Effect of electroacupuncture at Huantiao (GB 30) and Weizhong (BL 40) on serum IgG and IgM in rabbits with lumbar intervertebral disc herniation
2018-03-13FengYingshuai封迎帅LiuBaixiang刘百祥LinYaping林亚平LiJun李俊YangDawei阳大为
Feng Ying-shuai (封迎帅), Liu Bai-xiang (刘百祥), Lin Ya-ping (林亚平), Li Jun (李俊), Yang Da-wei (阳大为)
1 Department of Traditional Chinese Medicine of Hunan Provincial People’s Hospital, Changsha 410005, China
2 School of Acupuncture, Moxibustion & Tuina, Hunan University of Chinese Medicine, Changsha 410007, China
Lumbar intervertebral disc herniation (LIDH) is a common and frequently-occurring disease with clinical symptoms of low back pain and/or sciatica[1]. Clinical and experimental studies have shown that electroacupuncture (EA) has confirmed therapeutic effects on LIDH. LIDH patients showed improved or alleviated clinical symptoms, such as lumbar and leg pain, limited motion and sciatica, after EA treatment[2-4], but the underling mechanism is still controversial. The clinical symptoms, physical signs, degree of intervertebral disc herniation and the nerve root compression are not exactly the same in LIDH patients. Therefore, the theory of nervous mechanical compression cannot fully explain the mechanism of LIDH[5]. Serum immunoglobulin G(IgG) and immunoglobulin M (IgM) are important products of the immune response in the body. The occurrence or increase of IgG and IgM in LIDH patients may be the results of autoimmune reaction in the prominent intervertebral disc[6]. Immunoassay for LIDH patients showed increased positive rate of IgG,suggesting that the immune response might be an important cause of LIDH[7]. In this study, we focused on the autoimmune reaction of LIDH to observe the changes of thigmesthesia function, gait function,expression levels of serum IgG and IgM in experimental rabbits with LIDH after EA at Huantiao (GB 30) and Weizhong (BL 40), thus to explore the related immunological mechanisms of EA for LIDH .
1 Experimental Materials
1.1 Experimental animals
A total of 40 healthy adult New Zealand purebred rabbits were provided by the Experimental Animal Center of Hunan Provincial People's Hospital Clinical Research Center (general level), half male and half female with body weight of 1.5-2.0 kg. Each rabbit was housed separately in the second laboratory of Experimental Animal Center in Hunan Provincial People's Hospital Clinical Research Center. Rabbits were fed at the temperature of 20-25 ℃, and humidity of 50%-70%, with sufficient light and free access to standard diet and drinking water. The handling of animals during the experiments was in line with the requirements of theGuiding Opinions on the Treatment of Experimental Animalsissued by the Ministry of Science and Technology of the People's Republic of China[8].
1.2 Materials and reagents
Hwato Brand acupuncture needles of 0.30 mm in diameter and 25 mm in length (Suzhou Medical Appliance Factory, China); G6805-2 mode EA instrument (Qingdao Hua Qing Instrument Factory,China); IgG and IgM ELISA kit (Wuhan Xinqidi Biological Technology Co., Ltd., China).
1.3 Statistical methods
All data were analyzed using SPSS 19.0 software for Windows. First of all, normality test and homogeneity of variance test were performed. The data in normal distribution were presented as mean ± standard deviation (x±s). Pairedt-test was used for intra-group comparison before and after intervention. One-way ANOVA was used to compare the differences among multiple groups. The least significant difference (LSD)was used when the variance was homogeneous and Tamhane's T2 method was used when the variance was not homogeneous.P<0.05 indicated a statistical significance.
2 Experimental Methods
2.1 Animal groups
Using the quadratic random method, the rabbits were divided into a blank control group, a model group,an EA at acupoint group and an EA at non-acupoint group according to random number table method, with 10 rabbits in each group. All rabbits were fasted for 1 day, while with free access to water. Except for rabbits in the blank control group, rabbits in the other three groups were subjected to LIDH modeling[9]. Lumbar intervertebral disc CT examination was performed for the randomly selected rabbit samples after the successful modeling. Intervention started according to the grouping from the second day after modeling.
