Competences for a culture of prevention*
2016-10-19BOLLMANNUlrike
BOLLMANN Ulrike
(Institute for Work and Health(IAG)of the German Social Accident Insurance(DGUV))
Competences for a culture of prevention*
BOLLMANN Ulrike
(InstituteforWorkandHealth(IAG)oftheGermanSocialAccidentInsurance(DGUV))
Work is changing.Traditional approaches to prevention fall short.A broader understanding of prevention and the cultural transformation associated with it mean that there are new demands on companies and their employees.People and organisations need competences for this transformation;they must be empowered to create humane living and working conditions.In order for people and organisations to be able to develop competences for the transformation,appropriate structural conditions in educational institutions and workplaces must be created.These conditions should enable people to experience a feeling of competence,to feel part of something and to perceive their actions as autonomous.
culture of prevention;competence;learning;transformation
0 Introduction
Work is changing.Traditional approaches to prevention fall short.A broader understanding of prevention and the cultural transformation associated with it mean that there are new demands on companies and their employees.People and organisations need competences for this transformation;they must be empowered to create humane living and working conditions.
Globalisation and digitalisation are not only changing the world of work,but also work itself.Work is losing itself in space and time,it is becoming “volatile”(mobile,transitory).[1]Thus,the boundary between working life and private life is becoming increasingly diffuse;the result is a “delimitation” of work.Due to digitalisation,which began in the middle of last century,we are currently experiencing a new phase of technological transformation,which is characterised by the “fusing of technologies,that is,the boundaries between the physical,the digital and the biological spheres are becoming blurred”[2].Smart products are “revolutionising” our working and private lives.
The core of prevention work is no longer just about preventing accidents and occupational diseases but also the promotion of physical and mental health.In addition to classic risk prevention,workplace health promotion and workplace integration management are becoming increasingly important.Furthermore,prevention is developing into an approach that covers all phases of life.The impetus for this holistic view of prevention came from the Ottawa Charter of the World Health Organization(WHO)in 1986.
The term culture of prevention describes both a broader understanding of prevention and a new level of quality for preventive action;safety and health are integrated into all activities and thus,become a self-evident,lived part of our professional and daily lives.A culture of prevention is not only based on laws,guidelines,standards and rules for safety and health,but is also based on a common,collective appreciation of safety and health,as well as taking into consideration what health and safety personally means for every individual.Thus,a culture of prevention is not only based on the explicit(formal rules and shared values)but also on the implicit,which we are often unaware of and is,therefore,even more effective[3].The call for creating a culture of prevention can be traced back to the European Community Strategy on Health and Safety at Work 2002-2006.The call for a culture of prevention to be implemented at national level across the globe followed in 2008 at the XVIII World Congress on Safety and Health at Work in Seoul,South Korea.
1 Competence instead of qualification
The term competence in its current usage comes from the field of psychology.Robert W.White introduced the term into the psychology of motivation back in 1959.A year later,Noam Chomsky established the concept of linguistic competence and the correlating distinction with performance[4].In the seventies,the term competence found its place in pedagogy.In vocational training and work sciences,competence superseded qualification as a term in the last decade of the 20th century[5].This “competence-focused revolution” can also be attributed to the changed framework conditions in the world of work[6].Since 2000,the term “competence” has been increasingly used,particularly in connection with the PISA studies(Programme for International Student Assessment)and the measurability of competences has become a dominant issue.This increasing use and narrowing of the term competence culminated in the OECD Skills Strategy of 2012 which states that competences “have become the global currency of the 21st century”[7].
In terms of a culture of prevention,the term competence is discussed in this paper based on two meanings: competence in the sense of abilities,skills and know-how,and competence in the sense of “responsibility”[9].The latter and older meaning of competence as responsibility goes back to the concept of competence in public law of the Roman Republic[8].Since the 1990s,the first meaning has typically been divided into four competence areas: technical,methodological,social and personal.However,this at first seemingly clear schema has a tendency to “overflow”: “Nowadays,one speaks also of emotional,creative,moral and even spiritual competences.Ultimately,you can put the word ”competence“ at the end of any activity”[5].As a result,a large catalogue of competences has been emerging which is supposed to express what someone should know and be able to do,as well as how to measure these competences.
