锁骨滋养孔解剖学研究
2015-03-16张庆伟
李 京 张庆伟
(济宁医学院基础学院,山东 济宁 272067;济宁医学院临床学院, 济宁 272000)
·基础医学·
锁骨滋养孔解剖学研究
李 京 张庆伟
(济宁医学院基础学院,山东 济宁 272067;济宁医学院临床学院, 济宁 272000)
目的 观察人锁骨滋养孔的形态学特征,进一步丰富与锁骨相关的解剖学知识,为锁骨骨折、骨移植等治疗提供解剖学依据。方法 观察215例(左侧114例,右侧101例)锁骨滋养孔的数量及分布;采用游标卡尺测量滋养孔中心与锁骨胸骨端的距离;根据Hughes公式计算滋养孔指数。结果 具有滋养孔的锁骨共210例:1)含1个孔120例,2个孔64例,3个孔20例,4个孔6例;2)滋养孔位于锁骨中1/3段272例,内侧1/3段23例,外侧1/3段39例;3)滋养孔位于锁骨上面8例,下面108例,前缘7例,后缘211例;4)滋养孔距锁骨胸骨端平均64.3 mm,平均滋养孔指数44.6。结论 锁骨滋养孔多位于锁骨的后缘和下面,锁骨中1/3段;孔的方向自锁骨端至肩峰端;锁骨血供来自滋养孔动脉和骨膜血管网。掌握滋养孔的数量、位置对于手术时保护锁骨的血供具有重要意义。
锁骨;滋养孔;手术
锁骨呈“S”形,为胸、肩部骨骼肌如胸锁乳突肌、三角肌等提供附着点,协调肩关节和胸部运动,是连接上肢与躯干重要的附肢骨。锁骨的中1/3段是锁骨两个反相弯曲相接的部位,骨质较薄且缺少骨骼肌附着,容易发生骨折[1]。锁骨的中1/3骨面具有小孔,孔内含有滋养孔动脉或(和)锁骨上神经[2]。有研究显示[3],锁骨的血供来自锁骨骨膜动脉网,并未发现滋养动脉。Havet等[4]认为锁骨滋养孔多位于锁骨中、外1/3交界区,且锁骨中1/3段的血供来自肩胛上动脉的分支。由此可见,对于锁骨滋养孔所处部位及锁骨血供情况的研究并不十分清楚。本文在观察锁骨滋养孔数量、部位的基础上,探讨锁骨血供来源,为其损伤、治疗提供解剖学依据。
1 资料与方法
1.1 资料
采用解剖学实验室所存的215例人体锁骨标本;游标卡尺(精确度0.02 mm)。
1.2 方法
观察锁骨滋养孔所处的部位及数量;测量滋养孔的中心至锁骨胸骨端的距离(D),测量锁骨的长度(L),根据Hughes公式[5]计算滋养孔指数(foraminal index FI),即FI=D/L×100;将锁骨全长3等分,即内侧、中间及外侧1/3段。依据孔指数判断滋养孔所处的部位。