2.2 Modeling method and standards for identification of the successful modeling
2.2.1 Modeling method
A LIDH model maker, reformed from a maxillary sinus puncture needle of 1.6 mm in diameter according to the literature, was used to establish the LIDH models[9].The median incision next to the left lower abdomen was performed under aseptic conditions to expose both the anterior longitudinal collateral ligament before the intervertebral space and the area behind the intervertebral space.
The LIDH model maker was inserted by 7.80-8.00 mm to the right with a 45° angle at the L6-L7intervertebral space. Syringe was fixed and the intervertebral disc tissue in the syringe was push to the front of the posterior longitudinal ligament with a caput planum wick-in-needle, resulting in the right side LIDH model at L6-L7. Stitched the wounds, and the rabbits were sent back to the animal feeding room.
2.2.2 Standards to determine the success of models
Observation of lower limb nervous function: The lower limb nervous function of rabbits was observed and compared before and after modeling. Rabbit gait was scored according to the recommended neurological function criteria in the literature[10].
There were no statistically significant differences in neurological function scores of the lower extremities among groups before modeling. Except for the blank control group, the neurological function scores of rabbits’ lower extremity in the other three groups after modeling were significantly lower than those before modeling (P<0.01), indicating that the gait function in rabbits was weakened after successful modeling.
CT examination: Lumbar CT examination for modeling rabbits was performed after anesthesia before and after modeling, respectively (Figure 1).
Rabbit's nucleus pulposus herniation to the internal spinal canal after modeling indicated the intervertebral disc herniation and successful modeling.
2.3 Point positioning
Point positioning was performed according to the commonly-used animal point positioning method in theExperimental Acupuncture Science[11].
Huantiao (GB 30): At the 1/3 middle and outside intersection of the line between the highest point of the femur greater trochanter and the sacral fissure of rabbit.
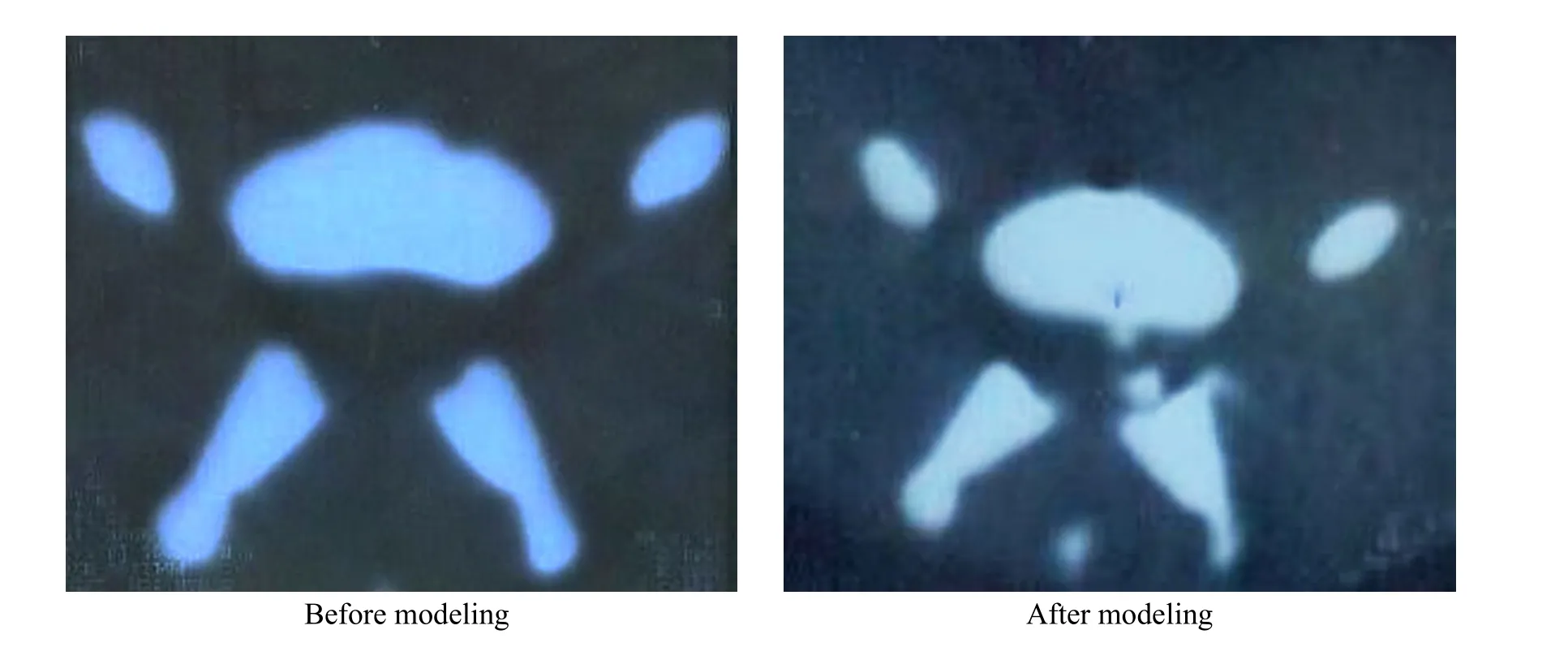
Figure 1. CT findings before and after modeling
Control point of Huantiao (GB 30): Non-acupoint,2 cm above Huantiao (GB 30).
