Case-control study of changes in bone mineral density in drug-naïve Patients in the first-ePisode of schizoPhrenia during the first year of treatment with risPeridone
2011-07-18XiaoyiLIHongCHENXingliCHENFangzhongXUBaopingXING
Xiaoyi LI,Hong CHEN,Xingli CHEN,Fangzhong XU,Baoping XING
·Research Article·
Case-control study of changes in bone mineral density in drug-naïve Patients in the first-ePisode of schizoPhrenia during the first year of treatment with risPeridone
Xiaoyi LI,Hong CHEN,Xingli CHEN,Fangzhong XU,Baoping XING*
Background:The long-term effect of risperidone treatment on bone mineral density remains unclear.
HyPothesis:Long-term treatment with risperidone in patients with schizophrenia has adverse effects on bone mineral density.
Methods:28 drug-naïve patients in their first episode of schizophrenia(diagnosed according to Chinese diagnostic criteria)were treated with risperidone for a one-year period.Bone density assessments reported as T-values(that compare the subject’s bone density to a reference value for young persons of the same gender and race)were made at baseline and at 3,6 and 12 months after initiating treatment.Bone density measurements were also conducted in 32 healthy control subjects at the time of enrollment and 1 year after enrollment.
Results:There were no statistically significant differences in the age,gender or bone density of patients and controls at the time of the baseline assessment,but after 12 months the decrease in bone density in the patient group (who received risperidone treatment)was significantly greater than in the control group(F=15.21,P<0.001).In the patient group there was a non-significant gradual drop in bone mineral density during the first six months of treatment and a statistically significant rapid drop during the second six months of treatment.Among the 20 patients who completed 12 months of risperidone treatment,1(5%)met WHO criteria for osteoporosis and another 8 (40%)meet WHO criteria for bone mass loss.
Conclusion:Long-term treatment with risperidone in patients with schizophrenia is associated with reduced bone mineral density.The most pronounced drop in bone density occurs after six months of treatment so follow-up studies that last less than one year may not identify clinically important changes in bone mineral density associated with use of antipsychotics medications.
Risperidone;Schizophrenia;Bone mineral density
1 Introduction
The risk of non-violent fractures in patients with schizophrenia is increased by 3.8-fold but the reasons for this increase remain uncertain[1].Factors that may be related to this problem include high levels of smoking,decreased activity,decreased exposure to sunlight,neuroendocrine and immunological dysfunction,and increased prolactin secondary to prolonged usage of antipsychotic medication[1-7].But most of the studies that consider this issue are cross-sectional assessments of patients who have used antipsychotic medications prior to the initiation of the study[2].The current study is a one-year follow-up study of drug-naïve,firstepisode patients with schizophrenia treated with risperidone—a second-generation antipsychotic associated with elevated serum prolactin.
2 Subiects and Methods
2.1 Subiects
First-episode patients with schizophrenia(as defined by the third edition of the Chinese Classification of Mental Disorders[8]—which only requires 1 month of acute psychotic symptoms)who meet the following criteria were included:1)outpatients or inpatients at Tongde Hospital in Hangzhou,Zhejiang from January 2009 to December 2010;2)30-4 5 years of age;3)no serious physical disease,endocrine disorders,metabolic disorders,or diseases of the skeletal system;4)not bed-ridden;5) non-smoker;6)does not use vitamins,hormones,or nutrient supplements;7)no previous treatment with antipsychotic medications;and 8)both patient and accompanying family member provide written informed consent.
Healthy controls were recruited among community members 30-45 years of age who received their regular annual physical examination at the Tongde Hospital.They meet the same criteria as the patients(above)except that they had no previous or current evidence of a mental illness.
This study was approved by the ethics committee of the Tongde Hospital.
2.2 Methods
All enrolled patients in the schizophrenia group were treated with monotherapy risperidone (2-6mg/d).No other antipsychotics were used but benzodiazepines could be added to the drug regimen to treat insomnia or agitation and trihexyphenidyl could be added to treat extrapyramidal side effects.
Patients’bone density was assessed four times (at baseline and 3,6,and 12 months after the start of treatment);control subjects’bone density was assessed at baseline and 1 year after baseline.The bone density of subjects’lumbar spine was assessed using the dual-energy LUNAR Prodigy X-ray bone density detector(manufactured by the General Electric Company,USA).The instrument provides a T-value which compares the assessed bone density with reference values for young persons of the same gender and race.Based on standards recommended by the WHO[9],T-values>-1 indicate normal density,values between-2.5 and-1 indicates bone mass loss,and values<-2.5 indicate osteoporosis.
The dual-energy X-ray bone mineral density test is convenient,safe,rapid and non-invasive.Its accuracy and precision are good so it has become the gold standard for the clinical diagnosis of osteoporosis.Each examination results in a radiological exposure of 0.001 mSV(equivalent to about one day exposure to sunlight)so the maximum of four assessments in this study resulted in an exposure of 0.004 mSV—a very small proportion of the annual maximum recommended exposure for China of 1 mSV.