In the meaning of competence in the sense of responsibility,the human and their actions are the focus.Here,competence is a social,if not social-political,category.In addition to the competences of each individual,competence here refers to “the granting of responsibility to all in order to increase humanity”[9],to participate in the design of our lives and our work.In this second meaning,someone is competent when they strive to “improve their circumstances” and thus,the humanity of human beings is reflected “in the humanity of the circumstances which they have created and are responsible for”[9-10].This involves communication not as a form of “conflict” but rather as a participative exchange on a common matter and a tendency towards symmetrical communication with mutual respect[9].
According to this understanding,considerate interaction with others in the world is a requirement for any communication and any social relationship(“primordial sociality” or “pre-communicative social relations”-based on Edmund Husserl,Maurice Merleau-Ponty,Alfred Sch tz)[9-12].
Competence refers here to the “transition from possibility to reality,from competence to performance,from knowledge to human action”[9].
2 Development of competences
Neither a culture of prevention nor a competence can be regarded as material objects.There is “no such thing’as a prevention culture”[13]and competences are likewise not directly observable: “Competences don’t lie around like tools in a box or pegs on a board(in our case in the brain,as neurophysiology would assert).Instead,they are generated situationally by the person who is acting”[5].Competences for a culture of prevention cannot be just depicted in a catalogue of competencies,but rather it is necessary to ask about the conditions under which a person or an organisation can develop competences and act competently.
Moreover competence is a basic human need.In addition to the need to feel close to others,to belong(be part of something)and the need for autonomy(feeling like your actions are self-determined),humans have a continuous need to develop their own efficacy and effectiveness in dealing with their environment[14-15].Which culture exists in a company,an organisation or a society depends mainly on whether,and to which extent,basic human needs can be met or not.
Furthermore competences develop as a result of learning.Here again there is a distinction between two meanings: between the idea of learning as an unbroken accumulation of knowledge,and learning as an experience[11].
Learning as an experience takes place as “relearning”: in learning,the learner has an experience about the experience itself[12].Moreover,the learner takes the position that it is not about knowledge but rather about the attitude towards the thing,towards oneself and towards others[11-16].Competences for a culture of prevention are based on learning as an experience.Learning as an experience is an integral part of the cultural transformation.In developing a culture of prevention,particular importance is placed on informal learning and learning in the process of working.
In addition to the development of individual competences,the focus of attention for some time now has been on the activation and development of competences in social systems.Organisational competence is understood to be the ability of organisations to continually develop innovative products and services which are either aligned to changing market requirements or contribute fresh impetus to the market[17].Organisational competences are the result of complex social-interaction processes which build up into collective action patterns in the sense of procedures.These action patterns are generally emergent,that is,without a core understanding of how and why this coordination works so well: “Organisational competence is far more embedded in the actions of the organisation’s members and is,therefore,only ”remembered“ in actions”[17].In addition to explicit knowledge,for example,technical and methodological knowledge,it is also very important for the development of organisational competence to have “tacit knowledge”[18]and narrative knowledge[17-19].
In times of accelerated technological change,competences need to be permanently flexible,as well as constantly renewed and further developed.“Leaders need to make brave decisions instead of sticking too long with strategies that were previously successful.Digitalisation,for example,means that certain business models simply no longer work and companies must do entirely new things[20].Of particular importance here is whether a company or organisation has“dynamic capabilities”[17].
3 Safety competence
A key element for the safety climate and safety culture in a company are rules and regulations,as well as the employees’attitude towards these.In this context,a distinction can be made between two models: a classical,rational top-down approach,which views rules as something static and the infringement of rules as negative behaviour,and a bottom-up approach,which perceives rules as dynamic,local and situated constructions.In the first case,the employee is at the forefront and is not allowed to make mistakes;in the second case,the employee is considered to be an expert whose competence is to adapt to the diversity of reality[21].A good error-learning culture,in which an error is not seen as a violation of rules but rather a learning opportunity,is thus a prerequisite for the development of safety competence.This competence cannot be substituted with a rule.On the contrary,it is rather the unwritten rules,the tacit rules and motivations that we can comply with or violate which make up the structure of organisational culture.The term “routines” is used to describe these unwritten rules.Routines result from experiences and repetition in a social context “in a way that is essentially informal and not written down.They form...the repository of organisational memory,and as such are necessarily subject to change as learning takes place”[21].