Weizhong (BL 40): In the depression of the posterior knee joint.
Control point of Weizhong (BL 40): Non-acupoint,0.5 cm medial to Weizhong (BL 40).
2.4 Treatment methods for rabbits in each group
Blank control group: Rabbits were fixed for 20 min using the rabbit fixing box without acupuncture treatment.
Model group: Rabbits were fixed for 20 min using the rabbit fixing box without acupuncture treatment.
EA at acupoint group: Rabbits were fixed using the rabbit fixing box. Huantiao (GB 30) and Weizhong (BL 40)on the affected side were selected. After shearing and sterilizing, acupuncture needles of 0.3 mm in diameter and 25 mm in length were inserted directly by a depth of 1 cm. A group of output wires of the G6805-2 EA instrument were respectively connected to Huantiao(GB 30) and Weizhong (BL 40). Negative pole was connected to Huantiao (GB 30), and positive pole was connected to Weizhong (BL 40). Sparse-dense wave was used. The frequency of sparse wave was 30 Hz and the dense wave was 100 Hz. The current of 0.5-1.0 mA was used to keep the hind limbs of rabbits slightly tremulous.Each stimulus lasted for 20 min.
EA at non-acupoint group: Control points of Huantiao(GB 30) and Weizhong (BL 40) were selected. Negative pole was connected to the control point of Huantiao(GB 30), and positive pole was connected to the control point of Weizhong (BL 40). Acupuncture methods and EA parameters were the same as those in the EA at acupoint group.
2.5 Specimen collection and treatment
All rabbits were anesthetized with 20% urethane[4 mL/(kg·bw)]. Four milliliter of carotid artery blood was collected and kept at room temperature for 2-3 h,then centrifuged at 3 000 r/min for 15 min at 4 ℃.The supernatant was stored at -20 ℃ after aliquoted in EP tubes for later measurement.
2.6 Observed items
2.6.1 Thigmesthesia function test for the limbs
Thigmesthesia function score was conducted by gently touching the affected toes with a cotton swab,according to the neurological function standards in the literatures[10]. 0 point: no any reaction; 1 point: slight reaction of affected limbs; 2 points: affected limbs had flexion or extension reaction, but the reaction was slow.3 points: reaction of affected limbs was quicker, but slightly worse than the healthy side; 4 points:thigmesthesia of the affected side was sensitive and showed no difference compared with the healthy side.2.6.2 Determination of limb gait function
The gait of rabbit was observed for gait score with reference to the literature[10]. 0 point: affected limbs were panplegia without autonomic activities; 1 point:affected limbs were semiplegia with muscle contraction and slight joint movement; 2 points: affected limbs showed poor strength, slow joint movement and walking instability; 3 points: affected limbs only showed interphalangeal joint dyskinesia; 4 points: recovered to normal exercise.
2.6.3 Serum IgG and IgM tests
Serum IgG and IgM were detected by enzyme-linked immunosorbent assay according to the kit instructions.
