椎体后凸成形术治疗骨质疏松性椎体压缩骨折后加固椎体再压缩危险因素分析
2017-08-01汪文龙陈吟海涌关立刘玉增陈小龙
汪文龙 陈吟 海涌 关立 刘玉增 陈小龙
椎体后凸成形术治疗骨质疏松性椎体压缩骨折后加固椎体再压缩危险因素分析
汪文龙 陈吟 海涌 关立 刘玉增 陈小龙
目的 探讨椎体后凸成形术治疗骨质疏松性椎体压缩骨折后加固椎体发生再压缩的危险因素。方法 回顾性分析 2 0 1 2 年 1 月至 2 0 1 4 年 1 月,我院收治的单节段骨质疏松性椎体压缩骨折并接受椎体后凸成形术患者共 2 5 2 例,根据患者随访影像学资料,将所有患者分为无压缩对照组和再压缩组,应用单因素和多因素分析研究导致椎体再压缩的可能因素,如年龄、性别、体质指数、是否为新鲜骨折、术前是否存在其它合并症、既往是否发生其它椎体压缩骨折、是否发生骨水泥渗漏、术前骨密度 T 值、注射骨水泥量、术前椎体压缩率、术后椎体压缩率、骨水泥是否与上下终板均接触、伤椎是否发生椎体内裂隙,推测其中可能导致术后加固椎体再压缩的危险因素。结果 术后发生再压缩 4 5 例,未再压缩者 2 0 7 例,压缩组术前合并其它合并症 4 0 例,未再压缩组 1 4 1 例;压缩组平均术前骨密度 T 值 ( -2.8 9±0.3 2 ),未再压缩组 ( -2.6 4± 0.2 9 );压缩组骨水泥与上下终板均接触者 1 3 例,未再压缩组 1 4 1 例;压缩组骨水泥发生椎体内裂隙者1 9 例,未再压缩组 4 4 例。单因素分析结果表明,术前存在其它合并症、术前骨密度 T 值、骨水泥与上下终板均接触在两组之间差异有统计学意义。多因素 L o g i s t i c 回归分析显示术前存在其它合并症 ( OR=0.2 2 3 ) 和术前骨密度 T 值低 ( OR=0.0 5 3 ) 是危险因素,骨水泥与上下终板均接触 ( OR=6.2 9 6 ) 是保护因素。结论 术前存在其它合并症和患者骨密度过低是椎体后凸成形术后加固椎体再压缩的重要危险因素,对有存在以上两种情况的患者进行密切观察随访十分重要。
骨质疏松;脊柱;椎体后凸成形术;骨折,压缩性;危险因素
骨质疏松性椎体压缩骨折 ( o s t e o p o r t i c v e r t e b r a l c o m p r e s s i o n f r a c t u r e,O V C F ) 是临床常见疾患,由其造成的局部疼痛和畸形严重影响生活质量[1]。椎体后凸成形术 ( p e r c u t a n e o u s k y p h o p l a s t y,P K P ) 通过球囊扩张椎体后注入骨水泥能够有效加固椎体,恢复椎体高度,减小后凸畸形,同时缓解疼痛,现已成为治疗 O V C F 的常规方法[2]。然而,文献中报道扩张加固后的椎体再次压缩的发生率 1 3% 左右,可导致椎体高度丢失和局部畸形加重[3-5]。通过对 2 0 1 2年 1 月至 2 0 1 4 年 1 月,因 O V C F 在我院行 P K P 的2 5 2 例患者的多种因素与椎体术后丢失高度进行相关性分析,旨在发现造成 P K P 椎体再压缩的危险因素,为临床工作提供有指导意义的信息。
资料与方法
一、纳入与排除标准
1. 纳入标准:( 1 ) 胸腰椎单节段 O V C F 行单节段 P K P;( 2 ) 术后随访时间>1 8 个月;( 3 ) 术后无明显外伤史;( 4 ) 术后抗骨质疏松治疗;( 5 ) 术后定期随访并行脊柱 X 线检查。
2. 排除标准:( 1 ) 非 O V C F;( 2 ) 骨折侵犯椎管伴神经功能损害者;( 3 ) 术前和 ( 或 ) 术后无法站立行走者;( 4 ) 术后出现邻近节段骨折;( 5 ) 无依从性患者或不能配合医师随访、检查者;( 6 ) 严重全身系统性疾病,如恶性肿瘤、严重器官功能紊乱者;( 7 )长期应用甾体类激素者。
二、一般资料