A direct link can be made between organisational routines and actions when faced with unpredictability and uncertainty.As opposed to a model of rationally-planned safety,Karl E.Weick developed an approach towards “managing the unexpected” based on James Reason’s concept of “an informed safety culture”.According to Weick,managing the unexpected means that people show “strong reactions to weak signals[22-23].The opportunity to learn and thus change is based on proactive and often uncomfortable behaviour,on detecting errors and taking them seriously.Karl E.Weick also speaks in this context of “mindful management”.In the style of the language philosopher Gilbert Ryle(1900—1976),mindfulness here is understood as the “disposition towards mindful,swift,cooperative and careful action”.This is associated with the expectation that “greater mindfulness means that it is more likely that unexpected or safety-critical situations can be dealt with”[24].Implicit knowledge(“tacit knowing”)and mindfulness are necessary “to exercise discretion in applying any rules that are defined,so that they are able to come up with adaptions,improvisations and extensions of them to cope with the unexpected and unforeseen situations”[21].
Andrew Hale and David Borys connect the model of rationally-planned safety and the model of dynamic adaptation to the situational context in a framework concept for managing rules with the following elements: the continuous observation and adaptation of rules,the involvement of the people who are to comply with the rules in the process of setting the rules,and regular,explicit dialogue with management and experts.
Due to the current speed of change and the accompanying loss of employee experience,thought is already being given to how the relationship between organisational routines and their effect on the dynamic of routines can be examined.For example,by forming clusters of routines,rules can be adapted and reinvented even more dynamically[25].
4 Health competence
At the beginning of this millennium,the concept of health competence in the context of work and health was introduced in German-speaking countries[26-27-15].
This concept is based on the term “health literacy” which the World Health Organisation(WHO)newly defined some ten years earlier.The original concept of “health literacy” was restricted to cognitive and social skills when dealing with health information.The new term was broader: “Health literacy implies the achievement of a level of knowledge,personal skills and confidence to take action to improve personal and community health by changing personal lifestyles and living conditions”[28].
On this basis,a structural model of health competence has been developed in Germany in the last few years which describes for the first time which skills and abilities are important for physical and mental health.The model distinguishes between basic health-related skills(for example,reading an instruction leaflet and being able to comply with a written regulation)and advanced health-related abilities such as health-related self-awareness(aware of one’s own feelings,needs and thoughts),actively taking responsibility(consciously deciding on health-promoting behaviour)and the ability to scrutinise health information.The central element in this structural model is the ability to guide one’s own health,together with the components of self-regulation and self-control[29].
Fundamental to this is the system-theoretical notion of an autopoietic system which can organise and adapt to changing conditions autonomously.Of particular importance when looking at health competence are self-determination theory[14]and Albert Bandura’s concept of self-efficacy.Mental health and well-being are dependent on the extent to which autonomous,motivated behaviour is possible and also on the person’s expectation,based on their own competences,that they can successfully perform the desired action.
WHO also speaks of “empowerment for health”.Whereas empowerment was initially about “a process through which people gain greater control over decisions and actions affecting their health”[28],today,empowerment is seen as a process “through which individuals and social groups are able to express their needs,present their concerns,devise strategies for involvement in decision-making,and achieve political,social and cultural action to meet those needs”[28-30].
Thus,health competence looks beyond the individual towards a “health-competent society whose goal is to empower its members to promote health and thereby make a substantial contribution to well-being and prosperity”[29].
5 Traditional approach to prevention versus culture of prevention
At the centre of the traditional prevention approach is technology,organisation and OSH management;the human being is generally viewed as a risk factor.Traditional prevention follows a functionalist,mechanistic paradigm which turns safety and health into tools for a higher,mainly economic,purpose.
At the centre of a culture of prevention are humans,namely in their social relationships: the way people perceive themselves and their fellow human beings;the pattern they follow to communicate with other people and things;the values and personal core convictions which guide their actions.