2.3 Statistical analysis
Version 9.2 SAS software was used in the analysis.The T-value parameter used to assess bone mineral density is not normally distributed so nonparametric tests were employed to compare median T-values between groups and over time.Comparison of baseline values between the two groups used the Mann-Whitney test,comparison of beforeversus after values in the control group used Wilcoxon signed ranked tests,and comparisons over the four time periods in the patient group and between the patient and control group were conducted using repeated measures analysis of the normalized rank transformation of the T-value(using the SAS PROC RANK procedure).All tests were two-tailed and the level of statistical significance was set at P<0.05.
3 Results
3.1 SamPle characteristics
The enrollment and follow-up of patients is shown in Figure 1.Twenty-eight patients with firstepisode schizophrenia were enrolled:they included 14 males and 14 females,had a mean(SD)age of 35.3(6.8)years,a mean duration of illness of 3.4 (1.8)months and had a mean total score on the Positive and Negative Syndrome Scale(PANSS)of 90.4(24.7).Eight patients(29%)changed medication,withdrew consent,or were lost to follow-up over the one-year follow-up(see Flowchart for details).The 32 control subjects included 16 males and 16 females;their mean age was 34.6(6.6) years.Two control subjects(6.3%)were lost to follow-up over the 1-year period.The gender ratio and mean age in the two groups of subjects were not significantly different.
3.2 ComParison of bone mineral density between the healthy control grouP and the schizoPhrenia Patient grouP at different time Points
Table 1 presents the results of the bone mineral density assessments.At baseline(that is,before patients started medication)the bone density in the patient group and control group were not significantly different(Mann-Whitney test Z=0.92,P= 0.361).The slight drop in bone mineral density in the control group from baseline to 12-month follow-up was not statistically significant(Wilcoxon signed rank test T=1.50,P=0.052).In the patient group the overall drop in bone mineral density over the 12-month period was statistically significant(F= 9.91,P<0.001)and was significantly greater than the drop in the control group(F=15.21,P<0.001).In the patient group the gradual decline in bone mass during the first six months of treatment was not statistically significant(F=2.30,P= 0.133)but the precipitous decline during the second six months of treatment was statistically significant(F=12.06,P<0.001).
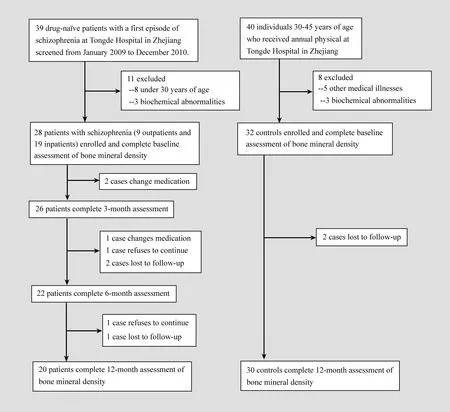
Figure 1.Flowchart for the study

Table 1.Median(interquartile range,IQR)T-value#for bone mineral density at different time Points between the schizoPhrenia Patient grouP and the healthy control grouP
At baseline none of the patients or controls met WHO criteria of low bone mass(-2.5<T<-1) or osteoporosis(T<-2.5).None of the controls met either criteria 12 months after enrollment. None of the patients met criteria of low bone mass or osteoporosis after 3 months or 6 months of treatment,but after one year 40%(8/20)of the patients who completed 12 months of risperidone treatment met criteria for low bone mass and 1 (5%)met criteria for osteoporosis.
4 Discussion
4.1 Main findings
This is the first study we are aware of that assessed changes in bone mineral density during the first year of treatment with risperidone in patients with schizophrenia who had been drug-naïve prior to the initiation of the treatment.
This study found no differences in bone mineral density between untreated patients with schizophrenia and normal controls,suggesting that schizophrenia does not,in itself,affect bone mass.This result contradicts the findings of cross-sectional studies[4]that report significantly lower bone mineral density,bone linear density and bone area density in patients with schizophrenia compared to normal controls.There are two possible explanations for these contradictory results:either the previous studies were confounded by the use of antipsychotic medications in the patient group(leading to lower T-values),or the duration of illness at the time of enrollment in our study(a mean of 3.4 months) was too short for the latent effect of schizophrenia on bone density to be evident.Studies with drug-naïve patients with schizophrenia who had longer pretreatment intervals would be needed to resolve this issue.