本研究共纳入患者 2 5 2 例,其中男 6 9 例,女1 8 3 例,所有患者均一期行单个椎体 P K P,其中 T51 例,T64 例,T76 例,T82 例,T91 例,T105 例,T111 1 例,T125 7 例,L18 9 例,L24 0 例,L32 2 例,L41 3 例,L51 例。年龄 5 1~9 2 岁,平均 ( 7 2.3± 9.7 ) 岁。所有患者均有术前、术后次日和术后 1 年以上随访时的站立位脊柱正侧位 X 线片、术前脊柱C T 平扫和 M R I ( 含压脂相 )。按 P K P 加固椎体是否发生再压缩分为再压缩组和未再压缩组。再压缩组4 5 例,发生率为 1 7.8 6% ( 4 5 / 2 5 2 ),其中男 1 3 例,女 3 2 例;年龄 5 8~9 1 岁,平均 ( 7 4.6±8.2 ) 岁。未再压缩组 2 0 7 例,男 5 6 例,女 1 5 1 例;年龄 5 1~9 2 岁,平均 ( 7 1.8±1 0.0 ) 岁。判定 P K P 加固椎体再压缩的标准:脊柱侧位 X 线片上末次随访伤椎前缘、中间或后缘高度较术后次日下降 4 m m 以上[3]。
三、观察指标
包括年龄、性别、体质量指数 ( b o d y ma s s i n d e x,B M I )、术前骨密度 T 值、骨折是否新鲜、术前是否伴有其它合并症 ( 包括原发性高血压 I I 级及以上,2 型糖尿病长期口服药物或胰岛素注射,冠状动脉粥样硬化性心脏病 )、是否发生骨水泥渗漏、既往其它椎体是否发生 O V C F、术中注射骨水泥量、术前椎体高度压缩率、术后椎体高度恢复率、骨水泥与上下终板是否均接触共 1 2 项。术前骨密度 T 值检测采用双光能骨密度检测仪测定的 L1~5椎体 T 值的平均值。判断为伤椎是否为新鲜骨折的标准为[6]:新鲜骨折:( 1 ) 病程<1 个月;( 2 ) M R I 提示伤椎 T1WI 和T2WI 均为高信号;陈旧骨折:( 1 ) 病程≥1 个月;( 2 ) M R I 提示伤椎 T1WI 高信号,T2WI 低信号。判断是否发生骨水泥渗漏以阅读术后脊柱正侧位 X 线片为主,部分诊断困难的患者行脊柱 C T 平扫。判断伤椎是否发生椎体内裂隙 ( i n t r a v e r t e b r a l c l e f t,I V C ) 采取如下影像学标准[7-8]:( 1 ) X 线片或 C T 表现椎体内半月形或不规则透亮区;( 2 ) M R I 表现为伤椎椎体内T1WI 低信号,T2WI 低信号或高信号,这可能由于裂隙内填充了液体或气体。椎体高度压缩率、术后椎体高度恢复率的计算方法如图 1。
四、统计学处理
使用 S P S S 2 2.0 软件进行统计学分析。单因素差异性分析中,连续变量符合正态分布和方差齐性时行独立样本 t 检验,不符合正态分布时行 M a n n-Wh i t n e y U 检验;分类变量行 χ2检验。以术后加固椎体再压缩与否作为应变量、单因素检验结果中差异有统计学意义的相关变量作为协变量,采用“进入”( E n t e r ) 的方法以 P<0.0 5 的标准筛选变量,得出相应的危险因素,建立 L o g i s t i c 回归模型。
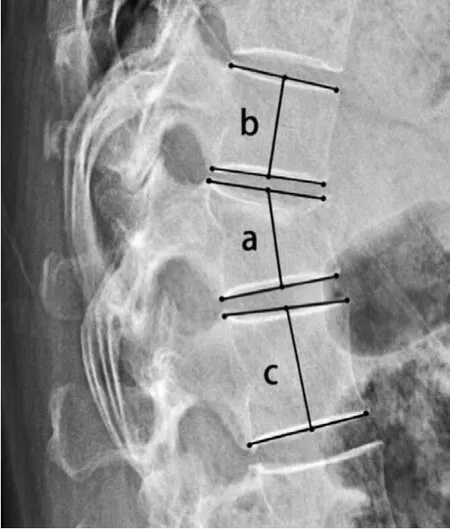
图1 测量椎体高度压缩率 ( a 为侧位片伤椎上下终板中点连线,b 为伤椎上位椎体上下终板中点连线,c 为伤椎下位椎体上下终板中点连线 ),椎体高度压缩率 = 1 - ( 2a / b + c ) × 100%;术后椎体高度恢复率 = 术后椎体高度压缩率 - 术前椎体高度压缩率Fig.1 Measurement of the compression rate ( Line a was between middle points of the upper and lower endplates; Line b was between middle points of the upper and lower endplates of the superior vertebral body; Line c was between middle points of the upper and lower endplates of the inferior vertebral body. Compression rate = 1 –( 2a / b + c ) × 1 00%; Restored rate = postoperative compression rate –preoperative compression rate