This type of “humanised prevention”[20]follows an interpretive paradigm and is interdisciplinary.It assumes “that cultural aspects and internal communication processes have a major impact on how prevention is understood and implemented”[31].Humanised prevention should not only be designed from the perspective of experts but also from the perspective of the people that are to be reached: “We need to revise our focus in prevention and look at people and their needs”[32].It is no longer just about bringing prevention services to the people,but first and foremost about understanding the person’s needs,thoughts and actions in order to then develop,with the person,the appropriate structures and services of prevention in terms of their living and working environments.
In order to avoid a possible misunderstanding,it should be made clear that humanised prevention is in no way opposed to technology,quite on the contrary,it takes on the challenges created by the new phase of technological transformation;prevention becomes an integral part of the technological transformation.Our intelligence ensures that safety and health are integrated into the development of every single product from the very start[33].
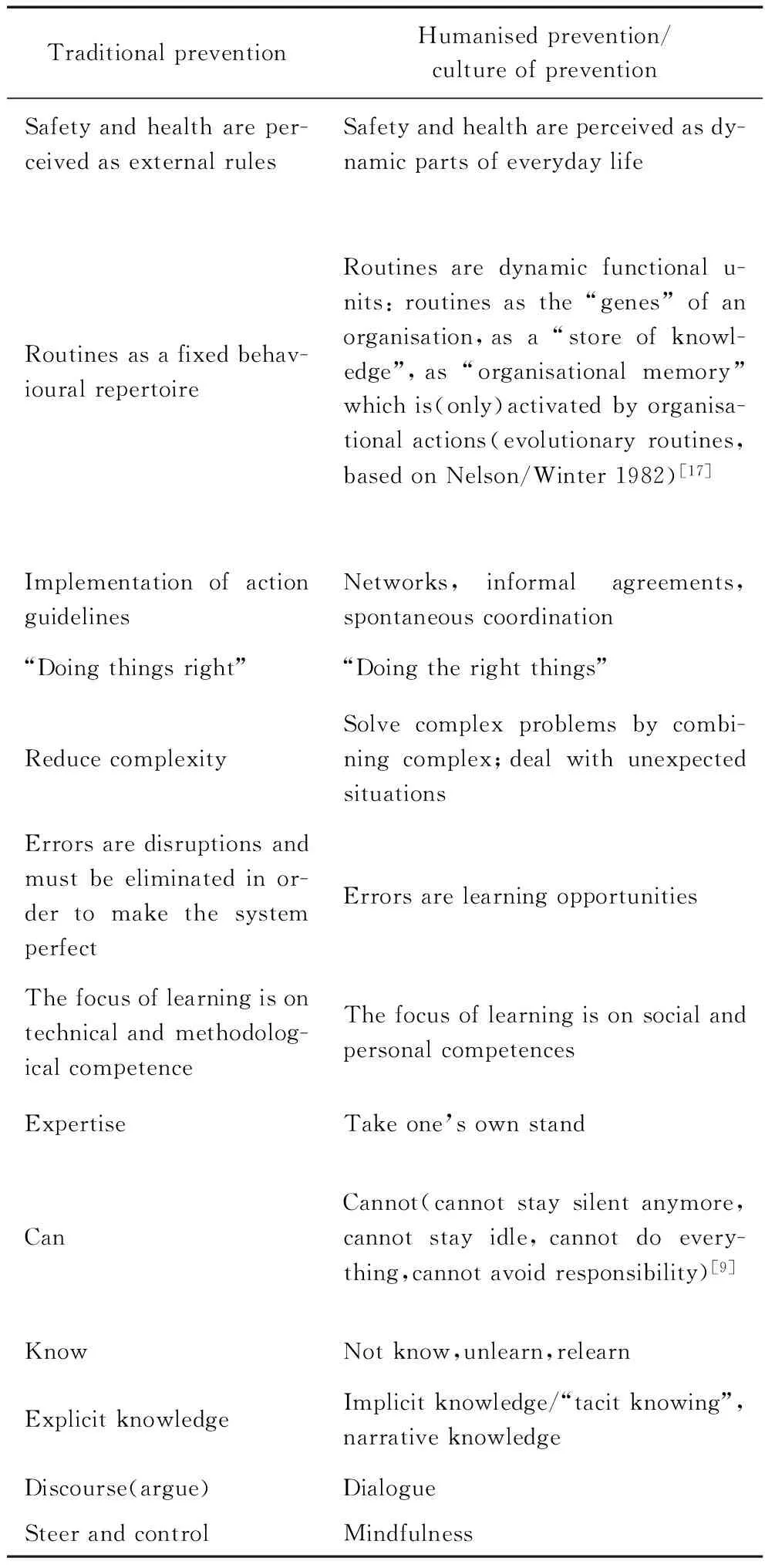
Tab.1 Comparison of approaches: traditional prevention
The design of humane living and working conditions requires skills to deal with the transformation.These competences cannot be “taught” in formal learning processes but rather must be acquired through one’s own experiences(learning as an experience).In order for people and organisations to be able to develop competences for the transformation,appropriate structural conditions in educational institutions and workplaces must be created.These conditions should enable people to experience a feeling of competence,to feel part of something and to perceive their actions as autonomous.