3 Results
3.1 Results of thigmesthesia function
There was no significant difference in thigmesthesia score among groups before modeling (P>0.05). The thigmesthesia function scores of the same group before and after modeling were compared: except for the blank control group, the thigmesthesia scores of the other three groups after modeling were significantly lower than those before modeling (allP<0.01),indicating that the thigmesthesia function of the rabbits after modeling was weakened. Comparing of the thigmesthesia function scores before and after treatment in the same group: thigmesthesia function score was significantly improved in the EA at acupoint group after treatment (P<0.01), while there was no statistically significant difference in other groups before and after treatment (allP>0.05). Comparison of thigmesthesia score differences after treatment among groups: the EA at acupoint group was significantly higher than the blank control group, model group and EA at non-acupoint group (allP<0.01), suggesting that the thigmesthesia function was significantly improved by EA at Huantiao (GB 30) and Weizhong (BL 40), thus showing a positive therapeutic effect of EA at Huantiao(GB 30) and Weizhong (BL 40) on dysfunction of thigmesthesia function in LIDH rabbits (Table 1).
3.2 Results of gait scores
There was no significant difference in gait score among groups before modeling (P>0.05). The gait scores before and after modeling in the same group were compared: except for the blank control group, the gait scores of rabbits in the other three groups after modeling were significantly lower than those before modeling (allP<0.01), indicating that the walking function was weakened after modeling. Comparison of the gait scores before and after treatment in the same group: the gait score after treatment in EA at acupoint group was significantly higher than that before treatment (P<0.01), but no statistically significant intra-group differences in gait scores were found in other groups (allP>0.05). Comparison of gait score difference after treatment among groups: EA at acupoint group was significantly higher than the blank control group, model group and EA at non-acupoint group (allP<0.01), suggesting that the walking function of LIDH rabbits was significantly improved by EA at Huantiao (GB 30) and Weizhong (BL 40), thus showing a positive therapeutic effect on dysfunction of walking function in LIDH rabbits (Table 2).

Table 1. Comparison of rabbits’ thigmesthesia function scores (x±s, point)

Table 2. Comparison of rabbits’ gait scores (x±s, point)
3.3 Serum IgG and IgM levels
Serum IgG and IgM levels in the model group were significantly higher than those in the blank control group (allP<0.01). The serum levels of IgG and IgM in the EA at acupoint group were significantly lower than those in the model group and EA at non-acupoint group(P<0.05). Serum IgG and IgM levels in EA at non-acupoint group were not statistically different compared with those in the model group, suggesting that the EA at Huantiao (GB 30) and Weizhong (BL 40)could inhibit serum IgG and IgM expressions in LIDH rabbits (Table 3).
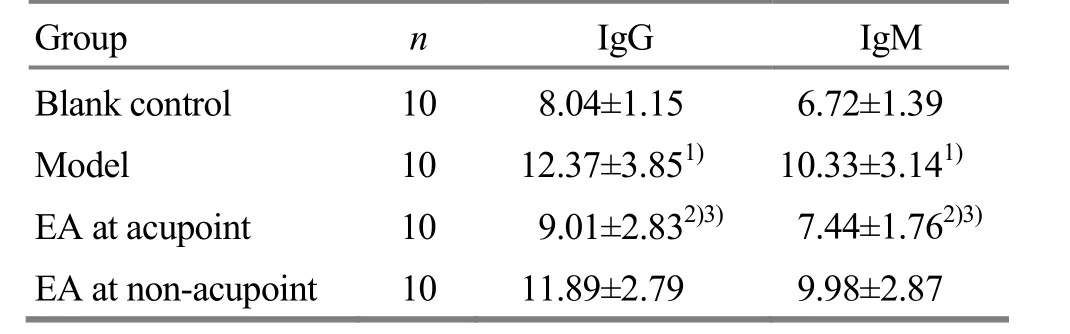
Table 3. Comparison of the levels of IgG and IgM expressions(x±s, μg/mL)
4 Discussion
LIDH falls under the category of ‘Bi-impediment syndrome’, ‘low back and leg pain’ or ‘Wei-flaccidity syndrome’ in Chinese medicine. It can be caused by either ‘obstruction’ or ‘malnourishment’. Obstruction occurs when exogenous wind, cold and dampness or traumatic injuries causes qi stagnation or blood stasis.Malnourishment occurs when long-lasting pain damages the liver and kidney or the failure of kidney qi to nourish the muscles or sinews due to constitutional liver and kidney deficiency. Consequently, the onset,development and treatment of LIDH are closely associated with meridians, qi, blood and functions of the Zang-fu organs.