结 果
单因素分析:术前存在其它合并症、术前骨密度 T 值低、骨水泥与上下终板均接触和椎体内裂隙与 P K P 加固椎体再压缩有关 ( P<0.0 5 ),其余因素差异均无统计学意义 ( 表 1 )。多因素分析:术前存在其它合并症、术前骨密度 T 值低和椎体内裂隙是P K P 加固椎体再压缩的危险因素,骨水泥与上下终板接触是保护因素 ( 表 2 )。典型病例见图 2。

表1 影响 PKP 加固椎体再压缩的单因素分析Tab.1 Univariate analysis for occurrence of vertebral recompression after PKP
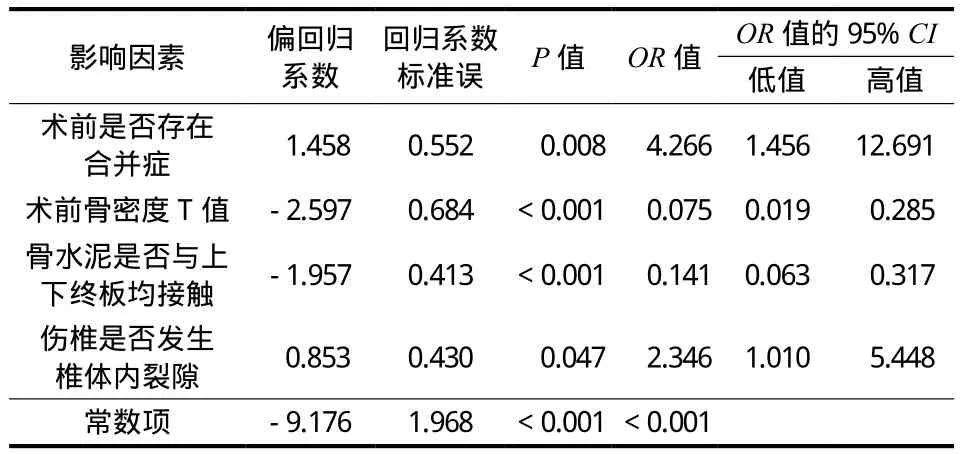
表2 影响 PKP 加固椎体再压缩的多因素 Logistic 回归分析结果Tab.2 Multivariate Logistic regression analysis for potential risk factors of vertebral recompression after PKP
讨 论
一、骨水泥分布与加固椎体再压缩的关系
C h e v a l i e r 等[9]通过对两种骨水泥的分布模型的有限元分析指出,骨水泥只与一侧终板接触时椎体刚度只增加 1~2 倍,强度几乎没增加;而当骨水泥与上下终板均接触时椎体刚度增加 1~8 倍,强度增加 1~1 1 倍。骨水泥只与一侧终板接触时手术椎体很容易发生再骨折。国内田伟等[10]认为,由于骨水泥刚度和强度明显高于骨组织,未被骨水泥填充的部分很容易发生再骨折,骨水泥未同时接触上下终板组的椎体再骨折的发生率是同时接触上下终板组的 1 2 倍。K i m 等[11]通过对尸体标本生物力学研究认为,P V P 骨水泥交错弥散于伤椎中,与上下终板接触,正因此负载可以在上下终板间传递。而 P K P骨水泥弥散较差,骨水泥未与上下终板接触,椎体高度更易丢失。手术应尽量使骨水泥周围交错分布且与上下终板接触。L i 等[12]对 3 4 例进行危险因素分析,得出骨水泥与上终板之间的距离是 P K P 手术椎体高度丢失的惟一因素。K i m 等[4]认为骨水泥团块与上下终板间存在骨松质区域是加固椎体再次骨折的主要原因。N i u 等[3]认为,P K P 骨水泥呈团块状分布周围骨质极易在日常活动中再次发生压缩。

图2 患者,女,67 岁,因“摔伤后腰背部疼痛 6 h”入院a~b:术前腰椎正侧位 X 线片示 L1椎体轻度楔形变;c:术前腰椎 CT 示 L1椎体轻度楔形变,终板完整,椎管内无异常;d~f:术前腰椎 MRI 提示 L1椎体等 T1、长 T2信号,脂肪抑制序列示 L1椎体高信号,T1、T2和脂肪抑制序列均可见椎体内存在条形低信号区,提示 IVC;g~h:术后腰椎正侧位 X 线片示术后骨水泥未与上终板接触;i~j:术后 13 个月随访示加固椎体高度丢失,局部后凸角度增加Fig.2 A 67-year-old female patient fell down 6 hours before the admission a - b: Preoperative anteroposterior & lateral lumbar X-ray films showed the wedging of L1vertebral body; c: Preoperative lumbar CT showed the wedging of L1without endplates fracture and occupied canal; d - f: Preoperative lumbar MRI showed the equal T1WI & long T2WI signal of L1, with long signal in STIR. All of them showed the linear low signal in