Learning as an experience can be made possible didactically when educational institutions create the necessary framework for self-organised learning processes which are open to the living and working environment of the learners[34].
Competence is developed primarily through implicit learning in the process of work and the social environment[34].One particular challenge of this is activating implicit knowledge(tacit knowing),that is,the knowledge or the ability which is not,or not fully,verbalised or formalised(unwritten rules).This is particularly true for each individual’s fundamental attitude towards safety and health,which was shaped either in earlier life cycles or by “critical events” in their life cycle[35].Here it is important to help raise learners’awareness of implicit knowledge and implicit beliefs[34].
6 Competencies for developing a culture of prevention
In 2017,the German Social Accident Insurance(DGUV)and its members are launching a prevention campaign to establish a culture of prevention at company level.The strategic concept of the campaign describes six fields of action to create a culture of prevention in companies: integration of safety and health into all activities;leadership;communication;participation;error-learning culture;social climate/company climate[36].At the centre of the campaign is the human being in their social relationships.The main idea of the campaign is that every employee can contribute to improving their work and private life through small actions in their everyday life.Prior to the campaign being promoted in companies and measures to promote a culture of prevention being implemented there,the current state of the six action fields will be determined within the DGUV and its member institutions.A special analysis tool called the “CultureCheck” will be used for this[37-38].Analysing the culture of prevention within its own “house” and then further developing it before the start of the campaign is considered an important prerequisite for ensuring the credibility of promoting cultural change at company level.
The new joint prevention campaign of the DGUV and its members is considered a suitable means of not only providing the necessary information regarding culture of prevention but also of assisting and accompanying the learning process needed for a cultural transformation both inside and outside the world of the social accident insurance institutions[39].
7 Conclusions
The design of humane living and working conditions requires skills to deal with cultural transformation.These competences cannot be just depicted in a catalogue of competencies nor can they be “taught” in formal learning processes.Competences for a culture of prevention are based on learning as an experience.To enable people to experience a feeling of competence,to feel part of something and to perceive their actions as autonomous,appropriate structural conditions in educational institutions and workplaces must be created.Which culture exists in a company,an organisation or a society depends mainly on whether,and to which extent,basic human needs can be met or not.The interrelationship between the development of a culture of prevention and the fulfillment of basic needs shall be further investigated in future as well as how to address the implicit(tacit knowing,patterns of behaviour),e.g.by practicing dialogue to explore the basic assumptions of people.

Tab.2 Competences for developing a culture of prevention
*The category of trust and its ambivalence in the context of safety and health must be considered separately.For example,a healthy balance between trust and mistrust is a prerequisite for a good error learning culture[21].Conversely,empathising with superiors can contribute to a lack of safe and healthy behaviour[31].
References
[1]Eichendorf,W.Interview at the 4thInternational Strategy Conference on Safety and Health (ISC2016),21-24 March 2016,DGUV Academy Dresden (Best-of-video),http://www.dguv.de/isc/documentation/index.jsp.
