCM symptoms and life quality score.The sample size was calculated according to the principle of 5-10 times of the variables. The number of samples should be at least 5 times of the number of variables. Considering the study basis of colorectal cancer in the earlier stage in the oncology department of Xiyuan Hospital of CACMS and the possible 10% shedding rate in the study, the sample size of colorectal cancer cases should not be less than 120 cases, esophageal cancer cases should not be less than 80 cases, and gastric cancer cases should not be less than 80 cases.
After platform screening, patients who met the inclusion criteria were screened out, with a total of 228 cases of advanced colorectal cancer, 90 cases of advanced gastric cancer, and 100 cases of advanced esophageal cancer. In fact, there were 120 cases of advanced colorectal cancer, 80 cases of advanced gastric cancer and 80 cases of advanced esophageal cancer included (Shown in Figure 2. for the screening flow chart).
OBSERVATION AND FOLLOW-UP,DEFINING AND SCREENING TCM DOMINANT POPULATION BASED ON TCM DOMINANT POPULATION OF ADVANCED DIGESTIVE TRACT MALIGNANT TUMORS
Collection on Baseline Information
At the time of inclusion, baseline information was collected, including demographic characteristics,medical history, personal life history, treatment experience, major clinical symptom scores related to the diseases [referred to pain NRS (numerical rating scale) classification[18], using an interval (0-10 points) to represent different degrees of symptoms,namely, 0 was asymptomatic, and 10 was the most serious symptoms], life quality scores (Chinese version of MADASI scale), physical strength scores(KPS scale), TCM syndrome differentiation (mainly the syndromes with the highest frequency recorded in the case observation table), etc.. The above information was truthfully filled in the CRF form and typed into the TCM Tumor Registration Platform by 2 people at a time.
Follow-up

Figure 2. Screening Chart on Cases Included
After inclusion, an automatic follow-up reminder and a follow-up progress reminder were carried out through the TCM Tumor Registration Platform.Most cases were followed up and managed by informationized, automated and remote methods such as mobile terminals and media interaction(WeChat platform), while information of the rest was regularly collected and recorded by traditional outpatient return visits, inviting patients to return to the hospital for regular examination, or phone calls. The follow-up mainly included the survival situation of the patient, improvement in major clinical symptoms, physical strength score, life quality score,TCM syndrome differentiation, TCM prescriptions and methods, combined application of Chinese patent medicines, and other tumor related treatment situations (with or without chemotherapy or radiotherapy, and its course of treatment), etc.. The follow-up was conducted once every 2 months until the study's end or the patient's death. The CRF form was filled in truthfully, and the collected information was typed into the TCM Tumor Registration Platform for storage.
Quality Control on Data
In order to ensure rigor of the study as well as authenticity and reliability of the data, this study was equipped with a 3-level quality control (hereinafter referred to as "quality control") to ensure accuracy of the study data from the original records to the paper CRF forms and then to the input on the platform. Among them, a third-party data monitoring company was entrusted to be responsible for the quality control on data from the original records to the paper CRF forms. The company was required to check integrity of the records, ensure accuracy of filling the CRF forms, ensure the timely followup and timely filling for cases, verify the data at the same time, and know the progress of the included patients. If there were any errors and omissions, the company needed to ask the researchers to correct,keep the original records, and give clear indication of the correcting date and staff in the correcting places. After the paper CRF forms were filled in,a method of real-time input by 2 people was used to type information on the paper CRF forms into the TCM Tumor Registration Platform to improve the accuracy of data input. At the same time, the platform was equipped with basic data verification rules. According to ranges and mutual relations of each index value in the CRF forms, data checks on the ranges and logic were set, and corresponding computer programs were wrote for preliminary correction on the input data and control on data input errors. Meanwhile, a specially-assigned person was responsible for the 3-level quality control on the study to check consistency between the platform data and information on the case report forms. He could query traces left on the platform online, and the data inputter could answer the query online.