This case control study also found an unequivocal stepwise drop in bone mineral density over the first year of treatment with risperidone in previously drug-naïve patients with schizophrenia.This result confirms previous studies[5,7]that report an association between decreased bone mineral density and the use of a variety of first-generation and secondgeneration antipsychotic medications;it also confirms previous reports of lower bone density in patients who have used the medications longer.Most of these previous reports[1,7,10-12]suggest that increased prolactin is the intermediate factor that directly results in osteoporosis,increased bone fragility and liability to fracture.
The slow decline in bone density in the first six months of treatment followed by a much more rapid decline in the second six months of treatment was an unexpected finding that has not been reported previously,possibly because most prior studies involve patients who had previously used antipsychotic medications.This finding has important implications both clinically and in research.These latent effects of antipsychotic medications could easily be missed,so clinicians need to remain vigilant about decreased bone mass throughout the long course of treatment.And studies about the relationship of medications on bone mass must continue for at least one-year:shorter studies could fail to identify important relationships.This result also raises questions about the exact mechanism that connects medication usage and loss of bone mass:why does the demineralization process accelerate after six months of treatment?Do changes in prolactin levels follow a similar time course?
None of the relatively young patients with schizophrenia in the study had abnormal bone mineral density prior to staring the medication but 1 of the 20 patients(5%)who completed one year of treatment with standard doses of risperidone met WHO criteria for osteoporosis and another 8 patients(40%)met WHO criteria of bone mass loss. Most patients with schizophrenia(and many patients with other diagnoses)use antipsychotic medication for many years so the cumulative negative impact on overall health of bone mass loss,osteoporosis and the associated elevated risk for nonviolent fractures is considerable.Thus this change in bone density is much more than an altered laboratory value:it is a serious iatrogenic health problem in patients with schizophrenia that is under researched,under identified,and under treated.
Further research needs to 1)follow patients for longer periods to see if the drop in bone density continues or stabilizes over time;2)compare the effects of different medications on bone density in drug-naïve,first-episode patients;3)assess the timing and degree of recovery of bone mass with changes or termination of drug treatment;4)simultaneously assess changes in prolactin to assess the causal direction of the relationship between prolactin,medication,and bone density;5)identify risk factors that increase the likelihood of bone mass loss in persons taking antipsychotic medications:and 6)test the effectiveness of preventive interventions such as administering calcium agents and instituting lifestyle changes.
4.2 Limitations
The sample size was too small to adjust the results by gender,age,duration of untreated psychosis,total dosage of anti-psychotic medication,and lifestyle factors(smoking,alcohol use,exercise and so forth)so it is uncertain whether or not these potential confounders affected the results.The small number of subjects also made it impossible to identify the risk factors(if any)that increased the likelihood of bone mass loss with antipsychotic treatment.
In order to match the age of the patient group with that of the available controls—persons who received annual physical examinations at a general hospital—we limited the age range of patients to 30-45 years of age.This meant that the mean age of onset in the patient group(35)was higher than is typical for schizophrenia.Additional study will be needed to confirm the identified medication-related changes in bone mineral density among younger patients with schizophrenia.
The 29%drop-out rate in the patient group may seem high but this means that 71%of firstepisode patients stayed on the initially prescribed antipsychotic medication for a full year,which is a much higher retention rate than reported in treatment studies in other countries[13].It is,moreover,unlikely that the reasons for discontinuing the risperidone or being lost to follow-up was related to bone mineral density so it is unlikely that these dropouts affected the overall conclusions.
4.3 ImPlications
Loss of bone mass is a common latent side effect of prolonged use of antipsychotic medication.This is a serious condition that can predispose patients to osteoporosis and fractures so clinicians need to periodically monitor bone mineral density in patients taking antipsychotics(regardless of diagnosis),particularly in elderly patients who are,by virtue of their age,at increased risk of osteoporosis. The relative risk for bone mass loss of different antipsychotic medications remains uncertain but it isreasonable to assume that medications which have a more pronounced effect on prolactin levels will be associated with greater losses in bone density. Nor is it known which types of patients are at greatest risk of bone mass loss with antipsychotic treatment,so clinicians should advise all patients and family members about this potential complication. If patients have continuing declines in bone density despite use of calcium supplements and recommended changes in lifestyle(e.g.,decrease smoking and alcohol consumption and increase exercise),clinicians should consider changing the antipsychotic regimen.
Conflict of interest
The authors report no conflict of interest in the preparation of this paper.
Funding
This project was supported by the Zhejiang Provincial Fund for Scientific Research in Health (project number:2009A034).
1. Howard L,Kirkwood G,Leese M.Risk of hip fracture in patients with a history of schizophrenia.Br J Psychiatry,2007,190:129-134.
2. Becker D,Liver O,Mester R.Rapoport M,Weizman A,Weiss M,Risperidone,but not olanzapine,decreases bone mineral density in female premenopausal schizophrenia patients.J Clin Psychiatry,2003,64(7):761-766.