[2]Schwab,K.The Fourth Industrial Revolution,Geneva 2016.
[3]Schein,E H.Organizational Culture and Leadership,3rd edition,San Francisco 2004; 1st edition 1985.
[4]Heckhausen,H.Kompetenz.In: Historisches Wörterbu-ch der Philosophie,Vol.4,1976,pp.918-933.
[5]Faulstich,P.Kompetenz-Kompetenz-Reflexion eines zentralen Begriffs erfahrungsbezogener Bildungsforschung.In: Stock,Michaela u.a.(Hrsg.),Kompetent-wofür? Life skills-Beruflichkeit-Persönlichkeitsbildung.Beiträge zur Berufsbildungsforschung.Tagungsband zur 4.Österreichischen Konferenz für Berufsbildungsforschung am 3./4.Juli 2014,Innsbruck/Wien/Bozen 2015.
[6]Sprafke,N.Kompetente Mitarbeiter und wandlungsf hige Organisationen.Zum Zusammenhang von Dynamic Capabilities,individueller Kompetenz und Empowerment,Wiesbaden 2016.
[7]OECD.Better skills,better jobs,better lives.A strategic approach to skills policy,2012[8]Redecker,F.v.Kompetenz.In: Historisches Wörterbuch der Philosophie,Vol.4,1976,pp.918-933.
[9]Schaller,K.Zauberformel “Kompetenz”.In: Vierteljahrsschrift für wissenschaftliche Pädagogik 4(2009),pp.389-412; online: http://homepage.ruhr-uni-bochum.de/klaus.schaller/PdK.htm.
[10]Comenius,J A.De rerum humanarum emendatione consultatio catholica,1645-1670.
[11]Meyer-Drawe,K.Diskurse des Lernens,München 2008.
[12]Meyer-Drawe,K.Vom anderen lernen.In: Borelli,Mi-chele; Ruhloff,Jörg (Hrsg.) Deutsche Gegenwartsp dagogik,Hohengehren,1996,pp.85-98.
[13]Antonsen,S.Safety Culture: Theory,method and impr-ovement,2009.
[14]Deci,E L & Ryan,R M.The “What” and “Why” of Goal Pursuits: Human Needs and the Self-Determination of Behavior,in: Psychological Inquiry,11:4 (2000),pp.227-268.
[15]Lenartz,N.Gesundheitskompetenz und Selbstregulation,Göttingen 2012.
[16]Petzelt,A.Wissen und Haltung.Eine Untersuchung zum Begriff der Bildung,Freiburg 1955.
[17]Schreyögg,G; Eberl,M.Organisationale Kompetenzen.Grundlagen-Modelle-Fallbeispiele.Stuttgart 2015.
[18]Polanyi,M.Implizites Wissen,Frankfurt a.M.,1985 (The tacit dimension 1966).
[19]Lyotard,J-F.Das postmoderne Wissen,Berlin 1986.
[20]Bollmann,U; Franke,Ch.Die Zukunft der Prävention: hinterm Horizont immer weiter-zusammen sind wir stark! Großveranstaltung zeichnet Bild der Zukunft,in: DGUV Forum 7-8/2016 (DE/EN in press).
[21]Hale,A; Borys,D.Working to rule,or working safely? Part 1: A state of the art review,in: Safety Science 55,(2013),pp.207-221.
[22]Weick,K E; Sutcliffe,K M.Das Unerwartete managen.Wie Unternehmen aus Extremsituationen lernen,Stuttgart 2010 (Managing the Unexpected,2001).
[23]Eichendorf,W; Bollmann,U.Future approaches to a culture of prevention,in: From Risks To Vision Zero.Proceedings of the International Symposium on Culture of Prevention-Future Approaches,Helsinki 2014,pp.43-53.
[24]Giebel,D.Integrierte Sicherheitskommunikation.Zur H-erausbildung von Unsicherheitsbewältigungskompetenzen durch und in Sicherheitskommunikation,Berlin 2012.
[25]Kremser,W; Schreyröög,G.The Dynamics of Interrelated Routines: Introducing the Cluster Level,in: Organization Science 27,No 3,May-June 2016,pp.698-721.