Studies have found that the degree of lumbar disc herniation and nerve root compression, severities of clinical symptoms and physical signs in LIDH patients are not exactly the same[5]. Therefore, some people have questioned the opinion that compression and stimulationto the nerve root by the herniated nucleus pulposus are the main cause of low back and leg pain in LIDH patients[12]. It is believed that the mechanism of LIDH is not completely explained by mechanical compression of the nerve root alone, which may be closely related to the inflammatory response caused by biochemical substances in diseased intervertebral disc tissues[13]and autoimmune reactions[14-15]. Autoimmune response is also an important factor that causes low back pain and sciatica[14]. Intervertebral disc is an avascular tissue in the body. The nucleus pulposus is surrounded by the fibrous ring to make it isolated from the outside, thus has certain auto-immunogenicity, so the nucleus pulposus can be called ‘hidden antigen’. If the fibrous ring is ruptured, the nucleus pulposus will bulge from the ruptured fibrous ring and expose to the body's immune system, which can cause autoimmune reactions, lead to low back and leg pain, and other symptoms[14,16]. A study found that during the early phase of nucleus pulposus herniation in the noncompressive LIDH rats, T cell-mediated immune response caused nerve root injury, leading to radicular pain[17]. After LIDH modeling, IgG level in the body of rats was increased. Scraping treatment inhibits the autoimmune response induced by the nucleus pulposus and the inflammatory response mediated by autoimmune response, therefore, the immune abnormalities recover to the normal[18]. IgG and IgM are immunoglobulins in the body that reflect the body's immune status. The severity of LIDH is closely related to the expression level of IgG and IgM in the body[19-22].IgM shows stronger antigen binding ability and is the earliest appeared antibody during the initial humoral immune response. IgG is synthesized and secreted by the plasma cells in spleen and lymph nodes, and is the main antibody produced during the secondary humoral immune response. It is a high-affinity antibody that plays an important role in immune defense. Serum IgG and IgM are significantly elevated in LIDH patients, and acupuncture combined with herb-partitioned moxibustion can modulate humoral immunity in LIDH patients, leading to the IgG and IgM levels in patients to the normal[23]. Increased IgG and IgM levels in LIDH patients are thought to be the result of autoimmune response in intervertebral disc tissue[18]. Acupuncture can effectively reduce the levels of blood IgG and IgM in LIDH patients, decrease the secretion of immunoglobulin, and reduce the deposition of immune complexes in the lumbar intervertebral discs and surrounding tissues, thereby reducing the local inflammatory response in the intervertebral discs[24].
Area of the low back and leg pain caused by LIDH is similar to paths of the Bladder Meridian and Gallbladder Meridian. The two branches from the lumbus and back of the Bladder Meridian both meet at Weizhong (BL 40). Weizhong (BL 40) is the He-Sea point of the Bladder Meridian, and the common acupoint used in the treatment of low back and leg pain.Huantiao (GB 30) is a crossing acupoint of the Bladder Meridian and Gallbladder Meridian, and can be used to treat low back and leg pain related to the Bladder Meridian and Gallbladder Meridian. Gallbladder controls bone-induced diseases, and bladder controls tendon-induced diseases. Acupuncture at Huantiao(GB 30) and Weizhong (BL 40) has the role to smooth the tendons and help the joints, used in the treatment of low back and leg pain, bones and muscles pain of lower limbs and other related diseases.