2 结果
2.1 锁骨滋养孔的数量
具有滋养孔的锁骨共有210例,缺如5例。见表1。
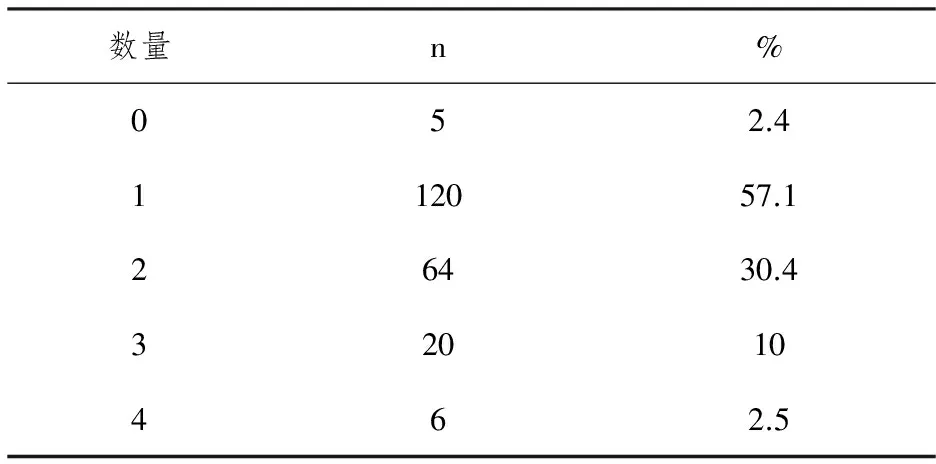
表1 锁骨滋养孔的数量
2.2 锁骨滋养孔的分布
滋养孔位于锁骨中1/3段272例,内侧1/3段23例,外侧1/3段39例。滋养孔的朝向均从胸骨端至肩峰端。滋养孔距锁骨胸骨端平均64.3 mm,平均孔指数44.6。见表2,图1、2。
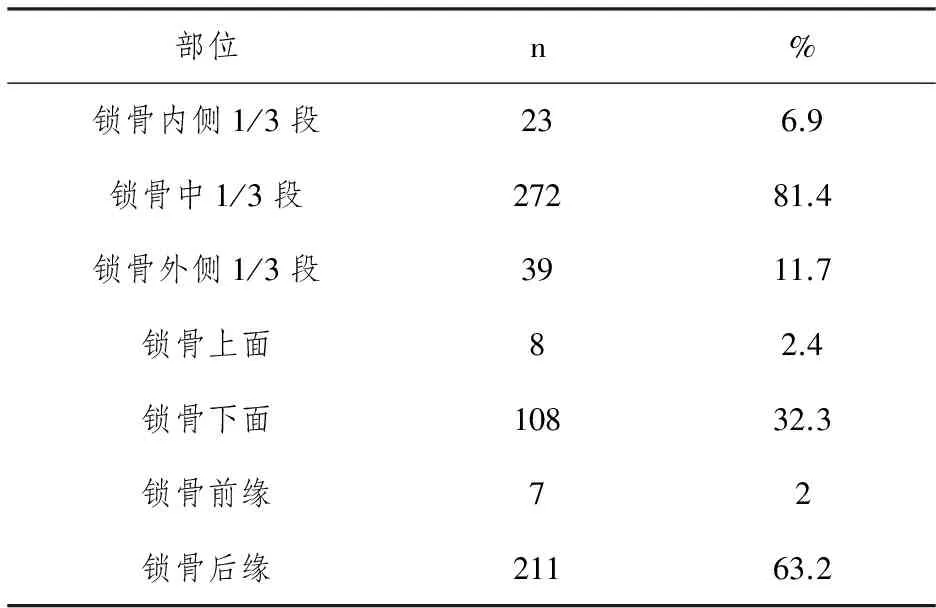
表2 锁骨滋养孔的分布
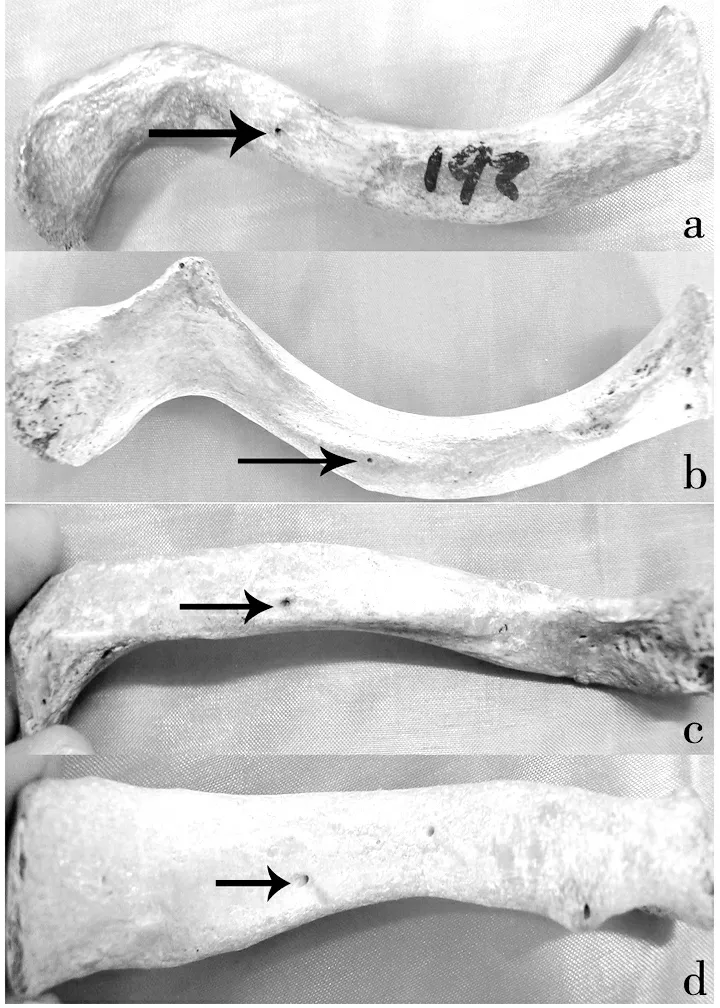
滋养孔位于锁骨a 上面;b 下面;c前缘;d 后缘
图1 锁骨滋养孔位置分布

滋养孔位于锁骨a 内侧1/3段;b 中1/3段;c外侧1/3段
3 讨论
滋养孔动脉是长骨主要的血液来源,在骨的生长和骨化的早期阶段尤为重要[6]。在哺乳动物中,滋养孔的位置和滋养管道的方向会随着骨的生长发生改变[7]。锁骨经原位膜内成骨,第一个完成骨化。当胚胎生长至18 mm,时,在锁骨的内侧2/3和外侧1/3交界区出现2个骨化中心,被软骨帽覆盖[8-9]。膜血管经软骨层向间质骨基质生长,间质骨基质随后逐渐溶解,胚胎长至32 mm时基质消失。发育过程中,在锁骨中段的初级骨化中心和胸骨端的次级骨化中心可能均有动脉发生[3],而骨骺位于锁骨胸骨端,推测锁骨的很可能是从肩峰端向着胸骨端生长。本文观察到,锁骨滋养孔均朝向肩峰端,提示锁骨的胸骨端应是锁骨生长的末端,这与Kumar[2]、Havet[4]的研究结果基本一致,即部分锁骨是由滋养孔动脉供血。除滋养孔动脉,滋养孔中还可能伴随锁骨上神经的内侧分支[2]。当滋养孔动脉缺如时,由于锁骨不含有骨髓腔,其血供并不完全依赖滋养孔动脉[2]。Murlimanju[11]在锁骨的前缘没有观察到滋养孔,而本文发现8例,考虑是其样本量较少的缘故。根据相关参考书[12]的描述,锁骨滋养孔多位于锁骨的下面,本文证实滋养孔多位于锁骨后缘和下面,后缘最多,值得进一步探讨。