[26]Schweer,R; Krummreich,U.Gesundheitskompetenz und Präventionskultur-Indikatoren für Gesundheit und Erfolg in Unternehmen: ein praktisches Handlungsmodell,in: Zeitschrift für Arbeitswissenschaft 63 (2009) No.4,pp.293-302.
[27]Soellner,R; Huber,S; Lenartz,N; Rudinger,G.Facetten der Gesundheitskompetenz-eine Expertenbefragung.Projekt Gesundheitskompetenz,in: Klieme,E.; Leutner,D.; Kenk,M.(Ed.): Kompetenzmodellierung.Eine aktuelle Zwischenbilanz des DFG-Schwerpunktprogramms.Weinheim/Basel 2010,p.104-114.
[28]Nutbeam,D.Health promotion glossary.In: Health Promotion International,Vol 13 (1998),No 4,pp.349-364.
[29]Lenartz,N; Soellner,R; Rudinger,G.Gesundheitskom-petenz.Modellbildung und empirische Modellprüfung einer Schlüsselqualifikation für gesundes Leben,in: DIE Zeitschrift 2014/2,pp.29-32.
[30]Nutbeam,D.The evolving concept of health literacy,in: Social Science and Medicine,67 (2008),pp.2 072-2 078.
[31]Wiencke,M; Cacace,M.& Fischer,S.3 Effects of Practices of Belonging on Accident and Illness Prevention in Small-and Medium-sized Enterprises.In: Healthy at Work-Interdisciplinary Perspectives,Heidelberg/London/New York 2016 (in press).
[32]Konkolewsky,H-H.Report on the results of Topic 2 People centered prevention at the 4th International Strategy Conference on Safety and Health (ISC2016),21-24 March 2016,DGUV Academy Dresden (Best-of-Video),http://www.dguv.de/isc/documentation/index.jsp.
[33]Teigeler,M.Interview at the 4th International Strategy Conference on Safety and Health (ISC2016),21-24 March 2016,DGUV Academy Dresden (Best-of-video),http://www.dguv.de/isc/documentation/index.jsp.
[34]Rosenstiel,L V.Kompetenzen erkennen und entwickeln in der Krise,online: http://www.psy.lmu.de/soz/studium/downloads_folien/ws_09_10/muf_09_10/von_rosenstiel_krise.pdf
[35]Kriegesmann,B; Kottmann,M; Masurek,L; Nowak,U.Kompetenz für eine nachhaltige Beschäftigungsfähigkeit,Bundesanstalt für Arbeitsschutz und Arbeitsmedizin (BAuA),Fb 1038,Berlin 2005.
[36]DGUV.Fachkonzept für die nächste gemeinsame Präve-ntionskampagne der DGUV und ihrer Mitglieder,Sankt Augustin 2015.
[37]DGUV.KulturCheck-Analysis tool for surveying the culture of prevention,Dresden 2016.
[38]Rahnfeld,M; Hessenmöller,A-M; Wetzstein,A.Gut vorbereitet für die neue Präventionskampagne,in: DGUV Forum 7-8/2016 (in press).
[39]Bollmann,U; Otten,E.Lernen als integraler Bestandteil des kulturellen Wandels.Qualifizierungskonzept zur Kampagne Kultur der Prävention,in: DGUV Forum 7-8/2016 (in press).
[40]Senge,P M.Die fünfte Disziplin.Kunst und Praxis der lernenden Organisation,Freiburg 1997 (The Fifth Discipline: The Art and Practice of the Learning Organization,New York 1990).
[41]Kim,Y; Park,J; Park,M.Creating a Culture of Prevention in Occupational Safety and Health Practice,in: Safety and Health at Work 7 (2016),pp.89-96.
[42]Prüße,M; Hemke-Smith,R; Wilhelm,M.Rahmenkonzept “Broschüre” für Klein-& Kleinstbetriebe,2016 (in press).
10.13800/j.cnki.xakjdxxb.2016.0521
1672-9315(2016)05-0741-09
2016-05-10责任编辑:刘洁
BOLLMANN Ulrike,Ph.D.,E-mail:ulrike.bollmann@dguv.de