L1vertebral body, which referred to intravertebral cleft ( IVC ); g - h: Postoperative anteroposterior & lateral lumbar X-ray fi lms showed that the cement didn’t touch the upper endplate; i - j: Films of 13 months’ follow-up showed the loss of vertebral height in strengthened vertebrae, with local kyphosis angle increased
本次研究中 9 8 例骨水泥未与上下终板接触患者中 3 2 例发生了椎体再压缩,发生率为 3 2.7%,显著高于骨水泥与上下终板接触的患者 ( 发生率为8.4% ),多因素回归分析提示骨水泥未与上下终板接触是 P K P 加固椎体发生再压缩的一个非常重要的因素,这与以上研究的结论一致。
二、骨密度与 P K P 再骨折的关系
T s e n g 等[13]通过大样本的 O V C F 患者的回顾性研究认为,高龄和骨密度较低是非手术椎体发生骨折的危险因素。刘法敬等[14]通过分析 P K P 治疗不同骨密度的 O V C F 疗效发现 2 例邻近椎体骨折患者,且均发生于骨密度值最低的组。但 L i 等[12]通过对 P K P 椎体再压缩的危险因素分析认为骨密度并非其危险因素。L i n 等[15]通过回顾性分析也发现椎体再压缩组和椎体未压缩组骨密度差异无统计学意义。本研究中 P K P 加固椎体再压缩组的骨密度 T 值明显低于未压缩组,多因素回归分析提示术前骨密度低是 P K P加固椎体发生再压缩的危险因素。
三、椎体内裂隙与 P K P 再骨折的关系
椎体内裂隙由 M a l d a g u e 等[16]首次报道,并认为可导致椎体缺血坏死骨折。最新的一篇 Me t a 分析指出[17]:存在 I V C 的 O V C F 术后椎体高度较低,骨水泥渗漏的发生率较高。高林等[18]伴有 I V C 的O V C F 术后骨水泥分布以团块状为主,而无 I V C 者以混合型分布为主,根据之前讨论的结果,弥散不佳呈团块状分布的骨水泥可能是造成加固椎体高度丢失和再压缩的重要原因。H e 等[19]回顾 O V C F 伴I V C 的病理机制后认为骨质疏松、缺血性骨坏死和骨折后生物力学改变是造成 I V C 的主要原因,伤椎这种缺血性骨坏死极有可能造成术后椎体骨质进一步塌陷和压缩,造成椎体高度丢失。张刚等[5]通过对单节段胸腰椎 O V C F 的研究认为 I V C 是 P K P 同一椎体再压缩的重要因素,本次研究也得出相同结论,研究认为 I V C 导致的骨水泥弥散不佳和缺血性骨坏死是导致这种结果的重要原因。
本次研究除纳入上述研究考虑到的危险因素如年龄、性别、骨密度、注射骨水泥量、骨水泥是否渗漏及骨水泥分布情况、是否存在椎体内裂隙等因素外,还增加了患者自身原因如 B MI、术前是否合并慢性疾病和既往是否发生 O V C F,同时分析了骨折新鲜与否、椎体压缩程度和术后椎体高度恢复程度等因素,均为临床上经常需要考虑和解决的问题。同时,本研究纳入的样本数量较多,随访时间也较其它同类研究为多。
目前对于 P K P 加固椎体发生再压缩现象报道较少,认识不足,临床上关注亦较少。但通过现有的资料进行的危险因素分析可发现术前存在其它合并症、术前骨密度 T 值绝对值大是造成 P K P 加固椎体再压缩的危险因素,骨水泥与上下终板接触能够预防这种现象的发生。本研究是回顾性研究,有一定的局限性,对于加固椎体再压缩现象的进一步研究亟待大样本、前瞻性和长期随访研究。
[1]Wang E, Yi H, Wang M, et al. Treatment of osteoporotic vertebral compression fractures with percutaneous kyphoplasty: a report of 196 cases[J]. Eur J Orthop Surg Traumatol, 2003, 23(Suppl 1):S71-75.