Classification Criteria
After the follow up in this study, according to the patients' final survival results and standards on TCM dominant population formulated earlier,the patients were grouped. That is, based on the concept of TCM dominant population with advanced malignant tumors formulated earlier (namely advanced malignant tumor survivors, who have received both standardized treatment in modern medicine and synchronous TCM treatment, have longer survival time than average survival time in those who have received modern standardized treatment based on the guidance of evidencebased medicine, or advanced malignant tumor survivors, who have received TCM treatment without standardized treatment in modern medicine, have longer survival time than other survivors' average survival time, and they are referred to as the TCM dominant population) and study data on the survival time of advanced colorectal cancer, advanced gastric cancer and advanced esophageal cancer home and abroad[19-27], the expert consultation method was applied to consult 39 TCM or Western medicine oncologists with a title of chief physician in China, so as to formulate the standard on TCM dominant population with advanced colorectal cancer. The time was counted until the patient's death or the last follow-up. There were patients with all genes of wild-type, and the survival time of StageⅣ more than 30 months, patients with RAS gene mutation, and the survival time of Stage Ⅳ more than 24 months, patients with BRAF gene mutation,the survival time of Stage Ⅳ more than 18 months,and patients without receiving gene detection, but the survival time of Stage Ⅳ more than 18 months.However, the standard on TCM disadvantaged population was those who reached the end of survival with the survival time of Stage Ⅳ no more than 12 months. Those between the two were the middle population, namely, the remaining population excluding the TCM dominant population and the TCM disadvantaged population. The standard on TCM dominant population with advanced gastric cancer was that as of the death of the patient or the last follow-up time, the survival time of Stage Ⅳwas no less than 333 days. The standard on TCM disadvantaged population with advanced gastric cancer was that as of the last follow-up time, the patient had died with the survival time of Stage Ⅳno more than 332 days. The standard on the middle population with advanced gastric cancer was that as of the last follow-up time, the patient was still alive with the survival time of Stage Ⅳ no more than 332 days. The standard on TCM dominant population with advanced esophageal cancer was that as of the death of the patient or the last follow-up time,the survival time of Stage Ⅳ was no less than 11.1 months. The standard on TCM disadvantaged population with advanced esophageal cancer was that as of the last follow-up time, the patient had died with the survival time of Stage Ⅳ less than 11.1 months. The standard on the middle population with advanced esophageal cancer was that as of the last follow-up time, the patient was still alive with the survival time of Stage Ⅳ less than 11.1 months.
STATISTICAL ANALYSIS, EXPLORING PROGNOSTIC FACTORS IN ADVANCED DIGESTIVE TRACT MALIGNANT TUMORS AND ESTABLISHING THE PREDICTION MODEL OF TCM DOMINANT POPULATION WITH ADVANCED DIGESTIVE TRACT MALIGNANT TUMORS
Statistical analysis in this study was operated by R software, withP<0.05 indicating statistically significant difference. According to the survival results in advanced colorectal cancer, advanced gastric cancer and advanced esophageal cancer, the survival time of patients in Stage Ⅳ was calculated by a calculation formula. The survival time of StageⅣ = the time of the patient's death or the last follow up - the discovery time of Stage Ⅳ. Taking the survival time as a dependent variable, and the other relevant factors as independent variables, a Cox model with a form of "h(t,X) =h0(t) exp (β1x1+β2x2+ … +βpxp)" was established, in which "h0(t)"was the basis hazard rate, and "x1,x2…xp" were factors. Prognostic factors were screened by the Cox proportional hazard model, and the key factors affecting the survival of advanced colorectal cancer,advanced gastric cancer and advanced esophageal cancer were explored in combination with clinical experience.
According to the screening results on prognostic factors from the Cox proportional hazard model of advanced colorectal cancer, advanced gastric cancer and advanced esophageal cancer,and combined with clinical experience, relevant variables were also included as discriminant factors,i.e. independent variables, for establishment of the prediction model of TCM dominant population.The classification results of the TCM dominant population, the TCM disadvantaged population and the middle population were taken as the dependent variable, Four discriminant functions of quadratic discriminant analysis (QDA), linear discriminant analysis (LDA), mixed discriminant analysis (MDA)and flexible discriminant analysis (FDA) were established to discriminate and predict population characteristics. Results of function prediction and results of actual population classification were compared, and the function model with the best prediction effect was selected as the final prediction model of the TCM dominant population. It was verified that the model had high prediction accuracy,of which the total prediction accuracy was 84.2%in advanced colorectal cancer, 67.1% in advanced gastric cancer and 65% in advanced esophageal cancer (Shown in Figure 3).