大多数学者认为锁骨的血供来自骨膜动脉网。尽管滋养孔内会有动脉通过,锁骨并不完全依赖它。knudson[3]将锁骨下动脉及其分支分别进行灌注,发现锁骨外侧4/5由肩胛上动脉供应,胸肩峰动脉和胸内动脉供应胸骨端1/5;锁骨是由骨膜内的动脉而非滋养动脉供血,滋养孔是静脉回流的通道。Fisher[12]曾描述肩胛上动脉的分支经滋养孔穿入锁骨,在锁骨内分为内、外侧两终支,此滋养动脉是锁骨中1/3段主要的血液来源。Havet[4]对上述分支进行了更深入研究,发现此分支于锁骨中、外1/3交界区穿入锁骨,距肩峰端4.5 cm,骨内分支的长度均<0.5 cm,证实锁骨不具有骨髓腔,锁骨的血供并不完全依赖此动脉,必然与骨膜血管网联系密切。本文观察到5例锁骨存在滋养孔缺失,推测其血供可能来源于骨膜动脉网。
锁骨的中1/3段是常见的损伤部位,占成人骨折的5%~10%[4]。Havet[4]通过对锁骨血供的研究,阐明锁骨骨折不愈合的病例机制和相应的手术方法。在锁骨的上面和前缘始终覆有骨膜动脉,这些血管位于相关骨骼肌附着点之间,当出现骨折或进行骨移植时,可能会造成这些血管的损伤;而锁骨的下面和后缘并没有动脉覆盖。Seikaly[13]对40例胸-肩峰动脉干解剖后发现,锁骨分支伴随三角肌支、胸部肌支共同起自胸-肩峰动脉干约62%;起自三角肌支者约23%;来自胸肩峰动脉干者10%;来自胸部肌支者5%。锁骨分支的直径1~1.5 cm,长度20~50 mm。如果锁骨用作带血管骨移植的材料,应保留供体的胸肩峰血管。如果穿入锁骨内的动脉长度<20 mm,当锁骨骨折伴有不愈合的状况,对骨膜动脉缺乏保护,最好应采用骨移植的治疗手段[4]。某些情况下,肩胛上神经的内侧分支穿过滋养孔后,分布至胸前区[14]。
本文观察锁骨滋养孔的解剖学特征,对教材缺少的内容进行了补充,即锁骨的滋养孔常出现在其下面和后缘,且滋养孔均朝向肩峰端;这进一步丰富骨学知识。锁骨并不完全依赖滋养孔动脉,而是由滋养孔动脉和骨膜动脉网相互补充,这对于外科医生进行锁骨骨折内固定、骨移植及胸锁韧带的修复具有重要意义。
[1] Robinson C M.Fractures of the clavicle in the adult.Epidemiology and classification[J].J Bone Joint Surg Br,1998,80(3):476-484.