[2]Zhai W, Jia Y, Wang J, et al. The clinical application and efficacy of percutaneous kyphoplasty via unilateral pedicular approach guided by CT image measurement[J]. Int J Clin Exp Med, 2015, 8(11):20861-20868.
[3]Niu J, Zhou H, Meng Q, et al. Factors affecting recompression of augmented vertebrae after successful percutaneous balloon kyphoplasty: a retrospective analysis[J]. Acta Radiol, 2015, 56(11):1380-1387.
[4]Kim YY, Rhyu KW. Recompression of vertebral body after balloon kyphoplasty for osteoporotic vertebral compression fracture[J]. Eur Spine J, 2010, 19(11):1907-1912.
[5]张刚, 周建伟, 邹德威, 等. 骨质疏松椎体压缩性骨折行椎体后凸成形术后同一椎体再压缩相关因素研究[J]. 腰腿痛杂志, 2014, 35(4):245-249.
[6]史光华, 李鹏翠, 张蜀华, 等. 椎体后凸成形术治疗新鲜性与陈旧性骨质疏松椎体压缩骨折的疗效分析[J]. 中国骨伤, 2013, 26(10):820-823.
[7]Theodorou DJ. The intravertebral vacuum cleft sign[J]. Radiology, 2001, 221(3):787-788.
[8]Libicher M, Appelt A, Berger I, et al. The intravertebral vacuum phenomen as specific sign of osteonecrosis in vertebral compression fractures: results from a radiological and histological study[J]. Eur Radiol, 2007, 17(9):2248-2252.
[9]Chevalier Y, Pahr D, Charlebois M, et al. Cement distribution, volume, and compliance in vertebroplasty: some answers from an anatomy-based nonlinear finite element study[J]. Spine, 2008, 33(16):1722-1730.
[10]田伟, 韩骁, 刘波, 等. 经皮椎体后凸成形术后骨水泥分布与手术椎体再骨折的关系[J]. 中华创伤骨科杂志, 2012, 14(3):211-215.
[11]Kim MJ, Lindsey DP, Hannibal M, et al. Vertebroplasty versus kyphoplasty: biomechanical behavior under repetitive loading conditions[J]. Spine, 2006, 31(18):2079-2084.
[12]Li D, Wu Y, Huang Y, et al. Risk factors of recompression of cemented vertebrae after kypholosty for osteoporotic vertebral compression fractures[J]. Int Orthop, 2016, 40(6):1285-1290.