PRACTICAL APPLICATION OF THE PREDICTION MODEL OF TCM DOMINANT POPULATION WITH ADVANCED DIGESTIVE TRACT MALIGNANT TUMORS
The prediction model for TCM dominant population with advanced digestive tract malignant tumors can automatically predict a new patient's population classification. The probability of the TCM dominant population can be calculated by the following formula.


Figure 3. Statistical Analysis Flow Chart
In the formula,yrepresents the dependent variable, namely, a patient belonging to the TCM dominant population or not. The value ofKcan be 1, 2 or 3, in which 1 indicates the TCM dominant population, 2 indicates the middle population, and 3 indicates the TCM disadvantaged population. X is a vector, which indicates a selected discriminant factor, namely, an important factor that affects a patient's result of belonging to the TCM dominant population or not. The corresponding probability can be calculated by inputting the screened discriminant factor, that is, a variable parameter. For example, by inputting a screened relevant discriminant variable of a patient with advanced colorectal cancer, the following contents can be obtained, "The probability that this patient belongs to the dominant population is 0.843 6, indicating that the patient belongs to the dominant population". Thus, the patients can be predicted. Embedding the model program into the TCM Tumor Registration Platform can realize real-time application of the model and real-time population classification.
CONCLUSION
In traditional clinical studies, artificial screening is often used to screen patients for inclusion. To some extent, it increases bias in clinical trials. This ideal clinical trial condition dominated by subjective consciousness is far from the actual medical environment, and the results obtained are often not sufficient to reflect effectiveness of relevant treatment in the actual medical environment, nor are they sufficient to respond to various complex problems faced by both doctors and patients under the actual medical conditions. Therefore, this study established the TCM Tumor Registration Platform for TCM tumor data registration, case screening for inclusion, follow-up reminding, clinical monitoring,statistical analysis, etc., which not only improves the TCM tumor registration research system, but also closely combines information technology, big data and clinical practice.
At present, there are many treatment methods for digestive tract malignant tumors. As an individualized and well-established therapy with years of history, TCM has played a unique role in the treatment of malignant tumors. However, through continuous clinical practice, it is found that different tumor populations have different sensitivities to TCM treatment. For this reason, Professor YANG Yu-fei formally put forward the concept of TCM dominant population with tumors at the 9th Chinese Conference on Geriatric Oncology in 2015, and took advanced colorectal cancer as an attempt to carry out a series of studies. He had preliminarily discovered some characteristic trends in the TCM dominant population[27-30]. Although previous studies reported that discriminant analysis can be used to assist clinical diagnosis, predict disease developmental trends and explore distribution rules of TCM syndromes[31-35], there was not any study report on applying the discriminant analysis to predict the TCM dominant population with tumors.Therefore, on the basis of previous studies, the sample size was further enlarged, advanced colorectal cancer, advanced gastric cancer and advanced esophageal cancer, three diseases with high incidence rates and hidden onsets which are incurable were included and analyzed. The key factors affecting the survival of advanced digestive tract malignant tumors were explored. The sensitivity and effectiveness of advanced digestive tract malignant tumor patients to TCM treatment were predicted by establishing a prediction model of TCM dominant population. The results showed that the total prediction accuracy of the prediction model in advanced colorectal cancer was 84.2%, that in advanced gastric cancer was 67.1%, and that in advanced esophageal cancer was 65%.
In this study, information technology was applied to the field of TCM treating advanced digestive tract malignant tumors, which to a certain extent promoted transformation on medical and health service mode and management mode in TCM. The TCM routine research approach on tumors was transformed to start from the TCM dominant population with good efficacy to explore the key factors affecting the survival of advanced digestive tract malignant tumors. Establishment of the prediction model of the TCM dominant population provides reference for patients with advanced digestive tract malignant tumors to receive TCM treatment or not, contributes to further improving efficacy of TCM on tumors, and better meeting the growing demand for medical services of people, and lays a foundation for its popularization to other tumor studies.