There are a lot of records about the treatment of low back and leg pain by Weizhong (BL 40) and Huantiao(GB 30) in the TCM classics from different ages.Therefore, Huantiao (GB 30) and Weizhong (BL 40) are the commonly used acupoints in the treatment of low back and leg pain. In this study, we observed the effects of EA at Huantiao (GB 30) and Weizhong (BL 40) on the expression of serum IgG and IgM in LIDH rabbits. We found that the thigmesthesia and walking functions of rabbits were decreased, and the levels of IgG and IgM in serum were increased significantly after modeling.After EA at Huantiao (GB 30) and Weizhong (BL 40),thigmesthesia and walking functions of rabbits were improved significantly, and serum IgG and IgM levels were significantly lower than those in the model group and EA at non-acupoint group; thigmesthesia and walking functions, and serum IgG and IgM levels in EA at non-acupoint group had no significant difference compared with those in the model group, suggesting that the autoimmune reaction may be related to the condition of LIDH, which is consistent with that being reported in domestic and foreign literatures[16,18,24],indicating that EA at Huantiao (GB 30) and Weizhong(BL 40) in regulation of LIDH rabbit serum immune response has a relative acupoint specificity effect. Based on the results above, it is concluded that the improvement of clinical symptoms, including thigmesthesia and gait score, of rabbits after treatment indicates that EA at Huantiao (GB 30) and Weizhong(BL 40) benifits LIDH rabbits. Prominent nucleus pulposus in LIDH rabbits can cause autoimmune response. EA at Weizhong (BL 40) and Huantiao (GB 30)can regulate the abnormal autoimmune reactions caused by autoantigen exposure due to the prominent nucleus pulposus in LIDH rabbits. Inhibition of the excessive immune response to nucleus pulposus autoantigen, thereby inhibiting of the initiation and progression of various inflammatory responses and alleviating clinical symptoms, may be one of the mechanisms during the treatment of LIDH. However,due to the small sample size, the limited experimental observation time (two courses) to detect the LIDH rabbit serum IgG and IgM levels in this trial, the real effect of EA at Huantiao (GB 30) and Weizhong (BL 40)on serum IgG and IgM levels in LIDH rabbit with a large sample size or under different experimental observation times remain to be further explored.
Conflict of Interest
The authors declared that there was no potential conflict of interest in this article.
This work was supported by Scientific Research Project of Hunan Provincial Administration of Traditional Chinese Medicine (湖南省中医药管理局科研资助项目, No.201378).
Statement of Human and Animal Rights
The treatment of animals conformed to the ethical criteria in this experiment.
[1] Wu ZD, Wu ZH. Surgery. 7th Edition. Beijing: People’s Medical Publishing House, 2008: 849-854.
[2] Feng YS, Liu BX, Yang DW. Clinical observation of electroacupuncture at Huantiao (GB 30) and Weizhong(BL 40) on lumbar intervertebral disc protrusion. Liaoning Zhongyiyao Daxue Xuebao, 2015, 17(3): 116-119.
[3] Feng YS, Liu BX, Zhang L, Yi SX, Yang DW. Effect of electroacupuncture at Huantiao (GB 30) and Weizhong(BL 40) points on rabbits with lumbar intervertebral disc protrusion. Hunan Zhongyiyao Daxue Xuebao, 2014,34(11): 53-56.
[4] Yang ZB, Feng YS, Yi SX, Wu X, Wu HX, Cao JY.Experimental research on the sciatic nerve lesion reparation in LIDP by electroacupuncture at Huantiao (GB 30) point.Zhonghua Zhongyiyao Zazhi, 2012, 27(1): 202-204.
[5] Liu YM, Wu YG, Wang ZT, Cui Y. Changes of lumbar facet joint angles and far lateral lumbar disc herniation.Zhongguo Gu Yu Guanjie Sunshang Zazhi, 2012, 27(3):250-252.
[6] Habtemariam A, Grönblad M, Virri J, Seitsalo S,Ruuskanen M, Karaharju E. Immunocytochemical localization of immunoglobulins in disc herniations. Spine(Phila Pa 1976), 1996, 21(16): 1864-1869.
[7] Zeng JX, Liang B, Yin D, Wen ZH, Chen F, Wang X, Gu J,Chu Y. MMP-3, IgG and CD68 expressions in the herniated nucleus pulposus between young and elder patients.Zhongguo Jizhu Jisui Zazhi, 2013, 23(12): 1109-1115.
[8] Ministry of Science and Technology of the People's Republic of China. Guiding Opinions on the Treatment of Experimental Animals (2006-09-30) [2017-06-20].http://www.most.gov.cn/fggw/zfwj/zfwj2006/200609/t2006 0930_54389.htm.
[9] Shen WD. New Animal Model Establishment and Experimental and Clinical Research of the Pathological Mechanism of Lumbar Disc Protrustion. Changsha: Doctor Thesis of Central South University, 2004: 8-17.
[10] Siegal T, Siegal T, Shapira Y, Sandbank U, Catane R.Indomethacin and dexamethasone treatment in experimental neoplastic spinal cord compression: part 1.Effect on water content and specific gravity. Neurosurgery,1988, 22(2): 328-333.
[11] Li ZR. Experimental Acupuncture Science. Beijing: China Press of Traditional Chinese Medicine, 2007: 327-329.