[13]Tseng YY, Yang TC, Tu PH, et al. Repeated and multiple new vertebral compression fractures after percutaneous transpedicular vertebroplasty[J]. Spine, 2009, 34(18): 1917-1922.
[14]刘法敬, 杜伟, 申勇, 等. PKP 治疗不同骨密度椎体压缩骨折的手术疗效分析[J]. 中国脊柱脊髓杂志, 2012, 22(4): 324-329.
[15]Lin WC, Lee YC, Lee CH, et al. Refractures in cemented vertebrae after percutaneous vertebroplasty: a retrospective analysis[J]. Eur Spine J, 2008, 17(4):592-599.
[16]Maldague BE, Noel HM, Malghem JJ. The intravertebral vacuum cleft: a sign of ischemic collapse[J]. Radiology, 1978, 129(1):23-29.
[17]Yu W, Liang D, Yao Z, et al. The therapeutic effect of intravertebral vacuum cleft with osteoporotic vertebral compression fractures: A systematic review and metaanalysis[J]. Int J Surg, 2017, 40:17-23.
[18]高林, 闫亮, 郝定均, 等. 椎体内裂隙对经皮椎体后凸成形术疗效的影响[J]. 实用骨科杂志, 2016, 22(6):482-485.
[19]He D, Yu W, Chen Z, et al. Pathogenesis of the intravertebral vacuum of Kummell’s disease[J]. Exp Ther Med, 2016, 12(2):879-882.
Risk factors of vertebral recompression after kyphoplasty for osteoporotic vertebral compression fracture
WANG Wen-long, CHEN Yin, HAI Yong, GUAN Li, LIU Yu-zeng, CHEN Xiao-long. Department of Orthopedics, Beijing Chaoyang Hospital, Capital Medical University, Beijing, 100020, China
HAI Yong, Email: spinesurgeon@163.com
Objective To investigate the risk factors of vertebral recompression after percutaneous kyphoplasty in the patients with osteoporotic vertebral compression fractures. Methods The clinical data of 252 patients with osteoporotic vertebral compression fractures who underwent single-level percutaneous kyphoplasty in our hospital from January 2012 to January 2014 were retrospectively reviewed. All the patients were divided into recompression group and non-recompression group according to the radiological data collected during the followup. Thirteen potential factors of vertebral recompression were assessed using univariate and multivariate analyses, including age, gender, body mass index, fresh fracture or not, other comorbidities or not, previous vertebral compression fracture or not, cement leakage or not, preoperative bone mineral density T-score, volume of polymethylmethacrylate injected, preoperative and postoperative vertebral compression rate, polymethylmethacrylate-endplates contact or not and intravertebral cleft or not. Results After the surgery, 45 patients experienced recompression of cemented vertebrae, and 207 patients ont. There were 40 patients with other preoperative comorbidities in recompression group, and 141 in non-recompression group. The mean preoperative bone mineral density T-scores were ( -2.89 ± 0.32 ) and ( -2.64 ± 0.29 ) in recompression group and non-recompression group respectively. There were 13 and 141 patients with polymethylmethacrylate-endplates contact in recompression group and non-recompression group respectively. There were 19 patients with intravertebral cleft in recompression group, and 44 in non-recompression group. Other preoperative comorbidities, preoperative bone mineral density T-score and polymethylmethacrylate-endplates contact showed statistically significant differences between the 2 groups by the univariate analysis. And the multivariatelogistic regression analysis indicated that combining with other comorbidities ( OR = 0.223 ) and low preoperative T-score ( OR = 0.053 ) were independent risk factors. However, the polymethylmethacrylate-endplates contact ( OR = 6.296 ) was a protective factor. Conclusions Combined comorbidities and low preoperative bone mineral density T-score are 2 important risk factors of recompression of cemented vertebrae after percutaneous kyphoplasty, and a careful follow-up is necessary for the patients with these factors.
Osteoporosis; Spine; Kyphoplasty; Fractures, compression; Risk factors
10.3969/j.issn.2095-252X.2017.07.016
R683.2, R591.1
2016-11-16 )
( 本文编辑:王萌 )
1 0 0 0 2 0 北京,首都医科大学附属北京朝阳医院骨科
海涌,E m a i l: s p i n e s u r g e o n@1 6 3.c o m