3. Halbreich U.Osteoporosis,schizophrenia and antipsychotics:the need for a comprehensive multifactorial evaluation.CNS Drugs,2007,21(8):641-657.
4. Ma WY,Sun HX,Zhang B,Yu ZJ,Zhang SH,Peng JF,et al. Control study of bone mineral density in patients with schizophrenia.Journal of Qiqihar Medical College,2006,27(1):15. (in Chinese)
5. Bilici M,Cakirbay H,Guler M,Tosun M,Ulgen M,Tan U. Classical and atypical neuroleptics,and bone mineral density,in patients with schizophrenia.Int J Neurosci,2002,112(7):817-828.
6. Yuan W,Dang J.Antipsychotics and osteoporosis(Analysis of 10 Cases).Journal of Clinical Psychiatry,2006,16(5):268. (in Chinese)
7. Graham SM,Howgate D,Anderson W,Howes C,Heliotis M,Mantalaris A,et al.Risk of osteoporosis and fracture incidence in patients on antipsychotic medication.Expert Opin Drug Saf,2011,10(4):575-602.
8. Chinese Society of Psychiatry.Chinese Classification of Mental Disorders,Third Edition(CCMD-3).Jinan:Shandong Science &Technology Press.2001.(in Chinese)
9. World Health Organization:Guidelines for Preclinical Evaluation and Clinical Trials in Osteoporosis.Geneva,WHO,1998:5-6.
10. Howes O.Bone mineral density and prolactin associations in patients with chronic schizophrenia.Schizophr Res,2004,66 (1):77-78.
11. Stubbs B.Antipsychotic-induced hyperprolactinaemia in patients with schizophrenia:considerations in relation to bone mineral density.J Psychiatr Ment Health Nurs,2009,16(9):838-842.
12. Hu JM,Li Y,Li T,Wang HM,Liu XH,Huo KJ.The effects of antipsychotics on serum prolactin in the first-episode schizophrenia patients.West China Journal of Pharmaceutical Sciences,2003,18(6):467-469.(in Chinese)
13. McEvoy JP,Lieberman JA,Perkins DO,Hamer RM,Gu H,Lazarus A,et al.Efficacy and tolerability of olanzapine,quetiapine,and risperidone in the treatment of early psychosis:a randomized,double-blind 52-Week comparison.Am J Psychiatry,2007,164(7):1050-1060.
利培酮治疗首发精神分裂症患者1年骨密度变化的病例对照研究
李晓一 陈 虹 陈杏丽 徐方忠 邢葆平
浙江省立同德医院精神科310012。通信作者:邢葆平,电子信箱2001life@163.com
背景长期非典型抗精神病药利培酮治疗对骨密度的影响尚不清楚。
假设长期利培酮治疗会对精神分裂症患者的骨密度有不利影响。
方法28例符合中国精神障碍分类与诊断标准的首发精神分裂症患者接受1年的利培酮治疗,分别于服药前及服药后第3、6、12月进行骨密度检测,结果以T值来表示。设立32例年龄、性别和种族匹配的健康对照,于入组时和1年后进行骨密度检测。
结果基线时,首发精神分裂症组的年龄、性别以及骨密度与健康对照组之间的差异无统计学意义。与对照组相比,接受利培酮治疗12个月的精神分裂症组的骨密度降低(F=15.21,P<0.001)。精神分裂症组利培酮治疗的前6个月内骨密度下降无统计学差异,在利培酮治疗的后6个月内骨密度显著下降。在20例完成12个月利培酮治疗的患者中,分别有1例(5%)和8例(40%)符合世界卫生组织关于骨质疏松和骨量减少的标准。
结论长期的利培酮治疗可能会降低精神分裂症患者的骨密度,这种骨密度变化在治疗6个月后最明显。因此,少于1年的随访往往无法发现这种与抗精神病药治疗相关的骨密度变化。
利培酮 精神分裂症 骨密度
date:2011-06-27;accepted date:2011-09-07)
10.3969/j.issn.1002-0829.2011.05.004
Zhejiang Province Mental Health Research Institute,Department of Psychiatry,Tongde Hospital,Hangzhou,Zhejiang,310012 China*Correspondence:2001life@163.com
·论著·
猜你喜欢
杂志排行

上海精神医学的其它文章
- 精神分裂症的全基因组关联分析研究
- ComParison of the neuroPsychological characteristics of two subtyPes of mild cognitive imPairment
- Randomized controlled trial comParing quetiaPine with lithium and clozaPine with lithium in the treatment of female Patients with mania
- Changes in the level of micro RNA-206 gene exPression in Patients with tyPe I biPolar disorder before and after treatment and comParison with a control PoPulation
- Differences in the levels of suPeroxide dismutase and brain-derived neurotroPhic factor in first-ePisode schizoPhrenia,chronic schizoPhrenia and normal control subiects
- Binary outcome variables and logistic regression models