[12] Yuan W, Li XL, Dong J, Zhou XG, Ma YQ, Zhou J, Wang HR. A middle-long term follow-up results of different surgical treatment methods for multiple lumbar disc disease.Zhongguo Gu Yu Guanjie Sunshang Zazhi, 2011, 26(9):769-771.
[13] Zhu G, Zhang SQ, Huang B, Zhuang JH, Gao QX, Liu JH,Chen DJ. Correlation between TNF level and pain induced by lumbar disc herniation. Beijing Zhongyiyao Daxue Xuebao, 2010, 17(4): 8-9.
[14] Liu C, Shou KQ, Fu NX, Li J, Huang H.Experimental study on the abnormal autoimmunity in the model of ruptured lumbar disc herniation. Zhongguo Jizhu Jisui Zazhi, 2013, 23(1): 61-65.
[15] Zhang HP, Zhang F, Yao Y. Autoimmune properties of nucleus pulposus in the patients with lumbar disc herniation. Zhongguo Zuzhi Gongcheng Yanjiu, 2012,16(48): 8931-8937.
[16] Capossela S, Schläfli P, Bertolo A, Janner T, Stadler BM,Pötzel T, Baur M, Stoyanov JV. Degenerated human intervertebral discs contain autoantibodies against extracellular matrix proteins. Eur Cell Mater, 2014, 27:251-263.
[17] Yuan WJ, Yuan ZW, Wang RY, Hu JZ. Autoimmune research on nerve root injury induced by non-compressive nucleus pulposus protrusion. Zhongguo Mianyixue Zazhi,2015, 31(4): 545-550.
[18] Chen H, Xu GH, Jiang RR, Li XC, Guo Y. Effects ofGua Shaon IgG in serum and pathological changes of disc tissue of rats with lumbar disc herniation. Nanjing Zhongyiyao Daxue Xuebao, 2014, 30(5): 450-453.
[19] Liu JC, Zhao YQ. Caudal injection of compoundDansheninjection for the treatment of lumbar disc herniation and impact on serum IgG and IgM. Zhongguo Shang Can Yixue, 2012, 20(9): 54-56.
[20] Zhu LG, Chen X, Yu J, Gao JH, Wang SQ, Feng MS, Yin H.Effect of removing dampness and promoting diuresis method on IgG, IgM and IL-1β, IL-8 in serum of rats with autoimmunity induced by nucleus pulposus. Zhongguo Gushang, 2011, 24(4): 327-331.
[21] Tang ZH, Li N, Cao L, Zhang H, Ding G, Wang ZZ, Xiao W. Improvement ofYaobitongcapsules on prolapsed of lumbar intervertebral disc in rats and study on its mechanism. Xiandai Yaowu Yu Linchuang, 2014, 29(10):1086-1091.
[22] Zheng XB, Zhu QG, Lin YF, Liu TX. Clinical effects of manipulative reduction plus acupoint injection on lumbar disc herniation. Zhongyi Linchuang Yanjiu, 2016, 8(2): 13-16.
[23] Wei WZ, Ruan YD, Ning XJ, Zheng Z, Wen S, Xie YF,Hong XT, Cai ZJ. Clinical research on elongated needle combined with herb-partitioned moxibustion in the treatment of lumbar disc herniation. Zhongguo Zhen Jiu,2013, 33(8): 673-677.
[24] Ding JJ, Ling GD, Zhou ZT. Observation on changes of blood IgG and IgM in lumbar intervertebral disc protrusion treated by the third acupoints on the waist. Xin Zhongyi,2015, 47(2): 185-186.
猜你喜欢
杂志排行

Journal of Acupuncture and Tuina Science的其它文章
- Effects of different doses of ginger-partitioned moxibustion on trefoil factor 1, mucin 5AC and epidermal growth factor receptor in rats with spleen deficiency syndrome
- Effect of acupuncture at complementary acupionts on mast cells and histamine/bradykinin released by mast cells in the regions of acupionts
- Development of workplace-related Liver Meridian-depression scale
- Music electric stimulation of points for anxiety:a multi-center randomized controlled clinical trial
- Acupuncture plus bloodletting therapy for insomnia in blood stasis constitution: a clinical study
- Efficacy observation on acupuncture plus moving cupping with compound white mustard oil for lumbar myofascitis