[2] Kumar R,Lindell M M,Madewell J E,et al.The clavicle:normal and abnormal[J].Radiographics,1989,9(4):677-706.
[3] Knudsen F W,Andersen M,Krag C.The arterial supply of the clavicle[J].Surg Radiol Anat,1989,11(3):211-214.
[4] Havet E,Duparc F,Tobenas-Dujardin A C,et al.Vascular anatomical basis of clavicular non-union[J].Surg Radiol Anat,2008,30(1):23-28.
[5] Hughes H.The factors determining the direction of the canal for the nutrient artery in the long bones of mammals and birds[J].Acta Anat,1952,15(3):261-286.
[6] Kizilkanat E,Boyan N,Ozsahin E T,et al.Location,number and clinical significance of nutrient foramina in human long bones[J].Ann Anat,2007,189(1):87-95.
[7] Henderson R G.The position of the nutrient foramen in the growing tibia and femur of the rat[J].J Anat,1978,125(Pt3):593-599.
[8] Cadilhac C,Fenoll B,Peretti A,et al.Congenital pseudarthrosis of the clavicle:25 childhood cases[J].Rev Chir Orthop Reparatrice Appar Mot,2000,86(6):575-580.
[9] Hirata S,Miya M,Mizumo K.Congenital pseudarthrosis of the clavicle:histologic examination for the etiology of the disease[J].Clin Orthop Relat Res,1995,315:242-245.
[10] Murlimanju B V,Prabhu L V,Pai M M,et al.Neurovascular foramina of the human clavicle and their clinical significance[J].Surg Radiol Anat,2011,33(8):679-682.
[11] Standring S.Gray’s anatomy[M].39th.The anatomical basis of clinical practice,edn.Churchill Livingstone,Spain,2006:817-818.
[12] Fischer L P,Carret J P.Arterial vascularization of human bones[J].Bull Assoc Anat (Nancy),1978,62(179):419-452.
[13] Seikaly H,Calhoun K,Rassekh C H,et al.The clavipectoral osteomyocutaneous free flap[J].Otolaryngol Head Neck Surg,1997,117(5):547-554.
[14] Rockwood C A,Matsen F A,Lippitt S B,et al. The shoulder[M],4th edn.Saunders Elsevier,Philadelphia,2009:77.
An anatomical study of neurovascular foramina of the human clavicle and their clinical significance
LIJing,ZHANGQingwei
(School of Basic Sciences,Jining Medical University,Jining 272067,China)
ObjectiveTo study the topographic anatomy and morphology of neurovascular foramina of the human adult clavicles.MethodsIn the present study 215 dry human clavicles was performed.The clavicles were macroscopically observed for the number,location and direction of the nutrient foramina.The foraminal index was calculated for each clavicle by applying the Hughes formula.ResultsThe neurovascular foramen was observed in 210 (97.6%) clavicles.The foramen was single in 120 (57.1%) clavicles,double in 64cases (30.4%),and there were more than 2 foramina in 26 clavicles (12.5%).The foramen was present at the middle 1/3 region in 82% of clavicles,at the medial 1/3 region in 7% and at the lateral 1/3 part in 11.7% of clavicles.It was on the inferior surface in 32.3% of clavicles,on the posterior surface in 63.2%,on the anterior surface in 2% and at the superior surface in only 2.4% of clavicles.The average distance of the foramen from the sternal end was 64.3 mm and the mean foraminal index was 44.6.ConclusionThe foramina were more common on the posterior surface which were often multiple,directed toward the acromial end.Knowledge of the localization of nutrient foramina can be useful in certain surgical procedures to preserve blood supply.The data obtained from the present study would be of interest to clinicians who are involved in procedures such as bone grafting,surgical approach for internal fixation and coracoclavicular ligament repair.
Clavicle;Neurovascular Foramina;Anatomy;Surgery
* [基金项目]2013年济宁医学院科研计划项目(编号:JY2013KJ014)
10.3969/j.issn.1000-9760.2015.06.003
R322.7
A
1000-9760(2015)12-397-03
2015-09-09)
